Return of Organization Exempt from Income
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pirates Theaters 010308
The Pirates Who Don't Do Anything - A VeggieTales Movie - - - In Theaters January 11th Please note: This list is current as of January 3, 2008 and is subject to change. Additional theaters are being added over the next few days, so be sure to check back later for an updated list. To arrange for group ticket sales, please call 1-888-863-8564. Thanks for your support and we'll see you at the movies! Theater Address City ST Zip Code Sunridge Spectrum Cinemas 400-2555 32nd Street NE Calgary AB(CAN) T1Y 7X3 Scotiabank Theatre Chinook (formerly Paramoun 6455 Macleod Trail S.W. Calgary AB(CAN) T2H 0K4 Empire Studio 16 Country Hills 388 Country Hills Blvd., N.E. Calgary AB(CAN) T3K 5J6 North Edmonton Cinemas 14231 137th Avenue NW Edmonton AB(CAN) T5L 5E8 Clareview Clareview Town Centre Edmonton AB(CAN) T5Y 2W8 South Edmonton Common Cinemas 1525-99th Street NW Edmonton AB(CAN) T6N 1K5 Lyric 11801 100th St. Grande Prairie AB(CAN) T8V 3Y2 Galaxy Cinemas Lethbridge 501 1st. Ave. S.W. Lethbridge AB(CAN) T1J 4L9 Uptown 4922-49th Street Red Deer AB(CAN) T4N 1V3 Parkland 7 Cinemas 130 Century Crossing Spruce Grove AB(CAN) T7X 0C8 Dimond Center 9 Cinemas 800 Dimond Boulevard Anchorage AK 99515 Goldstream Stadium 16 1855 Airport Road Fairbanks AK 99701 Grand 14 820 Colonial Promenade Parkway Alabaster AL 35007 Cinemagic Indoor 1702 South Jefferson Street Athens AL 35611 Wynnsong 16-Auburn 2111 East University Drive Auburn AL 36831 Trussville Stadium 16 Colonial Promenade Shopping Center Birmingham AL 35235 Lee Branch 15 801 Doug Baker Blvd. -

Urban Land Institute Advisory Services Panel June 24-29, 2007
San Bernardino, California San Bernardino Crossroads of the Southwest California Urban Land Institute Urban Land Advisory Services Panel Institute June 24-29, 2007 Advisory Services Panel June 24-29, 2007 San Bernardino Our Sincere Thanks to California • Mayor Patrick J. Morris and staff • Chairman Paul Biane and staff Urban Land • The members of the City Council Institute • The members of the County Board of Supervisors • Other elected city officials • The City’s Economic Development Agency • Citizen leaders / Interviewees Advisory Services Panel June 24-29, 2007 San Bernardino Urban Land Institute California • Established in 1936 Urban Land • Independent non-profit Institute education and research organization • More than 37,000 members worldwide The mission of the Urban Land Institute is to provide leadership in the • Representing the entire responsible use of land and spectrum of land use, in creating and sustaining architecture, planning, thriving communities worldwide. Advisory academic and real estate Services Panel development disciplines June 24-29, 2007 San Bernardino ULI Advisory Services California • Applies the finest expertise in real estate, market analysis, land planning and public policy to Urban Land complex land use and development projects Institute • All volunteer, independent panel • Over 400 ULI-member teams assembled worldwide since 1947 to assist sponsors find creative and practical solutions. Approximately 15 national and international advisory panels per year Advisory Services Panel June 24-29, 2007 San Bernardino -
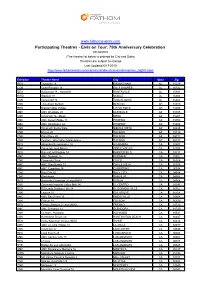
Participating Theatres
www.fathomevents.com Participating Theatres - Elvis on Tour: 75th Anniversary Celebration 07/29/2010 (The theatre list below is ordered by City and State) Theatres are subject to change Last Updated 6/17/2010 http://www.fathomevents.com/concertsandmusic/event/elvisontour_night1.aspx Exhibitor Theatre Name City State Zip REG Trussville 16 BIRMINGHAM AL 35235 COB Cobb Pinnacle 14 GULF SHORES AL 36542 REG Hollywood 18 - Huntsville HUNTSVILLE AL 35801 HWD Stadium 18 MOBILE AL 36606 COB Hollywood 16 TUSCALOOSA AL 35405 CNK Tinseltown Benton BENTON AR 72019 REG Breckenridge Village LITTLE ROCK AR 72205 AMC AMC Westgate 20 GLENDALE AZ 85305 CNK Cinemark 16 - Mesa MESA AZ 