Selecfed METABOLIC RESPONSES to SKATEBOARDING
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Skateboarding
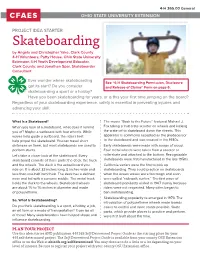
4-H 365.00 General OHIO STATE UNIVERSITY EXTENSION PROJECT IDEA STARTER Skateboarding by Angela and Christopher Yake, Clark County 4-H Volunteers; Patty House, Ohio State University Extension 4-H Youth Development Educator, Clark County; and Jonathan Spar, Skateboarder Consultant Ever wonder where skateboarding See “4-H Skateboarding Permission, Disclosure got its start? Do you consider and Release of Claims” Form on page 6. skateboarding a sport or a hobby? Have you been skateboarding for years, or is this your first time jumping on the board? Regardless of your skateboarding experience, safety is essential in preventing injuries and advancing your skill. What Is a Skateboard? The movie “Back to the Future” featured Michael J. When you look at a skateboard, what does it remind Fox taking a fruit crate scooter on wheels and kicking you of? Maybe a surfboard with four wheels. While the crate off to skateboard down the streets. This waves help guide a surfboard, the rider’s feet apparatus is commonly accepted as the predecessor help propel the skateboard. You can travel short to the skateboard and was created in the 1930s. distances on them, but most skateboards are used to Early skateboards were made with scraps of wood. perform stunts. Four metal wheels were taken from a scooter or Let’s take a closer look at the skateboard. Every rollerskate and attached to the bottom. Recognizable skateboard consists of three parts: the deck, the truck skateboards were first manufactured in the late 1950s. and the wheels. The deck is the actual board you California surfers were the first to pick up ride on. -

MEMORANDUM – JABSOM Skateboard, Bicycle and Surfboard Policy the University Has an Obligation to Provide a Safe Environment An
MEMORANDUM – JABSOM Skateboard, Bicycle and Surfboard Policy The University has an obligation to provide a safe environment and protect University property. JABSOM recognizes that students, faculty, and staff use a variety of means of transportation on campus. Although personal choice is important, JABSOM must consider the safety and well‐being of the campus community and our visitors as well as JABSOM property. Activities that include skateboarding may cause damage to sidewalks. In addition, there is a potential for injury to both the person doing the activity and the public at large. In an effort to balance our concern for community safety and the ability to use these means of transportation, the following policy applies to the use of bicycles and skateboards on campus (policies applicable to skateboards apply to roller‐skates and in‐line skates). Skateboarding, conducted in a reckless manner can be dangerous and presents a safety issue for pedestrians, as well as the skate boarder. Skateboarding has also caused significant damage to benches, walls, steps, curbs, and receptacles around campus. Nevertheless, skateboarding, when good judgment is exercised is an effective means to travel in urban areas. Skateboard (as well as roller skates and rollerblades) and bicycle use on JABSOM premises is allowed. However, it is the person on the skateboard or bicycle that is responsible for avoiding pedestrians and not the other way around. The use of these items, involves an assumption of personal risk. Persons who use them are personally liable for their actions Skateboards and bicycles shall be used solely to convey a person and shall not be used to perform tricks or carryout reckless or risky actions such as riding on ledges or using on steps. -

