Requires That ADA Paratransit Service Be Provided As an Alternative Mode
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

System Fact Sheet
SPRING 2017 Valley Metro System Fact Sheet VALLEY METRO RPTA BOARD OF DIRECTORS Councilmember Thelda Williams, Chair Valley Metro is the regional public transportation agency providing coordinated, City of Phoenix multi-modal transit options to residents of greater Phoenix. With a core mission of advancing a regional transportation network, Valley Metro plans, develops Vice Mayor Suzanne Klapp, Vice Chair and operates the bus, vanpool and light rail systems and alternative City of Scottsdale transportation programs for commuters, seniors and people with disabilities. Councilmember Lauren Tolmachoff, Treasurer City of Glendale HISTORY Councilmember Pat Dennis In 1993, the name Valley Metro was adopted as the identity for the regional City of Avondale transit system in the metropolitan Phoenix region. Under this brand name, local governments set the policy for the regional system that operates throughout the Councilmember Eric Orsborn City of Buckeye Valley. In 2008, the first 20 miles of light rail began service. Currently, six light rail extensions are planned or under construction to create a 66-mile system by Vice Mayor Kevin Hartke 2034. City of Chandler Councilmember Jack Palladino Valley Metro is governed by two boards of directors. The Regional Public City of El Mirage Transportation Authority (RPTA) Board consists of 16 public agencies (15 cities and Maricopa County) that set the policy direction for all modes of transit except Councilmember Brigette Peterson light rail. The Valley Metro Rail Board consists of five cities that set the policy Town of Gilbert direction for light rail high-capacity transit. The boards and the agency work to Councilmember Sharolyn Hohman improve and regionalize the public transit system. -

Mobility Center Getting Started
Valley Metro Mobility Center Getting Started The Mobility Center is a state-of-the-art some practice using transit in a safe 1. To apply for ADA Paratransit/Dial-a-Ride When Will You Be Notified Regarding Location: multifunctional facility that simulates and controlled setting. For Valley Metro, service, call 602.716.2100. Your Eligibility? Valley Metro the look and feel of the Valley’s public the transit environment provides an 2. Request an ADA Paratransit application. You will receive an ADA Paratransit Van Buren St transit system. The Center provides opportunity for us to accurately evaluate eligibility determination letter within ADA Paratransit/Dial-a-Ride eligibility whether our buses and trains can 3. Complete the application. Then call 21 calendar days of your assessment. Mobility Center assessments and a Travel Training accommodate the specific needs of each 602.716.2100 to schedule an appointment FOR THOSE WITH ALTERNATIVE program for people with disabilities. customer who applies for ADA Paratransit for an in-person assessment. How Should You Travel to the TRANSPORTATION NEEDS Mobility Center? and to determine whether travel training Drop-off area Visitor parking What Should You Expect on the Day of on ground level Customers can take a “transit walk” might be a viable option. The Mobility Center is located in central Your In-Person Assessment? 48th St Phoenix with convenient access to 44th St through a simulated streetscape in an You will meet with a transit evaluator who indoor environment, which includes The Center provides -

