Inclusion of Challenged Persons in Rural Setting
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
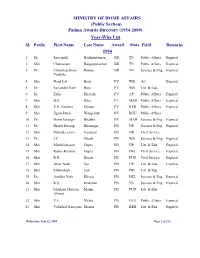
(Public Section) Padma Awards Directory (1954-2009) Year-Wise List Sl
MINISTRY OF HOME AFFAIRS (Public Section) Padma Awards Directory (1954-2009) Year-Wise List Sl. Prefix First Name Last Name Award State Field Remarks 1954 1 Dr. Sarvapalli Radhakrishnan BR TN Public Affairs Expired 2 Shri Chakravarti Rajagopalachari BR TN Public Affairs Expired 3 Dr. Chandrasekhara Raman BR TN Science & Eng. Expired Venkata 4 Shri Nand Lal Bose PV WB Art Expired 5 Dr. Satyendra Nath Bose PV WB Litt. & Edu. 6 Dr. Zakir Hussain PV AP Public Affairs Expired 7 Shri B.G. Kher PV MAH Public Affairs Expired 8 Shri V.K. Krishna Menon PV KER Public Affairs Expired 9 Shri Jigme Dorji Wangchuk PV BHU Public Affairs 10 Dr. Homi Jehangir Bhabha PB MAH Science & Eng. Expired 11 Dr. Shanti Swarup Bhatnagar PB UP Science & Eng. Expired 12 Shri Mahadeva Iyer Ganapati PB OR Civil Service 13 Dr. J.C. Ghosh PB WB Science & Eng. Expired 14 Shri Maithilisharan Gupta PB UP Litt. & Edu. Expired 15 Shri Radha Krishan Gupta PB DEL Civil Service Expired 16 Shri R.R. Handa PB PUN Civil Service Expired 17 Shri Amar Nath Jha PB UP Litt. & Edu. Expired 18 Shri Malihabadi Josh PB DEL Litt. & Edu. 19 Dr. Ajudhia Nath Khosla PB DEL Science & Eng. Expired 20 Shri K.S. Krishnan PB TN Science & Eng. Expired 21 Shri Moulana Hussain Madni PB PUN Litt. & Edu. Ahmed 22 Shri V.L. Mehta PB GUJ Public Affairs Expired 23 Shri Vallathol Narayana Menon PB KER Litt. & Edu. Expired Wednesday, July 22, 2009 Page 1 of 133 Sl. Prefix First Name Last Name Award State Field Remarks 24 Dr. -

Annual Report 2011-2012
Annual Report IND I A INTERNAT I ONAL CENTRE 2011-2012 IND I A INTERNAT I ONAL CENTRE New Delhi Board of Trustees Mr. Soli J. Sorabjee, President Justice (Retd.) Shri B.N. Srikrishna (w. e. f. 1st January, 2012) Mr. Suresh Kumar Neotia Professor M.G.K. Menon Mr. Rajiv Mehrishi Dr. (Mrs.) Kapila Vatsyayan Dr. Kavita A. Sharma, Director Mr. N. N. Vohra Executive Members Dr. Kavita A. Sharma, Director Mr. Kisan Mehta Mr. Najeeb Jung Dr. (Ms.) Sukrita Paul Kumar Dr. U.D. Choubey Cmde. (Retd.) Ravinder Datta, Secretary Lt. Gen. V.R. Raghavan Mr. P.R. Sivasubramanian, Hony. Treasurer Mrs. Meera Bhatia Finance Committee Justice (Retd.) Mr. B.N. Srikrishna, Dr. Kavita A. Sharma, Director Chairman Mr. P.R. Sivasubramanian, Hony. Treasurer Mr. M. Damodaran Cmde. (Retd.) Ravinder Datta, Secretary Lt. Gen. (Retd.) V.R. Raghavan Mr. Jnan Prakash, Chief Finance Officer Medical Consultants Dr. K.P. Mathur Dr. Rita Mohan Dr. K.A. Ramachandran Dr. B. Chakravorty Dr. Mohammad Qasim IIC Senior Staff Ms. Premola Ghose, Chief Programme Division Mr. Vijay Kumar Thukral, Executive Chef Mr. Arun Potdar, Chief Maintenance Division Mr. A.L. Rawal, Dy. General Manager (Catering) Ms. Omita Goyal, Chief Editor Mr. Inder Butalia, Sr. Finance and Accounts Officer Dr. S. Majumdar, Chief Librarian Ms. Madhu Gupta, Dy. General Manager (Hostel/House Keeping) Mr. Amod K. Dalela, Administration Officer Ms. Seema Kohli, Membership Officer (w. e. f. August 2011) Annual Report 2011-2012 As always, it is a privilege to present the 51th Annual Report of the India International Centre for the year commencing 1 February 2011 and ending 31 January 2012. -

Corporate Citizenship Report India 2016-17