85201 AMC AMC Desert Ridge 18 PHOENIX AZ 85050 AMC AMC Ahwatukee 24 PHOENIX AZ 85044 CNK Cinemark Sierra Vista SIERRA VISTA AZ 85635 CNK El Con 20 TUCSON AZ 85716 CNK Park Place 20 TUCSON AZ 85711 CNK Century - Oro Valley Marketplace TUCSON AZ 85737 REG Alhambra Renaissance 14 ALHAMBRA CA 91801 CNK Cinemark Jess Ranch APPLE VALLEY CA 92308 REG Bakersfield Stadium 14 BAKERSFIELD CA 93311 AMC AMC Burbank 16 BURBANK CA 91502 CNK Cinemark Chico CHICO CA 95926 AMC AMC Otay Ranch 12 CHULA VISTA CA 91915 AMC AMC Cupertino 16 CUPERTINO CA 95014 CNK Daly City 20 DALY CITY CA 94014 CNK Blackhawk DANVILLE CA 94506 REG Hacienda Crossings 20 plus IMAX DUBLIN CA 94568 CNK Cinemark Imperial Valley Mall 14 EL CENTRO CA 92243 REG El Dorado Stadium Hills 14 EL DORADO HILLS CA 95762 CNK Laguna 16 ELK GROVE CA 95758 AMC AMC Bay Street 16 EMERYVILLE CA 94608 CNK Folsom 14 FOLSOM CA 95630 REG Fresno -
BUS BOOK MECH B 11/29/10 3:09 PM Page 1
BUS BOOK MECH B 11/29/10 3:09 PM Page 1 C M Y CM MY CY CMY K BUSRoutes and Schedules Effective January 3,BOOK 2011 to May 2, 2011 RESOLVE TO RIDE. 1-800-9-OMNIBUS OMNITRANS.ORG Welcome Aboard! Table of Contents Pass Outlets 2-3 Expendios de pases Passes by Mail 96 Pases por correo Fare Information 4-6 Información del precio Calendar 3 Calendario How to Ride 7-10 Cómo Viajar Transfer Centers 11-13 Centros de transbordo Destinations 14 Destinos Telephone Numbers 15 Números de teléfono Bike & Ride 16 Pedalear y viajar Wheelchair Lift 17 Elevador para sillas de ruedas Route Maps & Schedules 18-91 Mapas y horarios de rutas Access, Omnilink 92 - 95 Access, Omnilink WHAT’S NEW NOVEDADES What’s new for January? Only minor changes to a few of ¿Qué hay de nuevo para enero? Solo cambios menores a our routes. Maps for Routes 3-4 and 82 will reflect minor algunos de nuestros recorridos. Los mapas de los changes in routing and service enhancements. recorridos 3-4 y 82 reflejarán cambios menores en los recorridos y mejoras del servicio. Routes 3-4 Run time changes to all days. Routing El horario del recorrido de las rutas 3-4 ha cambiado around the 4th Street Transit Mall has been altered and para todos los días. El recorrido por 4th Street Transit the time point has been moved to Court and E Streets. Mall ha sido modificado y el cartel con los horarios ha sido llevado a las calles Court y E Street. -

Andrew Hernandez Named '97 National Veterans Small Busi Ness Advocate of the Year We Proudly Salute the 1997 Educatiou Medal of Houor Recipieuts
California State University, San Bernardino CSUSB ScholarWorks Inland Empire Hispanic News Special Collections & University Archives 6-11-1997 June 11th 1997 Hispanic News Follow this and additional works at: https://scholarworks.lib.csusb.edu/hispanicnews Recommended Citation Hispanic News, "June 11th 1997" (1997). Inland Empire Hispanic News. 130. https://scholarworks.lib.csusb.edu/hispanicnews/130 This Article is brought to you for free and open access by the Special Collections & University Archives at CSUSB ScholarWorks. It has been accepted for inclusion in Inland Empire Hispanic News by an authorized administrator of CSUSB ScholarWorks. For more information, please contact [email protected]. nSMBMBER YOUn "BAD’' ON FATHER'S 0/^% SUNDAY, JUNE IS A Publication of the BULK RATE Hispanic Communication & -rmn- U.S. POSTAGE Development Corporation PAID San Bsrnardtno, CA PERMIT No. 118 Wednesday INLAND EMPIRE June 11,1997 4^ P Volume 10 O Number 21 Hispanic Ne\ -1 ■'c Serving the Hispanic Communities in the Inla pire ' San Bernardino • Colton • Rialto • Bloomington • Redlands • Fontana • Rancho Cucamonga • Ontario • Victorville • Riverside • Casa Blanca • Moreno Valley • Corona • Perris Tho Inlond Empire's Only Hispenic Minority Owned English Langusge Newspaper r. Albert K. Karnig to take over reins at Inland Empire Citizens honored by the Ameri §al State, San Bernardino in August can Heart Association, Western States Divi the advancement of higher education is sion for exemplary service to the community quite clear. We are very pleased that he will be bringing those qualities to San Bernardino.” Karnig, 55, has served in his current position since 1988. He is responsible for various academic activities includ ing programs and instruction, budget ing processes, diversity initiatives and outcomes, outreach programs and academic planning and standards. -

