RRH: Rural and Remote Health Article: 5666
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

EUROPEAN COMMISSION Brussels, 8.10.2019 COM(2019)
EUROPEAN COMMISSION Brussels, 8.10.2019 COM(2019) 463 final REPORT FROM THE COMMISSION TO THE COUNCIL 2019 report on the economic and social situation of Gozo (Malta) EN EN 2019 REPORT ON THE ECONOMIC AND SOCIAL SITUATION OF GOZO (MALTA) Without prejudice to the ongoing negotiations on the Multiannual Financial Framework for the period 2021-2027, and in accordance with Declaration 36 on the island region of Gozo annexed to the Treaty of Accession of Malta, the Government of Malta requested in February 2019 the Commission to report to the Council on the economic and social situation of Gozo and, in particular, on the disparities of the social and economic development levels between Gozo and Malta and to propose appropriate measures, to enable the further integration of Gozo within the internal market. This report assesses the state of development of Gozo and the evolution of disparities within Malta. It provides an assessment by reviewing recent trends on a series of dimensions and indicators relevant for the development of Gozo, i.e. demography and labour market, structure of the economy and economic growth, geography and accessibility. The paper also provides a comparison of Gozo with the rest of Malta and with other European regions. Finally, it analyses how Cohesion policy addresses the development needs of Gozo. This report uses regional statistics produced by Eurostat and by the Maltese Statistical Office. 1. ANALYSIS OF THE ECONOMIC AND SOCIAL SITUATION IN GOZO 1.1. Geography and land use Gozo is the second most important island of the Maltese archipelago in terms of surface and population. -

Socioeconomic Status and Its Impact on the Prevalence of Severe ADHD in the Maltese Islands
OriginalEditorial OrgOdRe Article Socioeconomic status and its impact on the prevalence of severe ADHD in the Maltese Islands Christopher Rolé, Nigel Camilleri, Rachel Taylor-East, Neville Calleja Abstract The main aim of this study was to assess Attention deficit hyperactivity disorder whether higher prevalence rates of ADHD were (ADHD) is a common disorder which presents in present in the districts, which are classically childhood. The core symptoms include; associated with a low socioeconomic status. All hyperactivity, impulsivity and reduced attention. If persons aged 0 to 18 years attending the left untreated this may possibly lead to various governmental clinics, having a documented impairments of function in other areas of one’s life, diagnosis of severe ADHD and therefore being such as lack of educational attainment, increased prescribed pharmacotherapy were identified and risk of accident-prone behaviour, substance misuse included in this study. Nine young people were and antisocial behaviours. Although the exact living in institutional care and were therefore aetiology is still not fully understood, various excluded from statistical analysis since this would studies have demonstrated the presence of both a skew that data in this study. A significant difference genetic and an environmental component. ADHD is (p<0.0001) in the point prevalence of ADHD highly hereditable, demonstrating a strong genetic between the six Malta districts was found, with component (0.75). Furthermore, increased rates of higher rates of ADHD occurring in the harbour ADHD have been linked with a low socioeconomic districts. Though not statistically significant, a status. positive correlation was demonstrated between the The islands of Malta have traditionally been ADHD prevalence and a number of socioeconomic divided for statistical purposes into 6 districts, with variables, these included; the rate of smoking certain districts more often being associated with (p=0.111), number of people classified as at-risk-of- low socioeconomic demographics. -