DATE AGENDA ITEM 4 January 25, 2017
DATE AGENDA ITEM 4 January 25, 2017 SUBJECT East Valley, Northwest Valley and Regional Paratransit Service Contract Award PURPOSE To request authorization for the Chief Executive Officer (CEO) to execute a contract with Transdev for the operation of East Valley, Northwest Valley and Regional Paratransit Services for a total of five years for an amount not to exceed $124.47 million, which includes a base contract cost of $108.34 million, a contract contingency of $10.83 million (10% of the five-year contract value) and a projected pass through reimbursement cost for fuel of $5.30 million. BACKGROUND/DISCUSSION/CONSIDERATION Valley Metro paratransit operations are currently performed under two contracts (Contract 1040014-S and Contract 1240003-S). Valley Metro is consolidating all services into one new turnkey paratransit operations contract resulting in one contractor who will accept customer calls, verify customer eligibility, schedule requested trips, operate the service, maintain the vehicles and provide all associated administrative support and reporting functions, including customer service. The new paratransit service contract is designed to improve our focus on service, safety, quality and productivity. It is designed to build on the utilization of dedicated vehicles and drivers for trips which can be grouped effectively, while still using flexible, non-dedicated vehicles (such as taxicabs) for trips which cannot be shared in a cost- effective manner. The new contract will also allow for the implementation of technology which will enable customers to use mobile phones and other electronic devices to interact with the paratransit service, thereby increasing service quality and responsiveness for customers while helping Valley Metro and its contractor to run the most efficient operation possible. -
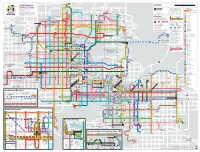
SYSTEM MAP Scale Is Approximate
Happy Valley Rd Happy Valley 0 1 2 3 4 5 R I- LEGEND Miles SYSTEM MAP Scale is approximate. MAPA DEL SISTEMA Pinnacle Peak Rd 17 Transit Center Valley Metro Rail Local Buses Light Rail, Local, Express Phoenix-Deer Valley Municipal Airport Frequent and reliable all-day rail Main bus route 29th Ave Park-and-Ride Regular service Deer Valley Dr E Marriott Dr and RAPID Bus Routes 19th Ave 27th Ave 27th Ave 23rd service operating 365 days a year Select trips only Barry Point of Interest linking Phoenix, Tempe and Mesa Limited service Deer Valley Rd Eective/Validez 10.28.2019 Goldwater Direction of Travel with connections to Sky Harbor High School R SR Central Avenue Honeywell Airport and many bus routes. Rose Garden Ln Rose Garden Ln Desert Ridge Marketplace St 73rd 602.253.5000 | valleymetro.org Pima Fwy Scottsdale Healthcare Dr Washington Agua Fria Fwy 7th Ave 101 Rail line is on 101 E Mayo Blvd Thompson Peak Pkwy this street Train stops only at Van Buren HonorHealth Scottsdale Beardsley Rd Beardsley Rd 51 RAPID Bus light rail stations Glendale Thompson Peak 7th Street Foothills Library Fast and frequent bus service from Apache Blvd Behrend Dr Yorkshire Dr park-and-rides to downtown Phoenix 7th Avenue Utopia Rd Blvd Tatum Abrazo Arrowhead Hospital E on weekdays 5–8 a.m. and 3–6 p.m. Union Hills Dr Rd Creek Cave Light rail line Roosevelt Union Hills Dr E 56th St Mayo Clinic See light rail map on reverse for details. Phoenix Campus E Foothills Paradise Valley 101 R I-E 12th Street Aquatics Center Ave 27th 17 Community College RAPID stops only at these RAPID route(s) Buckeye Road 59th Ave 59th Arrowhead Ave 57th points and at transit centers. -
Boards of Directors
MEETINGS OF THE Boards of Directors Joint Meeting Valley Metro RPTA and Valley Metro Valley Metro Valley Metro Rail RPTA Rail Date: September 17, 2020 Starting Time 11:15 a.m. Meetings to occur sequentially Location: Valley Metro Via Webex Phoenix Valley Metro is not accepting visitors at this time. Please join the Board meeting via Webex. If you require assistance accessing the meetings on the th th 10 floor, please go to the 14 floor or call 602.262.7433. Valley Metro I 101 N. 1st Ave. Phoenix, AZ 85003 602.262.7433 Agenda September 10, 2020 Joint Meeting Agenda Valley Metro RPTA And Valley Metro Rail Thursday, September 17, 2020 Webex/Phone 11:15 a.m. Action Recommended 1. Public Comment (yellow card) 1. For Information Public comment is being taken in written format and will be entered into the official minutes of the meeting. 2. Chief Executive Officer’s Report 2. For information Scott Smith, CEO, will brief the Boards of Directors on current issues. 3. COVID-19 Update 3. For information An update on transit operation impacts related to COVID-19 will be provided. 4. Minutes 4. For action Minutes from the August 27, 2020 Joint Board meeting are presented for approval. 5. Audit and Finance Subcommittee Update 5. For information Councilmember Arredondo-Savage, AFS Chair, will provide an update on the discussions and actions taken at the AFS meeting. Valley Metro I 101 N. 1st Ave. Phoenix, AZ 85003 602.262.7433 5A. Audit and Finance Subcommittee Charter 5A. For action Councilmember Arredondo-Savage, AFS Chair, will request that the Boards of Directors approve the AFS Subcommittee Charter. -