Part 3 Outreach
Part 3 Outreach The opportunities and constraints are viewed through the lens of High Quality Transit Areas and the principles of transit-oriented communities. Stakeholder Interviews Kick-off Meeting Executive Summary Station Area Profile Outreach Opportunities/Constraints HQTA Kick-off Meeting - 3/13/2018 STAKEHOLDER INTERVIEWS A kickoff meeting was held for the SCAG HQTA Pilot Project within the City of San Bernardino. - General Plan The purpose of this meeting was to bring together City of San Bernardino, Omnitrans, - Last completed in 2005 – missing many of the elements expected for a General SBCTA, SCAG, and the consultant team to discuss coordination and direction of the project. Plan developed today (bicycle and pedestrian focus, etc.) The meeting consisted of introductory comments from the City of San Bernardino and - Potential for General Plan update SCAG followed by a presentation by the consultant team to facilitate discussion of multiple - Would include update of focus area for Downtown topics. Topics of discussion included project goals, the vision plan process and work plan, - If funding not made available for citywide General Plan update, a new stakeholder/community outreach, project area, existing conditions, data requests, and the Specific Plan for Downtown to be developed schedule. The following is a summary of the main discussion items. - Draft Downtown Specific Plan - Draft Downtown Specific Plan developed with AECOM no longer valid Introductory Remarks and Overall Goals - Reconnecting the street grid and adding residential -

Sam Goo GOODY GOT IT
Two distinctly different records. Get them both at Goody. Sam Goo GOODY GOT IT Sale ends February 2nd, Arcadia ................._.........Santa Anita Fashion Park Los Angeles Westside Pavilion Thousand Oaks The Oaks Shoplmg Co. Brea Brea Mall Manhattan Beach ....Manhattan Village Torrance Del Amo Fasllon Clr Buena Pars. Buena Park Mall Mission Viejo ...Mission Vrelo Mall ' Ventura ....... 4020 E. .lain SI. Canoga Pak Fall :rook Square Montclair ....Montclair Plaza Viutorwlle ... ............ Mall AI Vicar Valley Canoga Park To nga Plaza Montebello ... .....Montebello Town Center West Covina The Plaza At Wes Covina Canoga Pk.... .... 6537 Topanga CanyonP Blvd. Newport Beach ....... ...Fashion Island Westminster Westmin_ter Mall Cerritos Los Cerritos Ctr. North Hollywood ..:.... .12012 Victory Blvd. Whittier 15250 Whiter Al Culver CIIr. Fox Hills Mall Northridge...... ..... Northridge Fash Ctr. Whittier ..... ...Whittwaod Mall Costa Mesa South Coast Plaza Orange .............................. .....Man 01 Orange Woodland Hills Prime Pt. Plaza Cypress 6927 Katella Avenue Palmdale Antelope Valley Mall Glendale .........................................Glendale Gallería Palm Desert ............................ Palm Desert Town Clr. Hawthorn ...............Hawthorne Plaza Pasadena......... ... .....Plaza Pasadena Hornet ........Hemet Valley Mall Redondo Ouch Galleria At South Bay Also available at Huntington Beach 16071 Golden West Sr. Riverside ........ ...Gallería at Tyler Huntington Beach 10111.A Adams Avenue ' Riverside _. ......3764 Tyler -

Part 2 Station Area Profile