State of Populism in Europe
2018 State of Populism in Europe The past few years have seen a surge in the public support of populist, Eurosceptical and radical parties throughout almost the entire European Union. In several countries, their popularity matches or even exceeds the level of public support of the centre-left. Even though the centre-left parties, think tanks and researchers are aware of this challenge, there is still more OF POPULISM IN EUROPE – 2018 STATE that could be done in this fi eld. There is occasional research on individual populist parties in some countries, but there is no regular overview – updated every year – how the popularity of populist parties changes in the EU Member States, where new parties appear and old ones disappear. That is the reason why FEPS and Policy Solutions have launched this series of yearbooks, entitled “State of Populism in Europe”. *** FEPS is the fi rst progressive political foundation established at the European level. Created in 2007 and co-fi nanced by the European Parliament, it aims at establishing an intellectual crossroad between social democracy and the European project. Policy Solutions is a progressive political research institute based in Budapest. Among the pre-eminent areas of its research are the investigation of how the quality of democracy evolves, the analysis of factors driving populism, and election research. Contributors : Tamás BOROS, Maria FREITAS, Gergely LAKI, Ernst STETTER STATE OF POPULISM Tamás BOROS IN EUROPE Maria FREITAS • This book is edited by FEPS with the fi nancial support of the European -
Sulfur Dioxide Trends in Malta: a Statistical Computing Approach Nicholas Desira James Madison University
James Madison University JMU Scholarly Commons Masters Theses The Graduate School Fall 2012 Sulfur dioxide trends in Malta: A statistical computing approach Nicholas Desira James Madison University Follow this and additional works at: https://commons.lib.jmu.edu/master201019 Part of the Environmental Sciences Commons Recommended Citation Desira, Nicholas, "Sulfur dioxide trends in Malta: A statistical computing approach" (2012). Masters Theses. 182. https://commons.lib.jmu.edu/master201019/182 This Thesis is brought to you for free and open access by the The Graduate School at JMU Scholarly Commons. It has been accepted for inclusion in Masters Theses by an authorized administrator of JMU Scholarly Commons. For more information, please contact [email protected]. SULFUR DIOXIDE TRENDS IN MALTA: A STATISTICAL COMPUTING APPROACH NICHOLAS DESIRA M.Sc. in Sustainable Environmental Resources Management & Integrated Science and Technology October 2012 Approved and recommended for acceptance as a dissertation in partial fulfillment of the requirements for the degree of Master of Science in Sustainable Environmental Resources Management & Integrated Science and Technology. Special committee directing the dissertation work of Nicholas Desira __________________________________________ Mr. Mark Scerri Date __________________________________________ Mr. Joel Azzopardi Date __________________________________________ Dr. Bob Kolvoord Date __________________________________________ Academic Unit Head or Designee Date Received by the Graduate School ____________________ Date SULFUR DIOXIDE TRENDS IN MALTA: A STATISTICAL COMPUTING APPROACH NICHOLAS DESIRA A dissertation submitted to the Graduate Faculty of JAMES MADISON UNIVERSITY - UNIVERSITY OF MALTA In Partial Fulfilment of the Requirements for the degree of Master of Science in Sustainable Environmental Resources Management & Integrated Science and Technology October 2012 ACKNOWLEDGEMENTS I would like to acknowledge the contribution of other people who supported me during the time I was working on this study. -