Citizens of Progress MESSAGE FROM • MILESTONES • MELJOL THE CEO • CITI VALUES • NAVYA DISHA • PUBLIC CONCERN FOR GOVERNANCE TRUST 2 • SAMPARK FOUNDATION • SEVA SADAN SOCIETY • SWADHAAR FINACCESS • ADAPT YOUTH SKILLING • WWF INDIA & EMPLOYABILITY • ANUDIP FOUNDATION FOR SOCIAL WELFARE • CHILDFUND INDIA 6 • FOUNDATION OF MSME CLUSTERS ART & • INDIA FOUNDATION FOR THE ARTS • GENERATION INDIA FOUNDATION CULTURE • CHHATRAPATI SHIVAJI MAHARAJ VASTU • LEARNING LINKS FOUNDATION SANGHRAHALAYA • MEDHA 36 • NATIONAL CENTER FOR THE PERFORMING ARTS • PRATHAM EDUCATION FOUNDATION • SAMARTHANAM TRUST FOR THE DISABLED HEALTHCARE • AKSHAYA PATRA FOUNDATION • TECHNOSERVE INC. • THE INDIAN HEAD INJURY FOUNDATION • UDYOGINI 42 • JALDHAARA FOUNDATION • JANAAGRAHA CENTER FOR CITIZENSHIP AND DEMOCRACY EDUCATION • AMERICAN INDIA FOUNDATION TRUST • ST. JUDE INDIA CHILDCARE CENTERS & FINANCIAL • ASHOKA UNIVERSITY INCLUSION • BROOKINGS INSTITUTION INDIA CENTER • CITI JOURNALISTIC EXCELLENCE AWARD PROGRESS & ENABLERS OF 18 • CITI WOMAN LEADER AWARD SUSTAINABILITY PROGRESS • GRAMEEN FOUNDATION • HUMANA PEOPLE TO PEOPLE INDIA 48 54 • HUMANITY WELFARE ORGANIZATION • INCREASING DIVERSITY BY INCREASING ACCESS TO LEGAL EDUCATION INSPIRING CITI • KALIGHAT SOCIETY FOR DEVELOPMENT PROGRESS VALUES FACILITATION 52 58 MESSAGE FROM THE CEO ` 551 million TOTAL INVESTMENT TOWARDS CITIZENSHIP INITIATIVES IN INDIA IMPACTING APPROXIMATELY 1.47 MILLION INDIVIDUALS At Citi, it is our mission to enable economic progress and happened by deepening our relationships with existing growth for our clients and for society. This mission is partners and by bringing new partners into our family. In I am very pleased to present our 2016-17 Corporate Citizenship accompanied by a strong conviction that it is imperative for 2016–17, Citi invested ` 551 million in citizenship initiatives in Report – Citizens of Progress. We believe that it is incumbent this growth to be responsible and inclusive. -

Professional & Non-Fiction
Professional & 2017-2018 Non-fiction Also available as ebook seec www.sagepub.in Seconds with Linda Conway Correll Georgee Table of Contents and Arpan Yagnik SAGE RESPONSE Bestsellers ...............................23 Q. What is Creative Aerobics (CA)? How does of alternating left-brain and right-brain CA differ from traditional processes? exercises. Also, Creative Aerobics can be Branding & Advertising ......16-18 learned non-confrontationally in a relaxed A. Creative Aerobics (CA) is an evolutionary Business Ethics .........................7 and enjoyable environment. To shape one’s four-step ideation system that is unlike creativity to perfection, master the Creative traditional brainstorming methodology. To Business Research ....................5 Aerobics 1 to 4 from the book and thereon, begin with, it concentrates on process rather like everything else, it requires practice, Corporate Governance ..............7 than end result—producing fresh, previously practice and practice! unexplored and arrived-at creative solutions Entrepreneurship .....................14 to assignments. Secondly, at each step of the Q. We often get to hear about “Big Ideas”. way, it employs self-generated data-bases Human Resource What is your book’s take on this? that reflect the sui generis individualism of Management ....................... 8-10 the problem-solver, instead of cookie-cutter A. Starting small is the best way. Reach the creativity. depth to which your creativity can descend International Business .............14 and the breadth of attention-grabbing ideas Q. Is CA applicable only for professionals in it can summon. In my experience, Big Ideas Leadership ......................... 11-13 creative fields? start out as the fresh, small, out-of-the-box Legends in Consumer thoughts that Creative Aerobics generates. -