System Fact Sheet City of Avondale
SPRING 2016 VALLEY METRO VALLEY METRO RPTA BOARD OF DIRECTORS Councilmember Jim McDonald, Chair System Fact Sheet City of Avondale Valley Metro is the regional public transportation agency providing coordinated, Councilmember Thelda Williams, Vice Chair multi-modal transit options to residents of greater Phoenix. With a core mission of City of Phoenix advancing a total transit network, Valley Metro plans, develops and operates the Councilmember Suzanne Klapp, Treasurer regional bus and light rail systems and alternative transportation programs for City of Scottsdale commuters, seniors and people with disabilities. Councilmember Eric Orsborn City of Buckeye HISTORY In 1993, the name Valley Metro was adopted as the identity for the regional Vice Mayor Kevin Hartke transit system in the metropolitan Phoenix region. Under this brand name, local City of Chandler governments set the policy for the regional system that operates throughout the Councilmember Jack Palladino Valley. In 2008, the first 20 miles of light rail began service. Currently, six light rail City of El Mirage extensions are planned or under construction to create a 66-mile system by 2034. Councilmember Jenn Daniels Town of Gilbert Valley Metro is governed by two boards of directors. The Regional Public Transportation Authority (RPTA) Board consists of 16 public agencies (15 cities and Councilmember Lauren Tolmachoff Maricopa County) that set the policy direction for all modes of transit except light City of Glendale rail. The Valley Metro Rail Board consists of five cities that set the policy direction for light rail high-capacity transit. The boards and the agency work to improve and Councilmember Sharolyn Hohman City of Goodyear regionalize the public transit system. -

Contact Information Retail Locations Fares
AUGUST 2013 RETAIL LOCATIONS CONTACT INFORMATION BUS / LIGHT RAIL There are nearly 800 retail locations where you can Customer Service: 602.253.5000 purchase your pass before boarding. Purchase TTY: 602.251.2039 (for the hearing impaired) passes at most valley-wide locations of the following stores: Customers can obtain information about various transit services by using our automated phone • 7-Eleven system 24 hours a day, 365 days a year. Hablamos • Circle K español. • Corner Store (formerly Valero) RIDE • Food City (select locations only) Customer Service Business Hours • Fry's Food Store • Weekdays, 6 am - 8 pm • PLS Check Cashers • Saturdays, 7 am - 7 pm • Safeway GUIDE • Sundays and designated holidays, 8 am - 5 pm • Walgreens • Closed New Year’s Day, Memorial Day, Passes can also be purchased at participating: Independence Day, Labor Day, Thanksgiving Day and Christmas Day • APS locations • Public libraries Lost and Found Information: 602.253.5000. • Transit centers Use the automated system for help. When prompted, say “Lost and Found” and provide the route number. Not all pass types are sold at every location. Follow provided instructions. Please contact the location prior to traveling to check availability of passes and types of payment Transit Watch. Help improve transit safety and accepted. security by reporting any and all suspicious activities to Valley Metro Customer Service. In case of For a complete list of retail locations, visit emergencies, call 911. valleymetro.org or call 602.253.5000. Local bus/light rail/ LINK Reduced** Express/ RAPID FARES 1-Ride* $2.00 $1.00 $3.25 Local bus, light rail and LINK share the same fare structure and pass All-Day $4.00 $2.00 $6.50 types. -

