Medical Product Quality Report – COVID‐19 Issues Issue 2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Chemical Disinfectants for Biohazardous Materials (3/21)
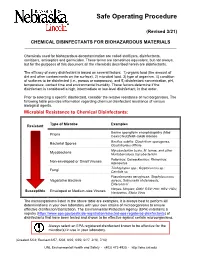
Safe Operating Procedure (Revised 3/21) CHEMICAL DISINFECTANTS FOR BIOHAZARDOUS MATERIALS ____________________________________________________________________________ Chemicals used for biohazardous decontamination are called sterilizers, disinfectants, sanitizers, antiseptics and germicides. These terms are sometimes equivalent, but not always, but for the purposes of this document all the chemicals described herein are disinfectants. The efficacy of every disinfectant is based on several factors: 1) organic load (the amount of dirt and other contaminants on the surface), 2) microbial load, 3) type of organism, 4) condition of surfaces to be disinfected (i.e., porous or nonporous), and 5) disinfectant concentration, pH, temperature, contact time and environmental humidity. These factors determine if the disinfectant is considered a high, intermediate or low-level disinfectant, in that order. Prior to selecting a specific disinfectant, consider the relative resistance of microorganisms. The following table provides information regarding chemical disinfectant resistance of various biological agents. Microbial Resistance to Chemical Disinfectants: Type of Microbe Examples Resistant Bovine spongiform encephalopathy (Mad Prions Cow) Creutzfeldt-Jakob disease Bacillus subtilis; Clostridium sporogenes, Bacterial Spores Clostridioides difficile Mycobacterium bovis, M. terrae, and other Mycobacteria Nontuberculous mycobacterium Poliovirus; Coxsackievirus; Rhinovirus; Non-enveloped or Small Viruses Adenovirus Trichophyton spp.; Cryptococcus sp.; -

Stanford Chem-H Presentation (PDF)
KiNativ® In situ kinase profiling Stanford University ChEM-H confidential @KiNativPlatform Principle of the KiNativ platform • ATP (or ADP) acyl phosphate binds to, and covalently modifies Lysine residues in the active site • Thus, ATP acyl phosphate with a desthiobiotin tag can be used capture and quantitate kinases in a complex lysate Acyl phosphate Desthiobiotin tag ATP 2 ATP acyl phosphate probe covalently modifies kinase in the active site Lysine 2 Lysine 1 3 ATP acyl phosphate probe covalently modifies kinase in the active site Lysine 2 Lysine 1 4 Samples trypsinized, probe-labeled peptides captured with streptavidin, and analyzed by targeted LC-MS2 Identification Quantitation Explicit determination of peptide Integration of signal from MS2 sequence and probe modification site fragment ions from MS2 spectrum 5 Comprehensive Coverage of Protein and Lipid Kinases Protein kinases Atypical kinases Green: Kinases detected on KiNativ Red: Kinases not detected on KiNativ ~80% of known protein and atypical kinases identified on the platform http://www.kinativ.com/coverage/protein-lipid.html 6 Profiling compound(s) on the KiNativ platform Control sample – add probe Sample: Lysate derived from any cell line or tissue from ANY species Treated sample – add inhibitor followed by probe Inhibited kinase Green: Kinases Blue: Probe Gray: Non-kinases Red: Inhibitor 7 Profiling compound(s) on the KiNativ platform Control sample – add probe MS signalMS Sample: Lysate derived from any cell line or tissue from ANY species Treated sample – add inhibitor -
Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination
Assessment of iodine deficiency disorders and monitoring their elimination A GUIDE FOR PROGRAMME MANAGERS Third edition Assessment of iodine deficiency disorders and monitoring their elimination A GUIDE FOR PROGRAMME MANAGERS Third edition WHO Library Cataloguing-in-Publication Data Assessment of iodine deficiency disorders and monitoring their elimination : a guide for programme managers. – 3rd ed. 1.Iodine – deficiency. 2.Nutrition disorders – prevention and control. 3.Sodium chloride, Dietary – therapeutic use. 4.Nutrition assessment. 5.Nutrition policy – standards. 6.Guidelines. I.World Health Organization. ISBN 978 92 4 159582 7 (NLM classification: WK 250) This report contains the collective views of an international group of experts, and does not necessarily represent the decisions or the stated policy of the World Health Organization. © World Health Organization 2007 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncom- mercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organi- zation concerning the legal status of any country, territory, city or area or of its authori- ties, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. -