A Resource Book on Disability Studies in India
A RESOURCE BOOK ON DISABILITY STUDIES IN INDIA Compiled by NILIKA MEHROTRA With assistance from Pooja Singh and Priyanka Saini Centre for the Study of Social Systems, School of Social Sciences, Jawaharlal Nehru University, New Delhi, August 2016 i Preface The idea of a resource book emerged from the ongoing discourses, seminars, conferences and workshops around the topic and theme of disability studies. The conference that I had organized on Disability Studies in 2015 is what finally gave it the much needed momentum and it has taken the shape of what it is today. This piece of work was also made possible due to the funding and support of organizations like CSSS, GSP and ICSSR. It is hoped that the resource book will be a valuable tool to students, researchers and academicians alike. Given the vast arenas of knowledge present, and the number of organizations and institutions working towards the growth of disability studies and its allied causes, it was felt that there was an absence of all these sources at one place. The resource book should help fill this vacuum, as well as act as a catalyst for further research and disability research. An e-copy of this resource book will also be available at: http://www.jnu.ac.in/FacultyStaff/ShowProfile.asp?SendUserName=nilika ii CONTENTS 1) Disability Studies Programmes in India 2) NGOs and DPOs dealing with Disability in India Disability Networks on the Web Disability Groups 3) Bollywood Movies and Documentaries catering to the subject of Disability 4) Bibliography Disability, Gender and Sexuality -

E-Vidya (Sage)
E-Vidya (Sage) S.no Author name Title Subtitle Pub Year Subject1 Subject2 ePub ISBN / Web ISBN 1 Tattwamasi Caring for the Social 2015 Aging & Development 9789351505365 Paltasingh Elderly Gerontology in Gerontology Studies the Indian Context 2 Esta de Fossard Using Edu- 2008 International & 9788132100119 Tainment for Development Distance Communication Education in Community Work 3 Nalini Rajan 21st Century 2007 Journalism 9788132101185 Journalism in India 4 Bernard Bel Media and Volume I 2005 Media Policy 9788132102694 Mediation 5 Vinod Pavarala Other Voices The Struggle for 2007 Mass Political 9788132101581 Community Radio Communication Communication in India 6 Esta de Fossard Writing and 2005 International & 9788132102625 Producing for Development Television and Communication Film 7 V. K. Cherian India’s Film The Journey and 2016 Communication & Cultural Studies 9789385985621 Society its Impact Media Studies Movement 8 Swarnavel Madras Studios Narrative, Genre, 2014 Communication & Mass 9789351502128 Eswaran Pillai and Ideology in Media Studies Communication Tamil Cinema E-Vidya (Sage) 9 Srinivas R Melkote Communication Theory and 2001 Development 9788132119975 for Development Practice for Studies in the Third World Empowerment 10 Raminder Kaur Bollyworld Popular Indian 2005 Film & Cinema 9789352803446 Cinema Through A Transnational Lens 11 Nalini Rajan Practising Values, 2005 Journalism 9789352800674 Journalism Constraints, Implications 12 Amos Owen Imagi-Nations and Media, Culture 2005 Media Media Policy 9789352803378 Thomas Borderless -