Chapter 430 BICYCLES, SKATEBOARDS and ROLLER SKATES
Chapter 430 BICYCLES, SKATEBOARDS AND ROLLER SKATES § 430.01. Definitions. [Ord. No. 458, passed 2-25-1991; Ord. No. 535, passed 7-8-1996] The following words, when used in this chapter, shall have the following meanings, unless otherwise clearly apparent from the context: (a) BICYCLE — Shall mean any wheeled vehicle propelled by means of chain driven gears using footpower, electrical power or gasoline motor power, except that vehicles defined as "motorcycles" or "mopeds" under the Motor Vehicle Code for the State of Michigan shall not be considered as bicycles under this chapter. This definition shall include, but not be limited to, single-wheeled vehicles, also known as unicycles; two-wheeled vehicles, also known as bicycles; three-wheeled vehicles, also known as tricycles; and any of the above-listed vehicles which may have training wheels or other wheels to assist in the balancing of the vehicle. (b) SKATEBOARD — Shall include any surfboard-like object with wheels attached. "Skateboard" shall also include, under its definition, vehicles commonly referred to as "scooters," being surfboard-like objects with wheels attached and a handle coming up from the forward end of the surfboard area. (c) ROLLER SKATES — Shall include any shoelike device with wheels attached, including, but not limited to, roller skates, in-line roller skates and roller blades. § 430.02. Operation upon certain public ways prohibited; sails and towing prohibited. [Ord. No. 458, passed 2-25-1991; Ord. No. 677, passed 12-8-2003] (a) No person shall ride or in any manner use a skateboard, roller skate or roller skates upon the following public ways: (1) U.S. -
HOBIE KA Y AKING + F I S HING C O Ll EC T
HOBIE KAYAKING + FISHING COLLECTION HOBIE HISTORY 1994 The Hobie Float Cat 1984 marked the company’s The windsurfing scene first cast into angling. was exploding and Hobie contributed 1987 by distributing Alpha Ladies love watersports, 1968 1977 . so Hobie delivered After ample hands-on Seeking all-out speed, Sailboards fashion-forward, R&D, Hobie introduced a the Hobie 18 delivered functional lightweight, beachable serious velocity thrills to women’s . sailing catamaran, the sailors worldwide. swimwear Hobie 14. 1958 Hobie teamed up 1950 with Grubby Clark to Hobie Alter shaped produce the world’s 1994 The Hobie Wave was his first surfboard in first fiberglass-and- designed and crafted his parents’ Laguna foam-core boards, as the perfect, simple, Beach garage. revolutionizing surfing. 1982 rotomolded catamaran. Reading the water is tricky, but Hobie tamed reflected light with its line 1986 Pursuing new ways of polarized sunglasses. to play, Hobie intro- 1966 1974 duced its first kayak, Recognizing that Introduced the the Alpha Wave Ski. people needed Hobie Hawk remote better-quality, sport- controlled glider. specific clothing, Hobie started selling his now-iconic line of sportswear. 1954 1962 Demand for Hobie’s After witnessing the birth boards spiked, so he of skateboarding, Hobie opened his first Surf introduced polyurethane 1970 Shop in Dana Point, skateboard wheels—the Classic. The two-person, 1982 1985 1987 California. sport’s biggest evolution. double-trapeze Hobie 16 The Hobie 33, the The Hobie 17 redefined The Hobie 21 was became an international fastest, sleekest one-person multihulls, bigger, faster, and sensation, instantly sparking monohull in its class. -

CHILD SKATEBOARD and SCOOTER INJURY PREVENTION Suggested Citation
Safekids New Zealand Position Paper: CHILD SKATEBOARD AND SCOOTER INJURY PREVENTION Suggested citation Safekids New Zealand (2012) Safekids New Zealand Position Paper: Child skateboard and scooter injury prevention. Auckland: Safekids New Zealand. If you use information from this publication please acknowledge Safekids New Zealand as the source. Safekids New Zealand 5th Floor, Cornwall Complex, 40 Claude Road, Epsom, Auckland 1023 PO Box 26488, Epsom, Auckland 1344 New Zealand P. +64 9 630 9955 F. +64 9 630 9961 Disclaimer Safekids New Zealand has endeavoured to ensure material in this document is technically accurate and reflects legal requirements. However, the document does not override legislation. Safekids New Zealand does not accept liability for any consequences arising from the use of this document. If the user of this document is unsure whether the material is correct, they should make direct reference to the relevant legislation and contact Safekids New Zealand. Published 2013 If you have further queries, call the Safekids New Zealand Information & Resource Centre on +64 9 631 0724 or email us at [email protected]. This document is available on the Safekids New Zealand website at www.safekids.org.nz Sponsored By This Safekids New Zealand position paper on skateboard and scooter injury prevention was made possible thanks to Jetstar's Flying Start Programme grant. Photo shows Jetstar's Captain Richard Falkner, Safekids Director Ann Weaver, Jetstar Ambassador Steve Price and children from Vauxhall Primary School. Safekids New Zealand Position Paper: Child skateboard and scooter injury prevention 1 Safekids New Zealand Position Paper: CHILD SKATEBOARD AND SCOOTER INJURY PREVENTION Summary Skateboards and non-motorised kick scooters provide Helmets children with a valuable form of exercise and transport. -

