Democratic Republic of Timor Leste Country Profile for Emergencies and Disasters
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Responsibility and Accountability
Part 8: Responsibility and Accountability Part 8: Responsibility and Accountability ..............................................................................................1 Part 8: Responsibility and Accountability ..............................................................................................2 8.1 Introduction ..................................................................................................................................2 8.2 Principal findings..........................................................................................................................5 8.3 Methodology for identification of institutional responsibility.....................................................11 8.4 Responsibility and accountability of the Indonesian security forces .......................................15 High-level responsibility........................................................................................................................51 The scale of violations:.........................................................................................................................52 The pattern of violations.......................................................................................................................52 Strategy.................................................................................................................................................52 Institutional norms and culture.............................................................................................................53 -

Walking in Hato Builico Timor Leste
Blue Mountains East Timor Friendship Committee The Friendship Committee was formed in 2006 as part of an Australia-wide initiative to develop friendship agreements with communities in Timor-Leste. To date, more than 40 councils across Australia have participated. Walking in Hato Builico The Blue Mountains committee is made up of community members, councillors and council staff from Blue Mountains City Council, all committed to improving the lives of the rural community of Hato Builico. A partner committee of residents of Hato Timor Leste Builico assesses the needs of the community and liaises with the Blue Mountains to progress projects. Fundraising events are organised regularly by volunteers. If you live in or plan to visit Australia in 2012, what about raising funds for Hato Builico by joining the sponsored Trek for Timor Blue Mountains on September 15th 2012. 50km or 15km - the choice is yours. www.trekfortimorbm.org.au Members of the Blue Mountains committee visit regularly on self-funded trips to monitor progress of projects and to talk to villagers about their needs. In 2011, a volunteer from Australian Volunteers International will spend extended periods in Hato Builico to work on local projects. Projects so far have included: Refurbishment of a community centre for training and community meetings Scholarships for 43 students to attend primary school, high school and university Collaborations between schools in East Timor and Blue Mountains Hedge seedlings to counteract the effects of deforestation Solar panels for the community centre Two water tanks for the community centre (supported by Rotary) Sports equipment, school equipment, readers and guitars for schools as well as participation in training for sports teaching And of course – this project! Two volunteers from the Blue Mountains spent three months living in Hato Builico and developing this series of guided walks. -
East Timor Law and Justice Bulletin (ETLJB), the Principal International NGO That Runs an HIV-AIDS Transmission Reduction Program Excludes Gays from Its Program
