Long-Acting Injectable Antipsychotics. Review and Recent Developments
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Deanxit SPC.Pdf
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Deanxit film-coated tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains: Flupentixol 0.5 mg (as 0.584 mg flupentixol dihydrochloride) Melitracen 10 mg (as 11.25 mg melitracen hydrochloride) Excipients with known effect: Lactose monohydrate For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Film-coated tablets. Round, biconvex, cyclamen, film-coated tablets. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Anxiety Depression Asthenia. Neurasthenia. Psychogenic depression. Depressive neuroses. Masked depression. Psychosomatic affections accompanied by anxiety and apathy. Menopausal depressions. Dysphoria and depression in alcoholics and drug-addicts. 4.2 Posology and method of administration Posology Adults Usually 2 tablets daily: morning and noon. In severe cases the morning dose may be increased to 2 tablets. The maximum dose is 4 tablets daily. Older people (> 65 years) 1 tablet in the morning. In severe cases 1 tablet in the morning and 1 at noon. Maintenance dose: Usually 1 tablet in the morning. SPC Portrait-REG_00051968 20v038 Page 1 of 10 In cases of insomnia or severe restlessness additional treatment with a sedative in the acute phase is recommended. Paediatric population Children and adolescents (<18 years) Deanxit is not recommended for use in children and adolescents due to lack of data on safety and efficacy. Reduced renal function Deanxit can be given in the recommended doses. Reduced liver function Deanxit can be given in the recommended doses. Method of administration The tablets are swallowed with water. 4.3 Contraindications Hypersensitivity to flupentixol and melitracen or to any of the excipients listed in section 6.1. -

Thioxanthene Derivates As Sole Anti-Infective Agents
(19) & (11) EP 2 114 406 B1 (12) EUROPEAN PATENT SPECIFICATION (45) Date of publication and mention (51) Int Cl.: of the grant of the patent: A61K 31/496 (2006.01) A61P 31/04 (2006.01) 25.05.2011 Bulletin 2011/21 A61P 33/00 (2006.01) (21) Application number: 08700129.3 (86) International application number: PCT/DK2008/000005 (22) Date of filing: 07.01.2008 (87) International publication number: WO 2008/080408 (10.07.2008 Gazette 2008/28) (54) THIOXANTHENE DERIVATESAS SOLEANTI- INFECTIVEAGENTS FORUSE INT HE TREATMENT OF INFECTIOUS DISEASES THIOXANTHEN-DERIVATE ALS ALLEINVERTRETER DER ANTIINFEKTIVA ZUR VERWENDUNG IN DER BEHANDLUNG VON INFEKTIONSKRANKHEITEN DÉRIVÉS DE THIOXANTHÈNE COMME SEULS AGENTS ANTIINFECTIEUX POUR LEUR UTILISATION DANS LE TRAITEMENT DES MALADIES INFECTIEUSES (84) Designated Contracting States: • MORTENSEN I ET AL: "THE ANTIBACTERIAL AT BE BG CH CY CZ DE DK EE ES FI FR GB GR ACTIVITY OF THE HR HU IE IS IT LI LT LU LV MC MT NL NO PL PT PSYCHOPHARMACOLOGICAL AGENT RO SE SI SK TR CLOPENTHIXOL AND ITS TWO MAIN METABOLITES" ACTA PATHOLOGICA (30) Priority: 05.01.2007 PCT/DK2007/000006 MICROBIOLOGICASCANDINAVICA, SECTION B, XX, XX, vol. 95B, no. 6, 1987, pages 355-359, (43) Date of publication of application: XP008066133 ISSN: 0108-0180 11.11.2009 Bulletin 2009/46 • KOCISKO ET AL: "Comparison of protease- resistant prion protein inhibitors in cell cultures (60) Divisional application: infected with two strains of mouse and sheep 10181816.9 / 2 301 545 scrapie" NEUROSCIENCE LETTERS, LIMERICK, IE, vol. 388, no. 2, 11 November 2005 (2005-11-11), (73) Proprietor: BKG Pharma ApS pages 106-111, XP005042190 ISSN: 0304-3940 2920 Charlottenlund (DK) • KAISER C ET AL: "Analogs of phenothiazines. -