Decontamination of Rooms, Medical Equipment and Ambulances Using an Aerosol of Hydrogen Peroxide Disinfectant B.M
Journal of Hospital Infection (2006) 62, 149–155 www.elsevierhealth.com/journals/jhin Decontamination of rooms, medical equipment and ambulances using an aerosol of hydrogen peroxide disinfectant B.M. Andersena,*, M. Rascha, K. Hochlina, F.-H. Jensenb, P. Wismarc, J.-E. Fredriksend aDepartment of Hospital Infection, Ulleva˚l University Hospital, Oslo, Norway bDivision of Pre-hospital Care, Ulleva˚l University Hospital, Oslo, Norway cDepartment of Medical Equipment, Ulleva˚l University Hospital, Oslo, Norway dHealth and Environment AS, Oslo, Norway Received 17 November 2004; accepted 1 July 2005 KEYWORDS Summary A programmable device (Sterinis, Gloster Sante Europe) Room decontamina- providing a dry fume of 5% hydrogen peroxide (H2O2) disinfectant was tion; Ambulance tested for decontamination of rooms, ambulances and different types of decontamination; medical equipment. Pre-set concentrations were used according to the Medical equipment decontamination; volumes of the rooms and garages. Three cycles were performed with Hydrogen peroxide increasing contact times. Repetitive experiments were performed using fume decontamina- Bacillus atrophaeus (formerly Bacillus subtilis) Raven 1162282 spores to tion; Spore test control the effect of decontamination; after a sampling plan, spore strips were placed in various positions in rooms, ambulances, and inside and outside the items of medical equipment. Decontamination was effective in 87% of 146 spore tests in closed test rooms and in 100% of 48 tests in a surgical department when using three cycles. One or two cycles had no effect. The sporicidal effect on internal parts of the medical equipment was only 62.3% (220 tests). When the devices were run and ventilated during decontamination, 100% (57/57) of spore strips placed inside were decontaminated. -
Evaluating Disinfectants for Use Against the COVID-19 Virus
When it comes to choosing a disinfectant to combat the COVID-19 virus, research and health authorities suggest not all disinfectants are equally effective. The difference is in their active ingredient(s). HEALTH CANADA AND U.S. EPA ASSESSMENTS The work to evaluate disinfectants perhaps best starts with lists of approved disinfectants compiled by government health authorities. Health Canada has compiled a list of 85 hard surface disinfectant products (as of March 20, 2020) that meet their requirements for disinfection of emerging pathogens, including the virus that causes COVID-19. It can be accessed here. You can wade through the entire list. But if you locate the Drug Identification Number (DIN) on the disinfectant product label or the safety data sheet (SDS), then you can use the search function to quickly see if the product meets Health Canada requirements. A second list, updated on March 19, 2020, provides 287 products that meet the U.S. Environmental Protection Agency’s (EPA) criteria for use against SARS-CoV-2, the novel coronavirus that causes the disease COVID-19. This list can be found here. Like the Health Canada list, you can wade through this one too. However, to best use this list, you should locate the U.S. EPA registration number on the product label or SDS, and use that number to search the list. The U.S. EPA registration number of a product consists of two sets of numbers separated by a hyphen. The first set of numbers refers to the company identification number, and the second set of numbers following the hyphen represents the product number. -