Part 2 Station Area Profile The Station Area Profile is a summary of some of the physical and regulatory conditions currently existing within the study area. Overview San Bernardino High Quality Transit Area Downtown San Bernardino Transit Center Socioeconomic Profile Demographic Profile Employment Profile Employment Trends Previous Planning Efforts Executive Summary Station Area Profile Outreach Opportunities/Constraints San Bernardino High Quality Transit Area OVERVIEW The City of San Bernardino’s HQTA is centrally located in the City’s downtown core, which includes the new San Bernardino Regional Transit Center and the now closed Carousel Mall. The HQTA is as represented in the map at right. It currently includes stops for the San Bernardino Express (SbX) Bus Rapid Transit line, regional and local buses, stops for Metrolink, and stops for the future Redlands Passenger Rail “Arrow” transit line, providing multi-modal access to Downtown San Bernardino. The City has adopted a TOD overlay zone for all properties within half-mile of their SbX BRT stops and will prepare a Downtown Specific 1/2 Mile radius Plan to incorporate TOD principles. The area is about three miles north of Hospitality Lane, which includes a cluster of hospitality and employment activities. HR&A has defined a study area around the center of the Carousel Mall as the Study Area for socio-economic and demographic profile presented on pages 10-12. In addition to the Mall, Theater the Study Area includes a large number of City offices and County facilities, as well as the Courthouse Square 8,000 seat San Manuel Stadium, home of the Inland Empire 66ers, a San Bernardino-based Caltrans minor league baseball team. -

Branding, Development, & Marketing Action Plan
Stockton, California July 2008 Downtown Stockton is the destination of choice when you want to celebrate life, art, food, music, sports, theater, and recreation. What would you like to celebrate this weekend? Branding, Development, & Marketing Action Plan 2 Stockton, California July 2008 Contents The Stockton brand ....................................................................................................................................................................................................................... 5 Executive Summary & brand direction ........................................................................................................................................................................................ 9 Summary Charts ............................................................................................................................................................................................................................ 20 Introduction and scope of work ................................................................................................................................................................................................... 27 Strengths, weaknesses, opportunities & threats ........................................................................................................................................................................... 31 RECOMMENDATIONS #1. Commit to the brand .......................................................................................................................................................................................................... -

SAN BERNARDINO COUNTY Business Growth OPPORTUNITIES
(REV. MAY 2019) SAN BERNARDINO COUNTY Business Growth OPPORTUNITIES DEVELOPMENT www.SelectSBCounty.com1 2 TO LAS VEGAS COUNTY OF SAN BERNARDINO BARSTOW ADELANTO VICTORVILLE TO LAUGHLIN APPLE VALLEY NEEDLES HESPERIA BIG BEAR LAKE UPLAND LAKE ARROWHEAD TWENTYNINE PALMS RANCHO CUCAMONGA YUCCA VALLEY MONTCLAIR FONTANA RIALTO YUCAIPA ONTARIO REDLANDS ONT AIRPORT SAN BERNARDINO CHINO COLTON HIGHLAND CHINO HILLS LOMA LINDA LOS ANGELES GRAND TERRACE COUNTY RIVERSIDE COUNTY ORANGE 3 COUNTY 3 Business Growth OPPORTUNITIES CITY CONTACTS 5 UNINCORPORATED AREA SHOPPING CENTERS 6–10 ADELANTO 12 APPLE VALLEY 13 BARSTOW 14 BIG BEAR LAKE 15 CHINO 16 CHINO HILLS 17 COLTON 18 FONTANA 19 GRAND TERRACE 20 HESPERIA 21 HIGHLAND 22 LOMA LINDA 23 MONTCLAIR 24 NEEDLES 25 ONTARIO 26 RANCHO CUCAMONGA 27 REDLANDS 28 RIALTO 29 SAN BERNARDINO 30 TWENTYNINE PALMS 31 UPLAND 32 VICTORVILE 33 YUCAIPA 34 YUCCA VALLEY 35 RDA 36–41 DISCLAIMER 42 Table of 2019 Contents Table 4 www.SelectSBCounty.com SEIZE THE ADVANTAGE 2019 San Bernardino County Economic Development Agency | 385 N. Arrowhead Avenue, Third Floor | San Bernardino, CA 92415 | Phone: 909.387.4700 | Fax: 909.387.4415 CITY CONTACTS ADELANTO CHINO HILLS LOMA LINDA REDLANDS (CONT.) VICTORVILLE Jessie Flores Joann Lombardo T Jarb Thaipejr Cruz Esparza IV Keith C. Metzler City Manager Community Development Director City Manager Economic Development Manager City Manager 760.246.2300 909.364.2740 909.799.2810 909.335.4755 ext. 1 760.955.5029 [email protected] [email protected] [email protected] [email protected] [email protected] Charles Rangel Yvette Brunetto Konrad Bolowich RIALTO Sophie L. -