Ecstasy and the Concomitant Use of Pharmaceuticals
J.Copeland, P. Dillon & M. Gascoigne Ecstasy and the Concomitant Use of Pharmaceuticals NDARC Technical Report No. 201 ECSTASY AND THE CONCOMITANT USE OF PHARMACEUTICALS Jan Copeland (PhD), Paul Dillon & Michael Gascoigne Technical Report Number 201 ISBN: 1 877027 92 8 ©National Drug and Alcohol Research Centre, University of New South Wales, Sydney, 2004 This work is copyright. You may download, display, print and reproduce this material in unaltered form only (retaining this notice) for your personal, non-commercial use or use within your organisation. All other rights are reserved. Requests and enquiries concerning reproduction and rights should be addressed to the information manager, National Drug and Alcohol Research Centre, University of New South Wales, Sydney, NSW 2052, Australia. 2 ACKNOWLEDGEMENT This study and report was funded by the Australian Government Department of Health and Ageing’s National Illicit Drug Strategy. It was conducted concurrently with a study of aspects of information seeking among ecstasy users and there is some replication of the data presented on demographic characteristics and perception of ecstasy related harms in this Technical Report and Technical Report Number 202. 3 TABLE OF CONTENTS ACKNOWLEDGEMENT 3 TABLE OF CONTENTS 4 TABLE OF TABLES 5 EXECUTIVE SUMMARY 6 INTRODUCTION 7 Anti-depressant medication 8 5-hydroxytryptophan 9 Attention Deficit Hyperactivity Disorder 11 Sildenafil Citrate 12 Benzodiazepines 13 Study Ains 14 METHOD 15 Participants 15 Procedure 15 Measures 15 RESULTS 17 Demographics -

Clopixol Acuphase®)
Guidelines for the use of zuclopenthixol acetate injection (Clopixol Acuphase®) Version 3.1 – January 2018 GUIDELINE REPLACED Version 3 RATIFYING COMMITTEE Drugs and Therapeutics Group DATE RATIFIED October 2015 NEXT REVIEW DATE January 2021 EXECUTIVE SPONSOR Executive Medical Director ORIGINAL AUTHOR Jed Hewitt – Chief Pharmacist Review / update – 2015 Helen Manuell – Lead Pharmacist (ESx) Review / update - 2018 Jed Hewitt – Chief Pharmacist If you require this document in an alternative format, i.e. easy read, large text, audio or Braille please contact the pharmacy team on 01243 623349. Guidelines for the use of zuclopenthixol acetate injection (Clopixol Acuphase®) Introduction In the past, Acuphase® has often been too widely and possibly inappropriately used, sometimes without full regard being given to the fact that it is a potentially hazardous and toxic preparation with very little published information to support its use. Indeed, the Cochrane Library concludes that there is inadequate data on Acuphase® and no convincing evidence to support its use in acute psychiatric emergency. So far as possible, it should therefore be reserved for the minority of patients who have a prior history of previous use and good response, with use defined in an advance directive. Similarly, as a general rule Acuphase® should not be used for rapid tranquillisation unless such practice is also in accordance with an advance directive. Normally, Acuphase® should never be considered as a first-line drug for rapid tranquillisation as its onset of action will often not be rapid enough in these circumstances. In addition, the administration of an oil-based injection carries very high risk in a highly agitated patient. -