Literature Review of Bicycle and E-Bike Research, Policies & Management
Literature Review Recreation Conflicts Focused on Emerging E-bike Technology December 19, 2019 Tina Nielsen Sadie Mae Palmatier Abraham Proffitt Acknowledgments E-bikes are still a nascent technology, and the research surrounding their use and acceptance within the recreation space is minimal. However, with the careful and constructive guidance of our consultants, the report outline morphed into chapters and, eventually, into a comprehensive document. We are deeply indebted to Mary Ann Bonnell, Morgan Lommele, and Stacey Schulte for guiding our thinking and research process and for supplementing our findings with resources and other support. We would like to express our deep appreciation to Lisa Goncalo, Tessa Greegor, Jennifer Alsmstead, and Rick Bachand for their careful and thoughtful reviews. Your gracious offer of time and knowledge was invaluable to our work. We also wish to acknowledge the help of Kacey French, John Stokes, Alex Dean, June Stoltman, and Steve Gibson for their consideration and continued interest in the process. Thanks are also due to colleagues at the Boulder County Parks & Open Space and Boulder County Transportation Departments, who offered their expertise at crucial moments in this process. We would like to offer our special thanks to Bevin Carithers, Pascale Fried, Al Hardy, Eric Lane, Tonya Luebbert, Michelle Marotti, Jeffrey Moline, Alex Phillips, and Marni Ratzel. None of this work would have been possible without the generous financial support from the City of Boulder, City of Fort Collins, and Larimer -

The .Pdf File
Bicycle Helmet Safety Institute Helmets.org 4611 Seventh Street South, Arlington, VA 22204-1419 703-486-0100 www.helmets.org [email protected] Helmet Program Toolkit October 6, 2020 Contents Program Resources Folded Pamphlet Duplicating Masters • Helmet Program Resources • Buyer’s Guide To Bicycle Helmets • Helmet Fact Sheet • A Bicycle Helmet for My Child • Where to Find Funding • How to Fit a Bicycle Helmet • Inexpensive Helmets • Skateboard Helmets • Videos and Films • Public Service Announcements • Child Bike Safety Talk Flat Pamphlet Duplicating Masters • Workshop on Bicycle Helmets • The Correct Way to Fit Your Helmet • Speaker's outline for a bike helmet talk • Helmet Fit Checklist • US DOT materials on your CD • Spanish helmet fit sheet – DOT • Spanish Language Materials • Traffic Safety Facts: Bicyclists • Helmets in Poor Neighborhoods • How to Inspect a Bike Helmet • Common Bicycle Collisions Basic Info • Bicycle Safety Tips • Helmets Made Simple • Frequently Asked Questions • Costs of Head Injury/Benefit of Helmets Other Handouts • Helmets and Playgrounds Don’t Mix! • Which Helmet for Which Activity • Medical Journal Articles • Bookmarks to print and cut • Helmet Standards • Word Game and Tongue Twisters • Helmets for the Current Season • A Maze and Connect-the-Dots • Consumer Reports Helmet Article • A Coloring Page • Mandatory Helmet Laws • A Four-Page Coloring Book CD and DVD’s • CD : BHSI Web site, pamphlet files, lesson plans, WABA safety site, rodeo guide. • DVDs : Helmet and bike safety videos Paper version is printed on 100% post-consumer content recycled paper. Helmets.org The Bicycle Helmet Safety Institute A consumer-funded program 4611 Seventh Street South, Arlington, VA 22204-1419 703-486-0100 www.helmets.org [email protected] October, 2020 Helmet Program Resources Dear Educator or Program Planner: In response to your request, here is information on helmets and helmet promotion campaigns. -