REGISTRATION SCHOOL CHOICE LIST KINDER 2 BOYS Segretarjat
Segretarjat għall-Edukazzjoni Nisranija Kurja tal-Arċisqof, Floriana REGISTRATION SCHOOL CHOICE LIST KINDER 2 BOYS Rank App. N. Student Name School Chosen 1 7312 LUCA GJONI ST. ANGELA MSIDA KINDER 2 7135 LUCA BENNETTI ST. ANGELA MSIDA KINDER 3 4295 CONOR O'BRIEN EDWARDS ST. ANGELA MSIDA KINDER 4 7341 MASON JAMES CARUANA ST. ANGELA RABAT KINDER 5 7576 BLAKE FARRUGIA ST. ANGELA RABAT KINDER 6 7218 JACK PARNIS ST. FRANCIS BIRKIRKARA 7 7383 GIANLUCA ORSINI ST. ANGELA MSIDA KINDER 8 7311 JACK GALEA ST. ANGELA MSIDA KINDER 9 7119 BEN ZAMMIT ST. ANGELA RABAT KINDER 10 4289 EZEQUIEL SPITERI ST. ANGELA MSIDA KINDER 11 7159 VIYAN GANDLA ST. FRANCIS BIRKIRKARA 12 7474 TOM RUSSELL WOLF VERDOODT ST. ANGELA RABAT KINDER 13 7616 ZAK AZZOPARDI ST. ANGELA RABAT KINDER 14 7689 LIAM CASSAR ST. ANGELA ZABBAR KINDER 15 7582 MIGUEL AXISA ST ALBERT THE GREAT COLLEGE KINDER FGURA 16 7601 JACK ELLUL ST ALBERT THE GREAT COLLEGE KINDER FGURA 17 4241 BENJAMIN BONELLO ST. ANGELA MSIDA KINDER 18 7308 ARTHUR TANTI ST. ANGELA RABAT KINDER 18 7309 ALEXANDER TANTI ST. ANGELA RABAT KINDER 19 7495 BEPPE CARUANA DEMICOLI ST. FRANCIS SAN GWANN KINDER 20 7294 JACK MALLIA UNGARO ST ALBERT THE GREAT COLLEGE KINDER FGURA 21 7594 GIUSEPPE CALOGERO VELLA ST. ANGELA ZABBAR KINDER Page 1 of 3 Segretarjat għall-Edukazzjoni Nisranija Kurja tal-Arċisqof, Floriana REGISTRATION SCHOOL CHOICE LIST KINDER 2 BOYS Rank App. N. Student Name School Chosen 22 7449 MIGUEL MAMO THERESA NUZZO HAMRUN KINDER 23 7739 MATT FALZON ST. ANGELA ZABBAR KINDER 24 7344 MICHELE BONAVIA MONTFORT ST. -
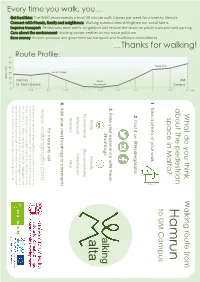
Ham Run Alta
km 2.5 What do you think Walking route from UM about the pedestrian Campus 2.25 space in Malta? Hamrun to UM Campus Skate Park Skate 2 1. Take a photo of your walk 1.75 2. Post it on @WalkingMalta 1.5 …Thanks …Thanks for walking! 3. Rate your experience with these #hashtags: alking 1.25 Msida Promenade #Safe #Unsafe alta . Walking communities strengthen our social fabric communities strengthen Walking . #Comfortable #Uncomfortable 1 #Pleasant #Unpleasant causes noise air causes pollution neither nor #Vibrant #Dull 0.75 4. Add your own hashtags or comments Walking Walking . Junior College Junior 0.5 For more info visit . Pedestrians ease traffic congestion and reduce the strain on public transport and on public parking transport the strain and reduce congestion ease traffic Pedestrians . www.walkingmalta.com The WHO recommends a brisk 30 minute walk 5 times per week for a healthy lifestyle a healthy for a brisk 305 week walk times minute per WHO The recommends By posting this info with @WalkingMalta you consent the use of it in . Reduce personal and governmental transport and healthcare expenditures and healthcare transport and governmental personal Reduce . 0.25 connection to our research project. Information included in your post with friends, family and neighbours and family friends, with will be analysed to give us valuable insights on pedestrian mobility and behaviour in Malta. Resulting data will be aggregated and anonymised. Personal data linked to your posts or messages, such as St. St. Paul’s Square Hamrun. Route Profile: username or profile picture, will be never used when disseminating . -

Sliema, St Julian's & Paceville
Sliema, St Julian’s & Paceville Why Go? Sights ..............................61 Malta’s cool crowd flocks to this area to promenade, eat, Activities .........................63 drink, shop and party. This is also where many tourists base Eating .............................63 themselves: despite the lack of interesting things to see or Drinking ..........................65 any beach to speak of, these three districts form a buzzing base and are well connected by public transport. Entertainment ................ 67 St Julian’s was once a pretty fishing village, but its origi- Shopping ........................ 67 nal charms have been all but obscured by the five-star hotels and apartment complexes rising along the rocky shoreline. It adjoins the small youth-oriented nightlife en- clave of Paceville, which only comes to life after dark; you Best Places to Eat won’t spot many punters aged over 25 here. This is also where many of Malta’s English-language schools are located. » Assaggi (p 64 ) Sliema has a more exclusive feel than St Julian’s, and has » Mint (p 63 ) long been associated with the Maltese upper classes. The » Zest (p 64 ) elegant backstreets remain largely residential and the busy » Kitchen (p 64 ) waterfront, while built-up, is dotted by some sophisticated eateries. Best Places to When to Go Stay Come in May, June, September and October if you’re look- » Hotel Juliani (p 133 ) ing for lower prices, guaranteed sunshine and few crowds. » Hotel Valentina (p 133 ) However, if you’re after a party atmosphere and lots of action, then head here during the peak summer months of » Palace Hotel (p 132 ) July and August, when the weather will be at its sultriest » Waterfront Hotel (p 132 ) and the nightlife at its most frenetic. -