Aromaticity of Anthranil and Its Isomers, 1,2-Benzisoxazole and Benzoxazole Carmen Domene,A Leonardus W
Tetrahedron Letters Tetrahedron Letters 46 (2005) 4077–4080 Aromaticity of anthranil and its isomers, 1,2-benzisoxazole and benzoxazole Carmen Domene,a Leonardus W. Jenneskensb,* and Patrick W. Fowlerc aPhysical and Theoretical Chemistry Laboratory, Oxford University, South Parks Road, Oxford OX1 3QZ, UK bDebye Institute, Organic Chemistry and Catalysis, Utrecht University, Padualaan 8, 3584 CH Utrecht, The Netherlands cDepartment of Chemistry, University of Exeter, Stocker Road, Exeter EX4 4QD, UK Received 14 February 2005; revised 28 March 2005; accepted 5 April 2005 Available online 19 April 2005 Abstract—Direct computation of the p-current density, that is, the Ôring currentÕ, of anthranil (1) and its isomers 1,2-benzisoxazole (2) and benzoxazole (3) reveals different patterns of current flow: isomers 2 and 3 sustain strong benzene-like currents in the six- membered and bifurcated flow in the five-membered ring, whereas, in keeping with its lower thermodynamic stability, 1 has only a perimeter circulation without separate monocycle currents. Although the ring current criterion does not offer a sharp distinction between 2 and 3, their difference in thermodynamic stability is identical to that between isoxazole (4) and oxazole (5) suggesting an aromaticity order 1 < 2 3. Ó 2005 Elsevier Ltd. All rights reserved. The extent to which energetic, reactivity and magnetic property underlying NICS: the current density induced criteria of aromaticity are descriptions of a single, unify- by a perpendicular magnetic field, that is, the Ôring ing property of molecules remains a matter of debate.1 currentÕ, which gives an insight into the essential differ- Anthranil (1) and its isomers 1,2-benzisoxazole (2) and ence between anthranil (1) on the one hand and its benzoxazole (3) offer a series of bicyclic molecules with two isomers 2 and 3 on the other. -

CENTRAL NERVOUS SYSTEM DEPRESSANTS Opioid Pain Relievers Anxiolytics (Also Belong to Psychiatric Medication Category) • Codeine (In 222® Tablets, Tylenol® No
CENTRAL NERVOUS SYSTEM DEPRESSANTS Opioid Pain Relievers Anxiolytics (also belong to psychiatric medication category) • codeine (in 222® Tablets, Tylenol® No. 1/2/3/4, Fiorinal® C, Benzodiazepines Codeine Contin, etc.) • heroin • alprazolam (Xanax®) • hydrocodone (Hycodan®, etc.) • chlordiazepoxide (Librium®) • hydromorphone (Dilaudid®) • clonazepam (Rivotril®) • methadone • diazepam (Valium®) • morphine (MS Contin®, M-Eslon®, Kadian®, Statex®, etc.) • flurazepam (Dalmane®) • oxycodone (in Oxycocet®, Percocet®, Percodan®, OxyContin®, etc.) • lorazepam (Ativan®) • pentazocine (Talwin®) • nitrazepam (Mogadon®) • oxazepam ( Serax®) Alcohol • temazepam (Restoril®) Inhalants Barbiturates • gases (e.g. nitrous oxide, “laughing gas”, chloroform, halothane, • butalbital (in Fiorinal®) ether) • secobarbital (Seconal®) • volatile solvents (benzene, toluene, xylene, acetone, naptha and hexane) Buspirone (Buspar®) • nitrites (amyl nitrite, butyl nitrite and cyclohexyl nitrite – also known as “poppers”) Non-Benzodiazepine Hypnotics (also belong to psychiatric medication category) • chloral hydrate • zopiclone (Imovane®) Other • GHB (gamma-hydroxybutyrate) • Rohypnol (flunitrazepam) CENTRAL NERVOUS SYSTEM STIMULANTS Amphetamines Caffeine • dextroamphetamine (Dexadrine®) Methelynedioxyamphetamine (MDA) • methamphetamine (“Crystal meth”) (also has hallucinogenic actions) • methylphenidate (Biphentin®, Concerta®, Ritalin®) • mixed amphetamine salts (Adderall XR®) 3,4-Methelynedioxymethamphetamine (MDMA, Ecstasy) (also has hallucinogenic actions) Cocaine/Crack -