21 Years of St Ke
2019 PRE-BOOK CATALOG 21 YEARS OF ST KE It all started one summer in 1996 with two surfers from Venice, California. They wanted to surf the warm waters of the Venice Breakwater, but it was as flat as a lake. So like the many generations before them, they took to the streets with skateboards in search of hills to surf. As they dropped in on those asphalt waves, they were struck with how unlike surfing the experience was. They really missed the snap and drive of the modern surfboard, with that pivot from the tail that lets you pump a wave for speed, and cut back into the pocket. They were left only imagining the performance they wanted, unable to get that feeling with any skateboard on the market. After experimenting with many new designs and dozens of prototypes, Carver made its first production trucks. Today, after 21 years of continuous innovation, Carver is proud to continue to lead the revolution in surfskate and provide that stoke to a new generation of riders from around the globe. 19. PRE-BOOK 31.5” ORIGIN Carver started with the sea, and with the joy of sliding on the face of a wave. But we are also surrounded by an abundance of municipally made inclined surfaces, our ‘waves by proxy’, so we slide across all this cement on watery bearings, capturing a similar kind of potential energy. Surfing inspired Carver’s innovative skateboard trucks, and now 21 years later we celebrate the true origin of our stoke; the wave and the process of its creation. -

Women in Skateboarding and Product Development 1
WOMEN IN SKATEBOARDING AND PRODUCT DEVELOPMENT 1 Women in Skateboard and Product Development by Griffin Carlborg An honors thesis submitted in partial fulfillment of the requirements for the degree of Bachelor of Science Undergraduate College Leonard N. Stern School of Business New York University May 2017 Professor Marti G. Subrahmanyam Professor Adam Alter Faculty Adviser Thesis Adviser WOMEN IN SKATEBOARDING AND PRODUCT DEVELOPMENT 2 Table of Contents Abstract ............................................................................................................................... 3 Women in Skateboarding and Product Development ........................................................ 4 Chapter 1: Sun Kissed Surfer Boys .................................................................................... 5 Chapter 2: A Boys Club ...................................................................................................... 8 Chapter 3: No Support for Girls........................................................................................ 12 Chapter 4: Potential Success for Female Specific Products ............................................. 16 Chapter 5: The Female Foot ............................................................................................. 18 Chapter 6: Implications and Feasibility of Gender Specific Products in Action Sports ... 22 Chapter 7: Steps Necessary to Yield Success ................................................................... 26 Chapter 8: Disruption of Female Skateboarding Leading -

Agenda Packet
TOWN OF FLORENCE SPECIAL MEETING AGENDA Mayor Tara Walter Florence Town Hall Vice-Mayor John Anderson 775 N. Main Street Councilmember Bill Hawkins Florence, AZ 85132 Councilmember Kristen Larsen (520) 868-7500 Councilmember Karen Wall www.florenceaz.gov Councilmember Michelle Cordes Meet 1st and 3rd Mondays Councilmember Judy Hughes Monday, June 17, 2019 4:30 PM ____________________________________________________________________________ Pursuant to A.R.S. § 38-431.02, notice is hereby given to the Town of Florence Council and to the general public that a Special Meeting of the Florence Town Council will be held on Monday, June 17, 2019, at 4:30 p.m., in the Florence Town Council Chambers, located at 775 N. Main Street, Florence, Arizona. The agenda for this meeting is as follows: 1. CALL TO ORDER 2. ROLL CALL: Tara Walter __, John Anderson__, Bill Hawkins__, Karen Wall____, Kristen Larsen___, Michelle Cordes__, Judy Hughes ___. 3. ADJOURNMENT TO EXECUTIVE SESSION For the purposes of discussions or consultations with designated representatives of the public body and/or legal counsel pursuant to A.R.S. Sections 38-431.03 (A)(3), (A)(4) and (A)(7) to consider its position and instruct its representatives and/or attorneys regarding: a. Town’s position and instruct its attorneys regarding pending litigation in Maricopa County Superior Court: Town of Florence v. Florence Copper, Inc. CV2015-000325, including counterclaims. b. Town’s position and instruct its attorneys regarding Arizona Department of Environmental Quality proceedings, related to Water Quality Appeals Board Case No. 16-002, including appellate proceedings to reviewing courts. c. Town’s position and instruct its attorneys regarding permitting, constructing and accepting of irrigation wells and National Environmental Policy Act 26 (“NEPA”) and the Administrative Procedure Act (“APA”). -