COASTAL AREA MANAGEMENT in MALTA Note
COASTAL AREA MANAGEMENT IN MALTA Note This document was prepared by the Priority Actions Programme Regional Activity Centre (PAP/RAC) of the Mediterranean Action Plan (MAP-UNEP). The authors of the document are Louis Vella, Christine M. Tanti and Avertano Rolé. Zeljka Skaricic contributed to its general revision and finalisation, and Viktor Popovic designed and prepared the document for printing. The designations employed and the presentation of the material in this document do not imply the expression of any opinion whatsoever on the part of the United Nations Environment Programme or the Mediterranean Action Plan concerning the legal status of any state, territory, city or area, or their authorities, or concerning the delimitation of its frontiers or boundaries. The views expressed in this document do not necessarily represent the views of the United Nations Environment Programme. © 2005 Priority Actions Programme Regional Activity Centre, Split ISBN 953-6429-56-X This publication may be reproduced in whole or in part in any form of educational and non-profit purposes without special permission from the copyright holder, provided acknowledgement of the source is made. PAP would appreciate receiving a copy of any publication that uses this material as source. No use of this publication may be made for resale or any other commercial purposes whatsoever without prior permission in writing from the copyright holder. For bibliographic purposes this document may be cited as: PAP/RAC: Coastal Area Management in the Maltese Islands, Priority Actions Programme Regional Activity Centre, Split, 2005. TABLE OF CONTENTS List of Plates iv List of Figures iv List of Tables v List of Boxes v List of Acronyms vi ACKNOWLEDGEMENTS vii PREFACE ix EXECUTIVE SUMMARY xi CHAPTER I / Introduction 1 1. -

Local Government White Paper and Interrelated Regions and Districts
LOCAL GOVERNMENT WHITE PAPER AND INTERRELATED REGIONS AND DISTRICTS Perit Joseph Magro B.Sc.(Eng.)(Hons.), B.A.(Arch.) Update Note to the Addendum “Interrelated Regions and Districts for Malta and Gozo” Annexed to the Study Paper “Proposals For An Improved Malta Electoral System” This note proposes another solution of interrelated regions and districts, now based on the six regions as detailed in the Local Government White Paper. It also serves as a comparative study to the one put forward in the Addendum where a similar organizational structure of interrelated regions and districts for Malta and Gozo was proposed, with the districts also serving as electoral divisions. October 2018 LOCAL GOVERNMENT WHITE PAPER AND INTERRELATED REGIONS AND DISTRICTS Table of Contents 1. INTRODUCTION ……………………………………………………………………………………………………………………… 3 1.1 Reference to the Local Government White Paper 1.2 Reference to the Addendum 1.3 Main Objectives of This Update Note to the Addendum 1.4 Parameters Governing this Exercise 2. THE REGIONS AS ESTABLISHED IN THE WHITE PAPER ……………………………..…..………………………… 4 2.1 Maps of the Regions 3. ESTABLISHING THE DISTRICTS ……………………………………………………………………………………………….. 5 3.1 Hamlets 3.2 Numbering of Regions and Districts 4. COMPARATIVE CASE STUDIES …………………………………………….……………..………………………………….. 6 4.1 Proposed Organizational Structure and Registered Voter Changes 4.2 District Seat Value 4.3 Registered Voter Changes between October 2007 and April 2018 5. CONCLUSION ………………………………………………………………………………………………………………………… 8 Appendix 1: Map of the (White Paper) Regions and Proposed Districts …..…..….………………….……… 9 Appendix 2: Map of the Existing Regions of Malta ……………………………………………………………….…… 10 Appendix 3: Map of the Regions as Proposed in the White Paper ………………………………………….…. 11 2 1. INTRODUCTION 1.1 Reference to the Local Government White Paper The Local Government White Paper, published on 19th October 2018, refers to the existing five Regions of Malta as established by Act No. -