INDIAN EPILEPSY ASSOCIATION 40 Years of Journey
A Saga of INDIAN EPILEPSY ASSOCIATION 40 Years of Journey Editor Dr HV Srinivas Consultant Neurologist Sagar Hospital & Agadi Hospital Bangalore INDIAN EPILEPSY ASSOCIATION A Saga of INDIAN EPILEPSY ASSOCIATION 40 Years of Journey A book of historical interest published on completion of 40 years of Indian Epilepsy Association and released during ECON 2013 at Hyderabad in February 2013 Copyright © 2013 by the Indian Epilepsy Association All rights reserved Cover design by D Drive Studio Bangalore Printed by: Aditi Enterprises #18/5, 22nd Cross, Bhuvaneshwari Nagar, Magadi Road, Bangalore - 23 Email: [email protected] CONTENTS Page Preface ..........................................................................................v Foreword ......................................................................................ix Founder Office Bearers .................................................................xi Governing Council (2011–2013) ................................................xii Presidents ..................................................................................xiv History of Indian Epilepsy Association ........................................ xv Presidents of Indian Epilepsy Association Dr Baldev Singh ..................................................................1 Dr TK Ghosh .......................................................................6 Dr KS Mani .......................................................................17 Dr B Ramamurthi ..............................................................22 -

(1954-2014) Year-Wise List 1954
MINISTRY OF HOME AFFAIRS (Public Section) Padma Awards Directory (1954-2014) Year-Wise List Sl. Prefix First Name Last Name Award State Field 1954 1 Dr. Sarvapalli Radhakrishnan BR TN Public Affairs 2 Shri Chakravarti Rajagopalachari BR TN Public Affairs 3 Shri Chandrasekhara Raman BR TN Science & Venkata 4 Dr. Satyendra Nath Bose PV WB Litt. & Edu. 5 Shri Nandlal Bose PV WB Art 6 Dr. Zakir Husain PV AP Public Affairs 7 Shri Bal Gangadhar Kher PV MAH Public Affairs 8 Shri V.K. Krishna Menon PV KER Public Affairs 9 Shri Jigme Dorji Wangchuk PV BHU Public Affairs 10 Dr. Homi Jehangir Bhabha PB MAH Science & 11 Dr. Shanti Swarup Bhatnagar PB UP Science & 12 Shri Mahadeva Iyer Ganapati PB OR Civil Service 13 Dr. Jnan Chandra Ghosh PB WB Science & 14 Shri Radha Krishna Gupta PB DEL Civil Service 15 Shri Maithilisharan Gupta PB UP Litt. & Edu. 16 Shri R.R. Handa PB PUN Civil Service 17 Shri Amarnath Jha PB UP Litt. & Edu. 21 May 2014 Page 1 of 193 Sl. Prefix First Name Last Name Award State Field 18 Shri Ajudhia Nath Khosla PB DEL Science & 19 Dr. K.S. Krishnan PB TN Science & 20 Shri Moulana Hussain Madni PB PUN Litt. & Edu. Ahmad 21 Shri Josh Malihabadi PB DEL Litt. & Edu. 22 Shri V.L. Mehta PB GUJ Public Affairs 23 Shri Vallathol Narayan Menon PB KER Litt. & Edu. 24 Dr. Arcot Mudaliar PB TN Litt. & Edu. Lakshamanaswami 25 Lt. (Col) Maharaj Kr. Palden T Namgyal PB PUN Public Affairs 26 Shri V. Narahari Raooo PB KAR Civil Service 27 Shri Pandyala Rau PB AP Civil Service Satyanarayana 28 Shri Jamini Roy PB WB Art 29 Shri Sukumar Sen PB WB Civil Service 30 Shri Satya Narayana Shastri PB UP Medicine 31 Late Smt. -