Quinolizidine-Derived Lucanthone and Amitriptyline Analogues Endowed with Potent Antileishmanial Activity
pharmaceuticals Article Quinolizidine-Derived Lucanthone and Amitriptyline Analogues Endowed with Potent Antileishmanial Activity Michele Tonelli 1,* , Anna Sparatore 2,* , Nicoletta Basilico 3,* , Loredana Cavicchini 3, Silvia Parapini 4 , Bruno Tasso 1 , Erik Laurini 5 , Sabrina Pricl 5,6 , Vito Boido 1 and Fabio Sparatore 1 1 Dipartimento di Farmacia, Università degli Studi di Genova, Viale Benedetto XV, 3, 16132 Genova, Italy; [email protected] (B.T.); [email protected] (V.B.); [email protected] (F.S.) 2 Dipartimento di Scienze Farmaceutiche, Università degli Studi di Milano, Via Mangiagalli 25, 20133 Milano, Italy 3 Dipartimento di Scienze Biomediche Chirurgiche e Odontoiatriche, Università degli Studi di Milano, Via Pascal 36, 20133 Milano, Italy; [email protected] 4 Dipartimento di Scienze Biomediche per la Salute, Università degli Studi di Milano, Via Mangiagalli 31, 20133 Milano, Italy; [email protected] 5 Molecular Biology and Nanotechnology Laboratory (MolBNL@UniTS), DEA, Piazzale Europa 1, 34127 Trieste, Italy; [email protected] (E.L.); [email protected] (S.P.) 6 Department of General Biophysics, Faculty of Biology and Environmental Protection, University of Lodz, 90-236 Lodz, Poland * Correspondence: [email protected] (M.T.); [email protected] (A.S.); [email protected] (N.B.) Received: 4 October 2020; Accepted: 21 October 2020; Published: 25 October 2020 Abstract: Leishmaniases are neglected diseases that are endemic in many tropical and sub-tropical Countries. Therapy is based on different classes of drugs which are burdened by severe side effects, occurrence of resistance and high costs, thereby creating the need for more efficacious, safer and inexpensive drugs. -

N-Alkylamino Derivates of Aromatic, Tricyclic Compounds in the Treatment of Drug-Resistant Protozoal Infections
Europaisches Patentamt 0 338 532 European Patent Office Qv Publication number: A2 Office europeen des brevets EUROPEAN PATENT APPLICATION 31/54 © Application number: 89107027.8 © mt.ci.4.A61K 31/38 , A61K @ Date of filing: 19.04.89 © Priority: 20.04.88 US 183858 © Applicant: MERRELL DOW 12.09.88 US 243524 PHARMACEUTICALS INC. 2110 East Galbraith Road @. Date of publication of application: Cincinnati Ohio 45215-6300(US) 25.10.89 Bulletin 89/43 © Inventor: Bitonti, Alan J. © Designated Contracting States: 7854 Carraway Court AT BE CH DE ES FR GB GR IT LI LU NL SE Maineville Ohio 45039(US) Inventor: McCann, Peter P. 3782 Cooper Road Cincinnati Ohio 45241 (US) Inventor: Sjoerdsma, Albert 5475 Waring Drive Cincinnati Ohio 45243(US) © Representative: Vossius & Partner Siebertstrasse 4 P.O. Box 86 07 67 D-8000 Munchen 86(DE) © N-alkylamino derivates of aromatic, tricyclic compounds in the treatment of drug-resistant protozoal infections. © Drug-resistant protozoal infection, particularly, drug-resistant malarial infection in humans, can be effectively treated with standard antiprotozoal agents if administered in conjunction with a tricyclic N-aminoalkyi iminodiben- zyl, dibenzylcycloheptane and cycloheptene, phenothiazine, dibenzoxazepine, dibenzoxepine, or thioxanthene derivative. CM < CM CO in oo CO CO LU Xerox Copy Centre EP 0 338 532 A2 N-ALKYLAMINO DERIVATIVES OF AROMATIC, TRICYCLIC COMPOUNDS IN THE TREATMENT OF DRUG- RESISTANT PROTOZOAL INFECTIONS This invention relates to the use of certain N-(aminoalkyl) derivatives of iminodibenzyl, dibenzyl- cycioheptane and cycloheptene, phenothiazine, dibenzoxazepine, dibenzoxepine, and thioxanthene in the treatment of drug-resistant malaria and in the treatment of other drug-resistant protozoal infections. -