TIMOR-LESTE Timor-Leste is a multiparty parliamentary republic with a population of approximately 1.1 million. President Jose Ramos-Horta was head of state. Prime Minister Kay Rala Xanana Gusmao headed a four-party coalition government formed following free and fair elections in 2007. International security forces in the country included the UN Police (UNPOL) within the UN Integrated Mission in Timor-Leste (UNMIT) and the International Stabilization Force (ISF), neither of which was under the direct control of the government. The national security forces are the National Police (PNTL) and Defense Forces (F-FDTL). Security forces reported to civilian authorities, but there were some problems with discipline and accountability. Serious human rights problems included police use of excessive force during arrest and abuse of authority; perception of impunity; arbitrary arrest and detention; and an inefficient and understaffed judiciary that deprived citizens of due process and an expeditious and fair trial. Domestic violence, rape, and sexual abuse were also problems. RESPECT FOR HUMAN RIGHTS Section 1 Respect for the Integrity of the Person, Including Freedom From: a. Arbitrary or Unlawful Deprivation of Life There were no politically motivated killings by the government or its agents during the year; however, on August 27, F-FDTL soldiers were involved in a fight with locals in Laivai, Lautem, in which one civilian was beaten to death. The case was handed to the Prosecutor General's Office and the Human Rights Ombudsman for investigation. At year's end the investigation was ongoing. There were no developments in the May 2009 case in which a group of F-FDTL members allegedly beat two men on a beach in Dili; one of the victims was subsequently found dead. -

FOR OFFICIAL USE ONLY Report No: PAD3216 INTERNATIONAL
FOR OFFICIAL USE ONLY Report No: PAD3216 INTERNATIONAL DEVELOPMENT ASSOCIATION PROJECT APPRAISAL DOCUMENT ON A PROPOSED CREDIT IN THE AMOUNT OF SDR 42.5 MILLION (US$59.0 MILLION EQUIVALENT) TO THE DEMOCRATIC REPUBLIC OF TIMOR-LESTE FOR A TIMOR-LESTE BRANCH ROADS PROJECT November 1, 2019 Transport Global Practice East Asia And Pacific Region This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective June 30, 2019) Currency Unit = United States Dollar (US$) SDR 0.71932 = US$1 US$1.39021 = SDR 1 FISCAL YEAR January 1 - December 31 Vice President: Victoria Kwakwa Country Director: Rodrigo A. Chaves Regional Director: Ranjit Lamech Practice Manager: Almud Weitz Task Team Leader(s): Rodrigo Archondo-Callao, Elena Y. Chesheva ABBREVIATIONS AND ACRONYMS AADT Annual Average Daily Traffic ADB Asian Development Bank ADN Agência de Desenvolvimento Nacional (National Development Agency) CAFI Conselho de Administração do Fundo Infraestrutura (Council for the Administration of the Infrastructure Fund) CERC Contingent Emergency Response Component CESMP Contractor’s Environmental and Social Management Plan CO2 Carbon Dioxide DA Designated Account DED Detailed Engineering Design DFAT Department of Foreign Affairs and Trade DG Director General DRBFC Directorate of Roads, Bridges and Flood Control EIRR Economic Internal Rate of Return EMP Environmental Management Plan -

Timor-Leste Building Agribusiness Capacity in East Timor
Timor-Leste Building Agribusiness Capacity in East Timor (BACET) Cooperative Agreement 486-A-00-06-00011-00 Quarterly Report July 01 - September 30, 2010 Submitted to: USAID/Timor-Leste Dili, Timor-Leste Angela Rodrigues Lopes da Cruz, Agreement Officer Technical Representative Submitted by: Land O’Lakes, Inc. International Development Division P. O. Box 64281 St. Paul, MN 55164-0281 U.S.A. October 2010 © Copyright 2010 by Land O'Lakes, Inc. All rights reserved. Building Agribusiness Capacity in East Timor CA # 486-A-00-06-00011-00 BUILDING AGRIBUSINESS CAPACITY IN EAST TIMOR USAID CA# 486-A-00-06-00011-00 Quarterly Report July - September 2010 Name of Project: Building Agribusiness Capacity in East Timor Locations: Fuiloro, Lautem District Maliana, Bobonaro District Natarbora, Manatutu District Dates of project: September 22, 2006 – September 30, 2011 Total estimated federal funding: $6,000,000 Total federal funding obligated: $6,000,000 Total project funds spent to September 30, 2010: $5,150,425 Contact in Timor-Leste: Michael J. Parr, Chief of Party Telephone: +670 331-2719 Mobile: +670 735-4382 E-mail: [email protected] Summary: BACET directly contributes to USAID/Timor- Leste’s agriculture and workforce development strategies for economic growth. though categorized as a capacity building and workforce development activity, many of the key activities of BACET have included infrastructure improvements, which are longer-term in nature. Similarly, teacher training and changed teaching methods have long-term impact. Quarterly Report July - September 2010 Land O'Lakes, Inc. Building Agribusiness Capacity in East Timor CA # 486-A-00-06-00011-00 Table of Contents 1. -