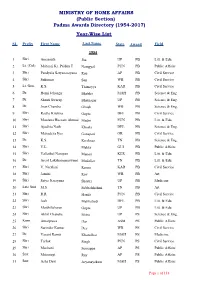
(Public Section) Padma Awards Directory (1954-2017) Year-Wise List
MINISTRY OF HOME AFFAIRS (Public Section) Padma Awards Directory (1954-2017) Year-Wise List SL Prefix First Name Last Name State Award Field 1954 1 Shri Amarnath Jha UP PB Litt. & Edu. 2 Lt. (Col) Maharaj Kr. Palden T Namgyal PUN PB Public Affairs 3 Shri Pandyala Satyanarayana Rau AP PB Civil Service 4 Shri Sukumar Sen WB PB Civil Service 5 Lt. Gen. K.S. Thimayya KAR PB Civil Service 6 Dr. Homi Jehangir Bhabha MAH PB Science & Eng. 7 Dr. Shanti Swarup Bhatnagar UP PB Science & Eng. 8 Dr. Jnan Chandra Ghosh WB PB Science & Eng. 9 Shri Radha Krishna Gupta DEL PB Civil Service 10 Shri Moulana Hussain Ahmad Madni PUN PB Litt. & Edu. 11 Shri Ajudhia Nath Khosla DEL PB Science & Eng. 12 Shri Mahadeva Iyer Ganapati OR PB Civil Service 13 Dr. K.S. Krishnan TN PB Science & Eng. 14 Shri V.L. Mehta GUJ PB Public Affairs 15 Shri Vallathol Narayan Menon KER PB Litt. & Edu. 16 Dr. Arcot Lakshamanaswami Mudaliar TN PB Litt. & Edu. 17 Shri V. Narahari Raooo KAR PB Civil Service 18 Shri Jamini Roy WB PB Art 19 Shri Satya Narayana Shastri UP PB Medicine 20 Late Smt. M.S. Subbalakshmi TN PB Art 21 Shri R.R. Handa PUN PB Civil Service 22 Shri Josh Malihabadi DEL PB Litt. & Edu. 23 Shri Maithilisharan Gupta UP PB Litt. & Edu. 24 Shri Akhil Chandra Mitra UP PS Science & Eng. 25 Kum. Amalprava Das ASM PS Public Affairs 26 Shri Surinder Kumar Dey WB PS Civil Service 27 Dr. Vasant Ramji Khanolkar MAH PS Medicine 28 Shri Tarlok Singh PUN PS Civil Service 29 Shri Machani Somappa AP PS Public Affairs 30 Smt. -

Spreading Smiles Sustaining Happiness
spreading smiles sustaining happiness Sustainability Report 2012 Aligned to GRI G 3.1 About this Report Coca-Cola India Private Limited (CCIPL hereinafter) is pleased to present its second sustainability report. While we started publishing communications on our sustainability performance in India recently, the concept of sustainability is not new to us. The Coca-Cola Company (TCCC - our parent company), which operates in over 200 countries, has identified facets of sustainability that are important to us based on the nature of our global operations and what our stakeholders expect of us. This has resulted in the ‘Me-We-World’ framework for sustainability that applies to all the group companies across the world. This multi-pronged framework covers material sustainability issues that enhance personal well being, build strong communities and help protect the environment. This sustainability report is arranged around the Me-We-World framework, and highlights key issues, relevant targets, and our performance in the reporting period (1st January 2012 to 31st December 2012). This report has been prepared based on the Global Reporting Initiative (GRI) G3.1 guidelines, including the Food Processing Sector Supplement (FPSS). This report takes into account all the reporting principles defined by the GRI to present a balanced and transparent communication and satisfies the requirements of GRI application level ‘B’. CCIPL is involved in the business of manufacturing and selling beverage concentrates and marketing products under the Coca-Cola trademark in India. Hindustan Coca-Cola Beverages Private Limited (HCCBPL), a wholly owned subsidiary of TCCC, is our largest bottling partner in India. There are other authorized third party (franchisee) bottlers, who manufacture and distribute our products in their respective geographical sub-divisions in India. -