System Fact Sheet
SYSTEM FACT SHEET FISCAL YEAR 2014 Valley Metro is the regional public transportation agency providing coordinated, multi-modal transit options to residents of greater Phoenix. With a core mission of advancing a total transit VALLEY METRO RPTA BOARD OF DIRECTORS network, Valley Metro plans, develops and operates the regional bus and light rail systems Councilmember Jim McDonald, Chair and alternative transportation programs for commuters, seniors and people with disabilities. City of Avondale Councilmember Gary Sherwood, Vice Chair HISTORY City of Glendale In 1993, the name Valley Metro was adopted as the identity for the regional transit system Councilmember Thelda Williams, Treasurer in the metropolitan Phoenix region. Under this brand name, local governments set the City of Phoenix policy for the regional system that operates throughout the Valley. In 2008, the first Vice Mayor Eric Orsborn 20 miles of light rail began service. Currently, seven light rail extensions are planned or are City of Buckeye under construction that will create a 60-mile system by 2034. Vice Mayor Kevin Hartke City of Chandler Valley Metro is governed by two Boards of Directors. The Regional Public Transportation Authority (RPTA) Board consists of 16 public agencies (15 cities and Maricopa County) Councilmember Lynn Selby that set the policy direction for all modes of transit except light rail. The Valley Metro Rail City of El Mirage Board consists of five cities that set the policy direction for light rail high-capacity transit. Councilmember Jenn Daniels The Boards and the agency work to improve and regionalize the public transit system. Town of Gilbert Vice Mayor Joe Pizzillo City of Goodyear REGIONAL FUNDING Supervisor Steve Gallardo Maricopa County voters approved Proposition 400 in 2004 extending the 1983 Maricopa County county-wide transportation tax. -
Destination Guide Showcasing Locations Around the Valley Accessible by Local Bus and Light Rail
Destination Guide Showcasing locations around the Valley accessible by local bus and light rail. Fall 2010 Valley Metro is your ride to Fall fun! Where to Purchase Fares Ride the local bus and light rail and... Save money by purchasing an All-day pass off the bus! • Get out of traffic jams • Avoid parking costs Retail Outlets: Select Fry’s, PLS Check Cashers, Safeway and • Save money on gas 7-Eleven stores sell passes. Check the location nearest you for the types of passes sold. **Fare Vending Machines (FVM): Located at each light rail FARES station, you can purchase one ride or one way for METRO light rail. All-day pass or greater fares purchased from the vending Pass Type machines are valid for both bus and light rail. Credit/debit LOCAL BUS/LINK/LIGHT RAIL - FULL FARE cards and cash are accepted. 1-ride (cash fare only) $1.75 Purchase Onboard (Bus only): If you purchase an All-day pass on the bus, have exact fare ready. Operators cannot issue All-day pass $3.50 change. Passes purchased onboard are automatically activated All-day pass (on-board bus) $5.25 and valid until 3-day (FVM only)** $10.50 2:59 a.m. the next day. Credit/debit 7-day $17.50 cards are not accepted. 31-day $55.00 Online Ordering: Visit ValleyMetro.org to purchase All-day, 7- or 31-day transit passes using a debit or credit card. LOCAL BUS/LINK/LIGHT RAIL - REDUCED FARE* 1-ride (cash fare only) $0.85 All-day pass $1.75 Hours of Operation All-day pass (on-board bus) $2.60 3-day (FVM only)** $5.25 BUS Bus service operates 365 days a year on all local routes in 7-day $8.75 Glendale, Phoenix, Scottsdale and Tempe. -

Ride Guide for Bus & Light Rail
FareFare FareFare VendingVending ProofProof ofof ContactContact HowHow toto RideRide ConnectionsConnections InformationInformation MachinesMachines PaymentPayment InformationInformation 3. Press send Press 3. STOP# 2. Enter 5-digit 5-digit Enter 2. •• PlanPlan youryour triptrip usingusing thethe onlineonline triptrip plannerplanner atat LocalLocal busbus andand lightlight railrail shareshare thethe samesame farefare FareFare vendingvending machinesmachines areare locatedlocated atat eacheach lightlight railrail LightLight railrail operatesoperates onon aa proof-of-paymentproof-of-payment system.system. CustomerCustomer Service:Service: 602.253.5000602.253.5000 or service animal. service or BUSBUS && LIGHTLIGHT RAILRAIL ®® 22966 1. Text Text 1. Valley Metro valleymetro.orgvalleymetro.org,,, RidekickRidekickRidekick ,,, thethethe TransitTransitTransit structurestructure andand passpass types.types. PassesPasses cancan bebe purchasedpurchased station.station. AnAn All-DayAll-Day oror multi-daymulti-day passpass isis alsoalso validvalid FareFare inspectorsinspectors regularlyregularly patrolpatrol thethe systemsystem andand askask TTY:TTY: 602.251.2039602.251.2039 (for(for thethe hearinghearing impaired)impaired) facilities or threatens the safety of any other person person other any of safety the threatens or facilities PlanPlan youryour triptrip usingusing thethe manymany busbus connectionsconnections thatthat BookBook oror contactcontact CustomerCustomer Service.Service. fromfromfrom farefarefare vendingvendingvending machines,machines,machines, -