Big Wig Hurley Emea Covid-19 Biz Strategies June 2020 €5 #101
BIG WIG HURLEY EMEA COVID-19 BIZ STRATEGIES JUNE 2020 €5 #101 RETAIL BUYER’S GUIDES SURFBOARDS, SUNGLASSES, SUP, LONGBOARDS, IMPACT VESTS, KITES DURA-CORD WITH SPEED POCKETS ZERO DISTRACTION ANKLE CUFF CLOSURE SILICONE ANKLE GRIPS INTRODUCING THE INFINITE FLEX KAIMANA 360° LEASH ENDS The ultimate fusion of strength, comfort, and ingenuity, delivering the freedom of a leash-less feel. THIN LINE RAILSAVER SYSTEM ALWAYS TRUSTED. EVER PROGRESSING. DAKINE.COM 2 3 4 5 Reduce your impact by making one. Every Dragon Upcycled frame is made from the waste of 5 plastic bottles. cycled #GetUp ©2020 Marchon Eyewear Inc. Style Shown: DR RENEW LL ION 6 7 which ultimately help you diversity to be a flash in EDITORIAL do your job better, will be the pan and while our plan CONTENT behind a paywall. and learnings continue to SOURCE#101 P.08 Contents evolve, we can promise P.36 Retail Buyer’s Guide: P.78 Market Insight: This issue contains our our readership that in the P.10 News SUP 2020 Austrian + Italian usual Retail Buyer’s future we will do better at Guides to help retailers showcasing our industry’s P.14 How COVID-19 Affected P.48 Retail Expertise: Blue P.80 Brand Profile: see what’s trending in people of colour, the Euro Boardsport Industry Tomato CEO Adam Ellis Landyachtz summer 2020 categories, COVID-19’s effect on the brands they work for and P.18 Market Insight: German boardsports industry has but we also speak with the art they do. We’ll also P.52 Retail Buyer’s Guide: P.75 Retail Buyer’s Guide: been seismic and combining retailers, distributors -

“Rules of the Road” for Personal Transportation Devices Kevin Fang Sonoma State University
San Jose State University SJSU ScholarWorks Mineta Transportation Institute Publications 5-2019 How and Where Should I Ride This Thing? “Rules Of The Road” for Personal Transportation Devices Kevin Fang Sonoma State University Asha Weinstein Agrawal San Jose State University, [email protected] Ashley M. Hooper University of California, Irvine Follow this and additional works at: https://scholarworks.sjsu.edu/mti_publications Part of the Transportation Commons Recommended Citation Kevin Fang, Asha Weinstein Agrawal, and Ashley M. Hooper. "How and Where Should I Ride This Thing? “Rules Of The Road” for Personal Transportation Devices" Mineta Transportation Institute Publications (2019). This Report is brought to you for free and open access by SJSU ScholarWorks. It has been accepted for inclusion in Mineta Transportation Institute Publications by an authorized administrator of SJSU ScholarWorks. For more information, please contact [email protected]. Project 1713 May 2019 How and Where Should I Ride This Thing? “Rules of the Road” For Personal Transportation Devices Kevin Fang, Ph.D. Asha Weinstein Agrawal, Ph.D. Ashley M. Hooper MINETA TRANSPORTATION INSTITUTE transweb.sjsu.edu MINETA TRANSPORTATION INSTITUTE MTI FOUNDER LEAD UNIVERSITY OF Hon. Norman Y. Mineta Mineta Consortium for Transportation Mobility MTI BOARD OF TRUSTEES Founded in 1991, the Mineta Transportation Institute (MTI), an organized research and training unit in partnership with the Founder, Honorable Norman Richard Anderson (Ex-Officio) Steve Heminger* (TE 2018) Dan Smith (TE 2020) Lucas College and Graduate School of Business at San José State University (SJSU), increases mobility for all by improving the safety, Mineta (Ex-Officio) President and CEO Executive Director President Secretary (ret.), US Department of Amtrak Metropolitan Transportation Capstone Financial Group, Inc.