Review of Pharmacokinetics and Pharmacogenetics in Atypical Long-Acting Injectable Antipsychotics
pharmaceutics Review Review of Pharmacokinetics and Pharmacogenetics in Atypical Long-Acting Injectable Antipsychotics Francisco José Toja-Camba 1,2,† , Nerea Gesto-Antelo 3,†, Olalla Maroñas 3,†, Eduardo Echarri Arrieta 4, Irene Zarra-Ferro 2,4, Miguel González-Barcia 2,4 , Enrique Bandín-Vilar 2,4 , Victor Mangas Sanjuan 2,5,6 , Fernando Facal 7,8 , Manuel Arrojo Romero 7, Angel Carracedo 3,9,10,* , Cristina Mondelo-García 2,4,* and Anxo Fernández-Ferreiro 2,4,* 1 Pharmacy Department, University Clinical Hospital of Ourense (SERGAS), Ramón Puga 52, 32005 Ourense, Spain; [email protected] 2 Clinical Pharmacology Group, Institute of Health Research (IDIS), Travesía da Choupana s/n, 15706 Santiago de Compostela, Spain; [email protected] (I.Z.-F.); [email protected] (M.G.-B.); [email protected] (E.B.-V.); [email protected] (V.M.S.) 3 Genomic Medicine Group, CIMUS, University of Santiago de Compostela, 15782 Santiago de Compostela, Spain; [email protected] (N.G.-A.); [email protected] (O.M.) 4 Pharmacy Department, University Clinical Hospital of Santiago de Compostela (SERGAS), Citation: Toja-Camba, F.J.; 15706 Santiago de Compostela, Spain; [email protected] Gesto-Antelo, N.; Maroñas, O.; 5 Department of Pharmacy and Pharmaceutical Technology and Parasitology, University of Valencia, Echarri Arrieta, E.; Zarra-Ferro, I.; 46100 Valencia, Spain González-Barcia, M.; Bandín-Vilar, E.; 6 Interuniversity Research Institute for Molecular Recognition and Technological Development, -
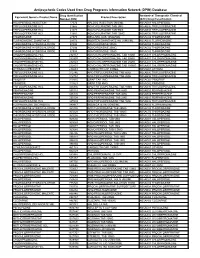
Antipsychotic Codes Used from Drug Programs Information Network (DPIN) Database
Antipsychotic Codes Used from Drug Programs Information Network (DPIN) Database Drug Identification Anatomical Therapeutic Chemical Equivalent Generic Product Name Product Description Number (DIN) (ATC) Drug Classification HALOPERIDOL INJECTION 17574 HALDOL INJECTION 5MG/ML N05AD01 HALOPERIDOL TRIFLUOPERAZINE HCL 21865 NOVO-FLURAZINE TAB 2MG N05AB06 TRIFLUOPERAZINE TRIFLUOPERAZINE HCL 21873 NOVO-FLURAZINE TAB 5MG N05AB06 TRIFLUOPERAZINE TRIFLUOPERAZINE HCL 21881 NOVO-FLURAZINE TAB 10MG N05AB06 TRIFLUOPERAZINE THIORIDAZINE 27375 MELLARIL SUS 10MG/5ML N05AC02 THIORIDAZINE FLUPHENAZINE ENANTHATE 29173 MODITEN ENANTHATE INJ 25MG/ML N05AB02 FLUPHENAZINE THIORIDAZINE HYDROCHLORIDE 37486 NOVO-RIDAZINE 50MG N05AC02 THIORIDAZINE THIORIDAZINE HYDROCHLORIDE 37494 NOVO-RIDAZINE 25MG N05AC02 THIORIDAZINE THIORIDAZINE HYDROCHLORIDE 37508 NOVO-RIDAZINE 10MG N05AC02 THIORIDAZINE CHLORPROMAZINE HCL 232157 NOVO-CHLORPROMAZINE TAB 10MG N05AA01 CHLORPROMAZINE CHLORPROMAZINE HCL 232807 NOVO-CHLORPROMAZINE TAB 50MG N05AA01 CHLORPROMAZINE CHLORPROMAZINE HCL 232823 NOVO-CHLORPROMAZINE TAB 25MG N05AA01 CHLORPROMAZINE CHLORPROMAZINE HCL 232831 NOVO-CHLORPROMAZINE TAB 100MG N05AA01 CHLORPROMAZINE LITHIUM CARBONATE 236683 CARBOLITH CAP 300MG N05AN01 LITHIUM TRIFLUOPERAZINE HCL 312746 APO TRIFLUOPERAZINE TAB 5MG N05AB06 TRIFLUOPERAZINE TRIFLUOPERAZINE HCL 312754 APO TRIFLUOPERAZINE TAB 2MG N05AB06 TRIFLUOPERAZINE PIMOZIDE 313815 ORAP TAB 2MG N05AG02 PIMOZIDE PIMOZIDE 313823 ORAP TAB 4MG N05AG02 PIMOZIDE TRIFLUOPERAZINE HCL 326836 APO TRIFLUOPERAZINE TAB 10MG N05AB06 -