World Bank Document
INTEGRATED SAFEGUARDS DATASHEET APPRAISAL STAGE I. Basic Information Date prepared/updated: 09/11/2012 Report No.: AC6721 Public Disclosure Authorized 1. Basic Project Data Original Project ID: P125032 Original Project Name: Timor Leste Road Climate Resilience Project Country: Timor-Leste Project ID: P130975 Project Name: Timor Leste Road Climate Resilience Project - Additional Financing Task Team Leader: Mitsuyoshi Asada Estimated Appraisal Date: April 30, 2012 Estimated Board Date: March 21, 2013 Managing Unit: EASNS Lending Instrument: Specific Investment Loan Sector: Rural and Inter-Urban Roads and Highways (85%);Public administration- Transportation (15%) Theme: Climate change (60%);Rural services and infrastructure (20%);Regional Public Disclosure Authorized integration (20%) IBRD Amount (US$m.): 30 IDA Amount (US$m.): 10 GEF Amount (US$m.): 0 PCF Amount (US$m.): 0 Other financing amounts by source: Borrower 52.00 52.00 Environmental Category: B - Partial Assessment Simplified Processing Simple [] Repeater [] Is this project processed under OP 8.50 (Emergency Recovery) Public Disclosure Authorized Yes [ ] No [X] or OP 8.00 (Rapid Response to Crises and Emergencies) 2. Project Objectives The project will deliver sustainable climate resilient road infrastructure on the Dili- Ainaro corridor. 3. Project Description The project would provide additional financing for the ongoing Timor Leste Road Climate resilience Project (TLRCRP). The proposed Additional Financing will finance the following revised components under RCRP: Component A: Climate Resilient Road Infrastructure This component will invest in key road infrastructure to improve its climate resilience. Public Disclosure Authorized The objective is to reduce the impact of the increasing traffic volume and intensity of rainfall on the road corridor from Dili to Ainaro. -

Project Brief: Enhancing Rural Access
Project Brief International Labour Organization Enhancing Rural Access (ERA) Objective To improve access and income opportunities for rural communities through rehabilitation and maintenance of rural roads by trained contractors. Key Partners Secretariat of State for Support and Promotion of Private Sector (SEAPRI) Ministry of Public Works (MPW) Don Bosco Foundation, Training Center in Comoro Instituto de Apoio ao Desenvolvimento Empresarial (IADE) Chambers of Commerce and Industry Timor-Leste (CCI-TL) Duration 4 years (2011 – 2015) Geographical Timor-Leste, Districts of Ainaro, Aileu, Bobonaro, Covalima, Ermera and Liquica Coverage Country Programme Enhanced rural employment, safety net, and economy through infrastructure investment Reference and private sector development. Donor The European Union Budget EUR 10,000,000 Contact Tomas Stenstrom | Project Chief Engineer | [email protected] Donato da Costa Pinheiro | Don Bosco Training Coordinator | [email protected] Project Background Timor-Leste is one of the least developed countries capacities, both in the private sector, in contract in the region. Its economy is essentially agriculture- management and in training delivery. Whilst the main based, with approximately 75% of its total population of objective of ERA is improved access through the about 1.1 million living in rural areas. A key constraint rehabilitation and maintenance of rural roads, this will to economic development is the poor condition of largely be done by local contractors trained in using a infrastructure in general, and the road network in labour-based approach. particular. Another serious structural problem of the economy is the inability to create employment Labour-based technology (LBT) optimizes the use of opportunities for the rapidly expanding labour force. -

3. Promotion of Community Reconciliation and Peacebuilding Process Through Development Projects