Macy's East SMALL TICKET DEPARTMENTS Store/DC List As of May 4, 2008 Page 1 of 19 As of 3/10/2008
Macy's East SMALL TICKET DEPARTMENTS Store/DC List as of May 4, 2008 Current Current New New DC Division Store Division Store DC Alpha Effective Name Number Name Number Name Code Mall Name / Store Name Address City State Zip Date Macy's North 0001 Macy's East 0301 Minooka CL Somerset Collection 2750 West Big Beaver Rd Troy MI 48084 5/4/2008 Macy's North 0002 Macy's East 0302 Minooka CL Twelve Oaks (Novi) 27550 Novi Rd Novi MI 48377 5/4/2008 Macy's North 0003 Macy's East 0303 Minooka CL Oakland (MI) 500 W 14 Mile Rd Troy MI 48083 5/4/2008 Macy's North 0004 Macy's East 0304 Minooka CL Lakeside (MI) 14200 Lakeside Circle Sterling Heights MI 48313 5/4/2008 Macy's North 0005 Macy's East 0305 Minooka CL Briarwood 700 Briarwood Circle Ann Arbor MI 48108 5/4/2008 Macy's North 0006 Macy's East 0306 Minooka CL Eastland Center (Detroit) 18000 Vernier Rd Harper Woods MI 48225 5/4/2008 Macy's North 0007 Macy's East 0307 Minooka CL Woodland (MI) 3165 28th St SE Kentwood MI 49512 5/4/2008 Macy's North 0008 Macy's East 0308 Minooka CL Genesee Valley Center 4600 Miller Rd Flint MI 48507 5/4/2008 Macy's North 0009 Macy's East 0309 Minooka CL Southland (MI) 23000 Eureka Rd Taylor MI 48180 5/4/2008 Macy's North 0010 Macy's East 0310 Minooka CL Westland (MI) 35000 West Warren Ave Westland MI 48185 5/4/2008 Macy's North 0011 Macy's East 0311 Minooka CL Northland Center 21500 Northwestern Hwy Southfield MI 48075 5/4/2008 Macy's North 0012 Macy's East 0312 Minooka CL Fairlane Town Center 18900 Mighican Ave Dearborn MI 48126 5/4/2008 Macy's North 0013 Macy's -

Part 4 Opportunities and Constraints Analysis
Part 4 Opportunities and Constraints Analysis The opportunities and constraints are viewed through the lens of High Quality Transit Areas and the principles of transit-oriented communities. Mobility Land Use Urban Design Executive Summary Station Area Profile Outreach Opportunities/Constraints Constraints MOBILITY I-215: I-215 is among the most significant physical features in Downtown San Bernardino. While it provides for the movement of vehicles through the city, it produces significant negative impacts for local residents and workers including air pollution and noise pollution. It is also a barrier to accessing downtown from west. I-215 Access: Traffic congestion at on-/off-ramps. Hazardous for bicyclists and pedestrians as drivers are unaware, focused on accessing highway, and/or in a rush. Poor visibility for pedestrians and bicyclists due to highway over crossings. Vehicle-oriented Corridors: Barriers to cross (physical and psychological), as well as unpleasant for pedestrians and bicycles to travel along. While they may have among highest traffic volumes in Downtown, they are also over-designed based on recorded and observed traffic volumes. Vehicle corridors mostly travel east-west and correspond with I-215 access (except Rialto Avenue). Limited Connectivity Across Rail Corridor: D Street is planned to be reconfigured with 1 a cul-da-sac on the north and south sides of the rail corridor, closing access to vehicle and pedestrians. Remaining rail crossings for vehicles and pedestrians occur at-grade at G Street, E Street, and Arrowhead Avenue. Limited Connectivity Across I-215: Street crossings occur at 3rd Street, 2nd Street, and Rialto Avenue. I-215 crossing at 5th Street occurs via bridge.