Guidance on the Treatment of Antipsychotic Induced Hyperprolactinaemia in Adults
Guidance on the Treatment of Antipsychotic Induced Hyperprolactinaemia in Adults Version 1 GUIDELINE NO RATIFYING COMMITTEE DRUGS AND THERAPEUTICS GROUP DATE RATIFIED April 2014 DATE AVAILABLE ON INTRANET NEXT REVIEW DATE April 2016 POLICY AUTHORS Nana Tomova, Clinical Pharmacist Dr Richard Whale, Consultant Psychiatrist In association with: Dr Gordon Caldwell, Consultant Physician, WSHT . If you require this document in an alternative format, ie easy read, large text, audio, Braille or a community language, please contact the Pharmacy Team on 01243 623349 (Text Relay calls welcome). Contents Section Title Page Number 1. Introduction 2 2. Causes of Hyperprolactinaemia 2 3. Antipsychotics Associated with 3 Hyperprolactinaemia 4. Effects of Hyperprolactinaemia 4 5. Long-term Complications of Hyperprolactinaemia 4 5.1 Sexual Development in Adolescents 4 5.2 Osteoporosis 4 5.3 Breast Cancer 5 6. Monitoring & Baseline Prolactin Levels 5 7. Management of Hyperprolactinaemia 6 8. Pharmacological Treatment of 7 Hyperprolactinaemia 8.1 Aripiprazole 7 8.2 Dopamine Agonists 8 8.3 Oestrogen and Testosterone 9 8.4 Herbal Remedies 9 9. References 10 1 1.0 Introduction Prolactin is a hormone which is secreted from the lactotroph cells in the anterior pituitary gland under the influence of dopamine, which exerts an inhibitory effect on prolactin secretion1. A reduction in dopaminergic input to the lactotroph cells results in a rapid increase in prolactin secretion. Such a reduction in dopamine can occur through the administration of antipsychotics which act on dopamine receptors (specifically D2) in the tuberoinfundibular pathway of the brain2. The administration of antipsychotic medication is responsible for the high prevalence of hyperprolactinaemia in people with severe mental illness1. -

< MOH Approved Drugs List >
Ministry Of Health Directorate General of Medical Supplies Rep_Id : App_Drugs_List_Who.rdf < MOH Approved Drugs List > DATE : 12/08/2009 Page : 1 of 108 VED Flag <S.No> < Item Code > < I T E M D E S C ROF I P- T I O N > < U N I T > DATE : ABC Flag H/C Flag Category : DRUGS 1 Ph. System : GASTRO-INTESTINAL SYSTEM 1 Main Group : ANTACIDS 1 Sub Group : ALUMINIUM COMPOUNDS 1 03000000105 ALUMINIUM HYDROXIDE GEL, DRIED 475 MG. CAPSULE Desirable Cat_C Not H/C Item 2 Sub Group : ANTACID COMPOUND PREPARATIONS 2 02000000079 ANTACID SUSPENSION (ALUMINIUM HYDROXIDE + BOTTLE Desirable MAGNESIUM HYDROXIDE OR TRISILICATE) 100 - 200 Cat_A ML. B0TTLE. H/C Item 3 03000000173 ANTACID TABLET (ALUMINIUM HYDROXIDE + TABLET/CAP Desirable MAGNESIUM HYDROXIDE OR TRISILICATE). Cat_A H/C Item 2 Main Group : ANTISPASMODICS 1 Sub Group : ANTIMUSCARINICS 4 01000000304 HYOSCINE N BUTYLBROMIDE 20MG/ML. 1ML. AMPOULE Essantial Cat_A H/C Item 5 03000000640 HYOSCINE N BUTYL BROMIDE 10MG. TABLET/CAP Essantial Cat_A H/C Item 6 020D0000063 ANTISPASMODIC DROPS 15ML-25ML. BOTTLE Desirable Cat_C Not H/C Item 2 Sub Group : OTHER ANTISPASMODIC AND MOTILITY STIMULANT 7 03000001245 MEBEVERINE HYDROCHLORIDE 100 MG - 135 MG. TABLET/CAP Essantial Cat_B Not H/C Item Ministry Of Health Directorate General of Medical Supplies Rep_Id : App_Drugs_List_Who.rdf < MOH Approved Drugs List > DATE : 12/08/2009 Page : 2 of 108 VED Flag <S.No> < Item Code > < I T E M D E S C ROF I P- T I O N > < U N I T > DATE : ABC Flag H/C Flag Category : DRUGS 1 Ph.