Transportation Expenses Add up in Phoenix Area Living on the Outskirts of Town May End up Costing More Our New Look… Than Expected
The mission of the RPTA is to promote the social and economic well-being of the community through an efficient and effective regional transit system as a valued and www.valleymetro.maricopa.gov significant component of the transportation network. Destinations is the official newsletter of the Regional Public Transportation Authority. Vol. IV, Issue II Spring 2001 Transportation Expenses Add Up in Phoenix Area Living on the outskirts of town may end up costing more Our New Look… than expected. According to a new report, Driven to Spend, Destinations’ style and recently released by the Surface Transportation Policy appearance have been Project (STPP), the Phoenix metropolitan region is ranked revised in an effort to better seventh in the nation when it comes to transportation provide readers with quick, easy-to-read updates spending. In fact, we spend more on getting around town regarding public (18.2 percent) than any other household expense, except transportation in shelter (19.9 percent). The average family in the Phoenix Maricopa County. area spends nearly $7,000 a year on transportation. We welcome your comments on these While the spending seems lopsided towards personal vehicle ownership, this changes by calling Susan breakdown is not unusual across the U.S. Remarkably, in some metro areas, Tierney at (602) 262-4668 households are spending more on transportation than shelter. The vast majority or via e-mail at of that spending—98 percent—is for the purchase, operation, and maintenance [email protected] . of automobiles. The spread-out development pattern, commonly called sprawl, makes the biggest impact according to how much is spent on transportation, according to Gloria Ohland, campaign manager for STPP. -

Valley Metro System Map April 2017
35 Happy Valley Rd Happy Valley 0 1 2 3 4 5 I-17 LEGEND Miles SYSTEM MAP Scale is approximate. Pinnacle Peak Rd 17 MAPA DEL SISTEMA 19 Transit Center Valley Metro Rail Local Buses Light Rail, Local, Express Phoenix-Deer Valley Municipal Airport Frequent and reliable all-day rail 29th Ave Main bus route Deer Valley Dr Park-and-Ride E Marriott Dr 136 and RAPID Bus Routes 19th Ave 27th Ave 27th Ave 23rd service operating 365 days a year 44 Select trips only Barry 7 Point of Interest linking Phoenix, Tempe and Mesa 27 Deer Valley Rd Eective/Validez 04.24.2017 Goldwater Direction of Travel with connections to Sky Harbor High School SR 51 0 Central Avenue Honeywell Airport and many bus routes. Rose Garden Ln 27 Rose Garden Ln 90 Desert Ridge Marketplace 72 St 73rd 602.253.5000 | valleymetro.org Pima Fwy Scottsdale Healthcare Dr 1 Washington Agua Fria Fwy 7th Ave 101 Rail line is on 101 575 Mayo Blvd Thompson Peak Pkwy this street Train stops only at 3 Van Buren HonorHealth Scottsdale Beardsley Rd Beardsley Rd 51 RAPID Bus light rail stations 575 Thompson Peak 7 7th Street Utopia Rd Fast and frequent bus service from Apache Blvd Behrend Dr Yorkshire Dr Glendale Foothills Library park-and-rides to downtown Phoenix 8 7th Avenue Utopia Rd Blvd Tatum 575 on weekdays 5–8 a.m. and 3–6 p.m. Union Hills Dr Rd Creek Cave Light rail line 10 Roosevelt Union Hills Dr 43 186 16 39 186 56th St Mayo Clinic See light rail map on reverse for details.