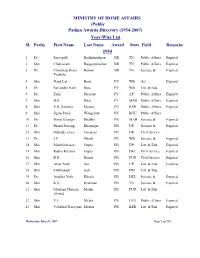
Padma Awards Directory (1954-2007) Year-Wise List
MINISTRY OF HOME AFFAIRS (Public Padma Awards Directory (1954-2007) Year-Wise List Sl. Prefix First Name Last Name Award State Field Remarks 1954 1 Dr. Sarvapalli Radhakrishnan BR TN Public Affairs Expired 2 Shri Chakravarti Rajagopalachari BR TN Public Affairs Expired 3 Dr. Chandrasekhara Raman BR TN Science & Expired Venkata 4 Shri Nand Lal Bose PV WB Art Expired 5 Dr. Satyendra Nath Bose PV WB Litt. & Edu. 6 Dr. Zakir Hussain PV AP Public Affairs Expired 7 Shri B.G. Kher PV MAH Public Affairs Expired 8 Shri V.K. Krishna Menon PV KER Public Affairs Expired 9 Shri Jigme Dorji Wangchuk PV BHU Public Affairs 10 Dr. Homi Jehangir Bhabha PB MAH Science & Expired 11 Dr. Shanti Swarup Bhatnagar PB UP Science & Expired 12 Shri Mahadeva Iyer Ganapati PB OR Civil Service 13 Dr. J.C. Ghosh PB WB Science & Expired 14 Shri Maithilisharan Gupta PB UP Litt. & Edu. Expired 15 Shri Radha Krishan Gupta PB DEL Civil Service Expired 16 Shri R.R. Handa PB PUN Civil Service Expired 17 Shri Amar Nath Jha PB UP Litt. & Edu. Expired 18 Shri Malihabadi Josh PB DEL Litt. & Edu. 19 Dr. Ajudhia Nath Khosla PB DEL Science & Expired 20 Shri K.S. Krishnan PB TN Science & Expired 21 Shri Moulana Hussain Madni PB PUN Litt. & Edu. Ahmed 22 Shri V.L. Mehta PB GUJ Public Affairs Expired 23 Shri Vallathol Narayana Menon PB KER Litt. & Edu. Expired Wednesday, May 30, 2007 Page 1 of 124 Sl. Prefix First Name Last Name Award State Field Remarks 24 Dr. Arcot Mudaliar PB TN Litt. -

New and Bestselling Titles
New and Bestselling Health & titles Social Work 2016-2017 www.sagepub.in Health & Social Work | 2016-17 8 March 2015 The Dirty picture This is one of the first books of Furthermore, the essays bring latter chapters. From sanitation the year that deal with the tricky out the role (or lack thereof) of at the watershed level and how it and highly important subject of women in water management. empowers women, these chapters page 5A water and sanitation — and a The focus is on self-help groups describe various facets of the link welcome addition to the body of (SHGs) and the authors argue that between sanitation and women. work available to practitioners. It women in villages with watershed A more academic treatise in covers broad concepts — water programmes have six times the the chapter called ‘Women-led and sanitation and their Total Sanitation’ underlines relationship with women. A new compendium on the greater benefits women In fact, the final section of derive from sanitation than the book features papers women’s relationship with men. It argues for making the presented at the National water and sanitation exposes community-led total sanitation Conference on Women- approach women-led in the led Water Management in a series of harsh realities State of Madhya Pradesh. An November 2012. innovation in sanitation called Pan in the Van has been used The initial chapters cover for training and promoting the overall water, sanitation and savings of villages without these inclusive WASH. hygiene (WASH) ‘sector’ and the programmes. Other chapters interplay with women’s issues.