3. Promotion of Community Reconciliation and Peacebuilding Process through Development Projects War-affected communities possess particular mutual characteristics. The evaluation report on post-conflict humanitarian assistance prepared by UNDP and the Japanese government (2002) concludes that many features in post-conflict situations affect all humanitarian assistance projects: Lack of baseline data and lack of reliable information relating to damages and needs of the communities lead the requirement of modification in planning and budgeting of projects. Security issues and the difficulties of arranging logistics delay the projects. The presence of international organisations and personnel raises the prices of every product dramatically in the country and makes for an unnatural economy. This also increases the project budget. Short term contract of staff in international organisations in war-affected countries makes cooperation among humanitarian assistance organisations, as well as the sustainability of projects, difficult physically. In many cases, the recipient government and its administration system are not existing or not viable enough. And there are lack of techniques and the people who have special skills and techniques. This increases the dependency of the recipient countries on international assistance. This chapter will discuss how the development project could or should promote the community reconciliation and peacebuilding process at the community level. Firstly, the author will describe the development projects in Ainaro district. Secondly, the author will assess three particular development projects; aim, performance, implementation structure, relationship with local communities, relevance, efficiency, effectiveness, impact, sustainability, challenges and relation with promoting reconciliation process. Then discuss how the development project could or should promote the community reconciliation and peacebuilding process at the community level based on the lessons learned from project analysis in Ainaro. -

The General Prosecutor of the United Nations Transitiona& ) Administration
J~-- /', THE GENERAL PROSECUTOR OF THE UNITED NATIONS TRANSITIONA& ) ADMINISTRATION IN EAST TIMOR -' ~1 "-" AGAINST GASPAR LEITE I. INDICTMENT The General Prosecutor of the United Nations Transitional Administration in East Timor, pursuant to his authority under UNTAET Regulation 1999/1, 2000/11, 2000/15, 2000/16 and 2000/30 charges: GASPAR LEITE with MURDER As set forth in this indictment, the General Prosecutor requests the Special Panel for Serious Crimes of the District Court of Dili to take jurisdiction of this matter expeditiously. II. NAME AND PARTICULARS OF THE ACCUSED Name: Gaspar Leite Age: 43 Date of Birth: 6th March 1957 Place of Birth: Erolo, Aileu Nationality: East Timorese Location: Gleno Prison III. STATEMENT OF THE FACTS 1. On 30th August 1999 the people of East Timor voted in a referendLll11 for independence from the Republic of Indonesia. 2, Following the vote, there were attacks directed against the civilian population in, among other areas, the District of Aileu. 3. Within the District of Aileu is the village of HoHuLu. 4, By September 1999 Gaspar Leite had been a soldier with the TNI for about 9 years. During 1999 the TNI commander in the District of Aileu was Seargent Major Ali Cocoleo (Alikkokolok) of Kodim 1632. 5. On or about 8th September 1999 Ali Cocoleo (Alikkokolok) addressed a group of about twenty TNI personnel, including Gaspar Leite. Ali Cocoleo (Alikkokolok) gave instructions to the TNI personnel to attack the village of HoHuLu, to burn houses there and shoot people from the village. PURL: https://www.legal-tools.org/doc/51ab50/ ,r" i··-"')/ Io. -

53395-001: Water Supply and Sanitation Investment Project
Initial Environmental Examination March 2021 Timor-Leste: Water Supply and Sanitation Investment Project – Viqueque City Subproject (Part 1 of 5) Prepared by the Directorate General for Water and Sanitation, Ministry of Public Works for the Asian Development Bank. (page left Intentionally blank) i ABBREVIATIONS WSSIP - Water Supply and Sanitation Investment Project ACMs - Asbestos Containing Materials ADB - Asian Development Bank DED - Detailed Engineering Design DGAS - Directorate General for Water and Sanitation DNAP - National Directorate for Protected Areas DNCP - National Directorate for Pollution Control DNSA - National Directorate for Water Services EARF - Environmental Assessment and Review Framework EHS - Environment, Health and Safety EIA - Environmental Impact Assessment EIS - Environmental