Following Paul from Shipwreck on Malta to Martyrdom in Rome MALTA • SICILY • ITALY Led by Dr
Following Paul from Shipwreck on Malta to Martyrdom in Rome MALTA • SICILY • ITALY Led by Dr. Carl Rasmussen MAY 11-22, 2021 organized by Following Paul from Shipwreck on Malta to Martyrdom in Rome / May 11-22, 2021 Malta Following Paul from Shipwreck on Malta to Martyrdom in Rome MAY 11-22, 2021 Fri 14 May Ferry to POZZALLO (SICILY) - SYRACUSE – Ferry to REGGIO CALABRIA Early check out, pick up our box breakfasts, meet the English-speaking assistant at our hotel and transfer to the port of Malta. 06:30am Take a ferry VR-100 from Malta to Pozzallo (Sicily) 08:15am Drive to Syracuse (where Paul stayed for three days, Acts 28.12). Meet our guide and visit the archeological park of Syracuse. Drive to Messina (approx. 165km) and take the ferry to Reggio Calabria on the Italian mainland (= Rhegium; Acts 28:13, where Paul stopped). Meet our guide and visit the Museum of Magna Grecia. Check-in to our hotel in Reggio Calabria. Dr. Carl and Mary Rasmussen Dinner at our hotel and overnight. Greetings! Mary and I are excited to invite you to join our handcrafted adult “study” trip entitled Following Paul from Shipwreck on Malta to Sat 15 May PAESTUM - to POMPEII Martyrdom in Rome. We begin our tour on Malta where we will explore the Breakfast and checkout. Drive to Paestum (435km). Visit the archeological bays where the shipwreck of Paul may have occurred as well as the Island of area and the museum of Paestum. Paestum was a major ancient Greek city Malta. Mark Gatt, who discovered an anchor that may have been jettisoned on the coast of the Tyrrhenian Sea in Magna Graecia (southern Italy). -

Malta 2017 Crime & Safety Report
Malta 2017 Crime & Safety Report Overall Crime and Safety Situation U.S. Embassy Valletta does not assume responsibility for the professional ability or integrity of the persons or firms appearing in this report. The ACS Unit cannot recommend a particular individual or location and assumes no responsibility for the quality of service provided. THE U.S. DEPARTMENT OF STATE HAS ASSESSED VALLETTA AS BEING A MEDIUM- THREAT LOCATION FOR CRIME DIRECTED AT OR AFFECTING OFFICIAL U.S. GOVERNMENT INTERESTS. Please review OSAC’s Malta-specific webpage for proprietary analytic reports, Consular Messages, and contact information. Crime Threats Malta is a generally safe country that receives numerous foreign tourists on a yearly basis. However, crimes of opportunity and violent crime do occur. Most street crimes are non-violent and non-confrontational and range from scams to petty theft. Theft of cell phones, computers, money, jewelry, and iPods is common. Visitors should keep these items out of sight and only use them in safe locations. Most street criminals are unarmed and are not prone to gratuitous violence. Victims of street crime are often inattentive targets of opportunity. Women should keep purses zipped and in front of them. Wear the shoulder straps of bags across your chest. Keep your money, credit cards, wallet, and other valuables in your front pockets. In 2016, crime statistics revealed that theft was the predominate criminal offense, making up over half of the crimes committed in Malta. Assaults numbered under 1,000, with the peak being June, July, and August (height of tourism season). Nationwide crime rates are higher in areas frequented by tourists to include: St. -

Migration, Surnames and Marriage in the Maltese Island of Gozo Around 1900
Journal of Maltese History, 2011/2 Migration, surnames and marriage in the Maltese island of Gozo around 1900. H.V.Wyatt Visiting Lecturer in the School of Philosophy, University of Leeds. Abstract The marriage records in the Public Registry in Gozo have been used to count the. frequency of surnames. Children with poliomyelitis and their controls from the same villages have been traced to their great grand-parents. These records have been used to trace migration to and from the larger island of Malta and the extent of consanguinity in each village. ______________________________________________________ Dr. Wyatt has held research and teaching posts in England, the United States, and the West Bank. He has taught and researched for 2 years in India, Pakistan and Bangladesh and for 4 years in Malta. He was previously Honorary Research Fellow in Public Health Medicine at Leeds University. Acknowledgements: I am very grateful to the Peel Medical Research Trust and the Royal Society for travel grants, to all the doctors, parish priests and other clergy who helped me, but especially to Professors H.M.Gilles and A. Scicluna-Spiteri. 35 Journal of Maltese History, 2011/2 Introduction To the north-west of Malta is the smaller island of Gozo (Fig 1), with an area of 67 square kilometres and about one tenth the population of Malta. In November 1942 poliovirus was introduced to the islands from Egypt and more than 420 children were paralysed. There were later, but smaller epidemics, until mass immunisation with the Sabin vaccine ensured that there have been no cases since 1964.