Impact Statement EMP - Environmental Management Plan EMR - Environmental Monitoring Report ESS - Environmental Safeguard Specialist ESA - Environmental Safeguard Assistant FSTP - Faecal Sludge Treatment Plant GRM - Grievance Redress Mechanism IEE - Initial Environmental Examination IFC - International Finance Corporation MPW - Ministry of Public Works PA - Protected Area PD - Project Document PDC - Project Design Consultant PSC - Project Supervision Consultant PMU - Project Management Unit SEA - Superior Environmental Authority SEIS - Simplified Environmental Impact Statement CEMP - Site-specific Construction EMP SMASA - Municipal Water, Sanitation and Environment Services SPS - Safeguard Policy Statement TOR - Terms of Reference WDZ - Water -
Aileu DPT Final.Indd
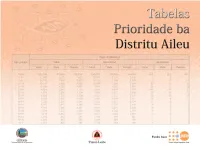
GLOSSÁRIU SENSUS TABELAS PRIORIDADE BA DISTRITU MANUFAHI NIAN 112 TTabelasa b e l a s PPrioridader i o r i d a d e bbaa DDistritui s t r i t u AileuA i l e u Testu © Kopiraite DNE ho UNFPA 2008 Direcção Nacional de Estatística (DNE) Fundu Populasaun Nasoens Unidas (UNFPA) i ii Y Y Y hsvs YY Y Y Y YY Y Y Y histriuisun2ptin2xe9eé2im2rel Y Y Y Y YYY YY YYYYYY gyEvs esYYY Y Y Y Y Y YY Y Y YYYYY YY YY Y Y Y YYYY Y YYY Y YYY YYY YY YYY YYY YY hss 2esvi Y YY YYY YYYY YYYY Y Y YY Y YY YY YYY YYY Y YY Y Y Y YY YY YYYY Y Y Y Y Y Y Y YYY Y Y Y YYY YYY Y YYYY Y Y Y Y YY Y Y YY Y Y Y Y Y YYYYYY YY Y Y Y YYY Y Y YYY evs Y YY YYYY YY YY YY Y Y Y YYYY YY Y Y Y Y Y YYY YY YY YY YYY YY YYYY YYYY Y YY Y Y YYYY YYYYYYYYY Y YY YYYY YYY Y Y Y Y Y YY Y YYY Y YY YY YY YYY Y YY Y Y Y Y Y Y Y ptinGum2xe9eé2em2hel YYY YY YYY Y Y Y YY YYYYYY YY Y YY Y Y Y Y YYYYYYYYYYYYYYY YY YY Y YYY Y Y Y Y YYYYYYYYYYYY Y Y YYY Y YYYYYY YYYYYYY Y YYYYYYYYYYYYYY Y YYYYY Y Y YYYYY YY YYYY Y YY YYYYYY vs sge Y Y Y YY Y Y YYY YYYYYY Y yspitál2no2ulínik Y YY Y YY YY ÑY Y Y vee iy Y Y Y Y YYYYY Y Y Y Y YYY Y YYYYYYYYYY YY YY YYY YY Y YY Y YYY Y Y Y Y eg we Y YYYY YY YYY Y YYY YYYY YYY Y YYY Y Y Y Y Y Y Y YY YY Y Y Y Y Y Y YY Y Y Y Y grg2@gommunity2relth2genterA Y Y YY Y Y Y gyyve Y Y YYYY Y YY Y entru2úde2uomunidde Y YY Y Y Y Y Y Y YY YYYY YY YY Y Y Y Y Y Y Y YY Y YYY Y YYY YY Y Y Y Y Y Y Y Y Y YYY Y Y Y Y Y Y Y Y Y YYY YY YY Y YYY Y YY YY Y YYYYY YYYYYYYYYYYY Y YYYYYY YY yr wieY Y YY Y YY YY YY Y Y fliz2uku YY YY Y YY Y iwisy Y Y Y YYYYY Y YY YYYYYYY YYY ve veeYY Y Y YY YY YY Y YY -
Fieldwork in Timor-Leste
Understanding Timor-Leste, on the ground and from afar (eds) and Bexley Nygaard-Christensen This ground-breaking exploration of research in Timor-Leste brings together veteran and early-career scholars who broadly Fieldwork in represent a range of fieldwork practices and challenges from colonial times to the present day. Here, they introduce readers to their experiences of conducting anthropological, historical and archival fieldwork in this new nation. The volume further Timor-Leste explores the contestations and deliberations that have been in Timor-Leste Fieldwork symptomatic of the country’s nation-building process, high- Understanding Social Change through Practice lighting how the preconceptions of development workers and researchers might be challenged on the ground. By making more explicable the processes of social and political change in Timor- Leste, the volume offers a critical contribution for those in the academic, policy and development communities working there. This is a must-have volume for scholars, other fieldworkers and policy-makers preparing to work in Timor-Leste, invaluable for those needing to understand the country from afar, and a fascinating read for anyone interested in the Timorese world. ‘Researchers and policymakers reading up on Timor Leste before heading to the field will find this handbook valuable. It is littered with captivating fieldwork stories. The heart-searching is at times searingly honest. Best of all, the book beautifully bridges the sometimes painful gap between Timorese researchers and foreign experts (who can be irritating know-alls). Academic anthropologists and historians will find much of value here, but the Timor policy community should appreciate it as well.’ – Gerry van Klinken, KITLV ‘This book is well worth reading by academics, activists and policy-makers in Timor-Leste and also those interested in the country’s development.