Download Product Insert (PDF)
PRODUCT INFORMATION Pacritinib Item No. 16709 CAS Registry No.: 937272-79-2 Formal Name: 11-[2-(1-pyrrolidinyl)ethoxy]-14,19-dioxa- 5,7,27-triazatetracyclo[19.3.1.12,6.18,12] O heptacosa-1(25),2,4,6(27),8,10,12(26), 16E,21,23-decaene Synonym: SB1518 N N H MF: C28H32N4O3 FW: 472.6 N Purity: ≥98% O Stability: ≥2 years at -20°C Supplied as: A crystalline solid N O UV/Vis.: λmax: 285 nm Laboratory Procedures For long term storage, we suggest that pacritinib be stored as supplied at -20°C. It should be stable for at least two years. Pacritinib is supplied as a crystalline solid. A stock solution may be made by dissolving the pacritinib in the solvent of choice. Pacritinib is soluble in the organic solvent DMSO, which should be purged with an inert gas, at a concentration of approximately 0.5 mg/ml (slightly warmed). Pacritinib is sparingly soluble in aqueous solutions. To enhance aqueous solubility, dilute the organic solvent solution into aqueous buffers or isotonic saline. If performing biological experiments, ensure the residual amount of organic solvent is insignificant, since organic solvents may have physiological effects at low concentrations. We do not recommend storing the aqueous solution for more than one day. Description FMS-like tyrosine kinase 3 (FLT3) and Janus kinase 2 (JAK2) are tyrosine kinases that mediate cytokine signaling and are frequently mutated in cancers, particularly acute myeloid leukemia.1,2 Pacritinib is an 1 inhibitor of both FLT3 and JAK2 (IC50s = 22 and 23 nM, respectively). -

Antimicrobial Activity of Cationic
ANTIMICROBIAL ACTIVITY OF CATIONIC ANTISEPTICS IN LAYER-BY-LAYER THIN FILM ASSEMBLIES A Thesis by CHARLENE MYRIAH DVORACEK Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE May 2009 Major Subject: Mechanical Engineering ANTIMICROBIAL ACTIVITY OF CATIONIC ANTISEPTICS IN LAYER-BY-LAYER THIN FILM ASSEMBLIES A Thesis by CHARLENE MYRIAH DVORACEK Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE Approved by: Chair of Committee, Jaime Grunlan Committee Members, Michael Benedik Xinghang Zhang Head of Department, Dennis O'Neal May 2009 Major Subject: Mechanical Engineering iii ABSTRACT Antimicrobial Activity of Cationic Antiseptics in Layer-by-Layer Thin Film Assemblies. (May 2009) Charlene Myriah Dvoracek, B.S., Rose-Hulman Institute of Technology Chair of Advisory Committee: Dr. Jaime Grunlan Layer-by-layer (LbL) assembly has proven to be a powerful technique for assembling thin films with a variety of properties including electrochromic, molecular sensing, oxygen barrier, and antimicrobial. LbL involves the deposition of alternating cationic and anionic ingredients from solution, utilizing the electrostatic charges to develop multilayer films. The present work incorporates cationic antimicrobial agents into the positively-charged layers of LbL assemblies. When these thin films are exposed to a humid environment, the antimicrobial molecules readily diffuse out and prevent bacterial growth. The influence of exposure time, testing temperature, secondary ingredients and number of bilayers on antimicrobial efficacy is evaluated here. Additionally, film growth and microstructure are analyzed to better understand the behavior of these films. -

Safer Disinfectant Use in Child Care and Schools During the COVID-19 Pandemic
Safer Disinfectant Use in Child Care and Schools During the COVID-19 Pandemic Vickie Leonard, PhD Environmental Health in Early Care and Educaon Project, Western States Pediatric Environmental Health Specialty Unit (WSPEHSU) 1 Why Should We Be Concerned about Environmental Health in ECE? 2 Why Should We Be Concerned about Environmental Health in ECE? • There are 8 million children in child care centers in the U.S. A child may spend up to 12,500 hours in an ECE facility. A million child care providers work in these centers in the U.S. Half are child-bearing age. • Many toxicants found in child care facilities are not addressed in state child care health and safety regulations. • No agency at the state or federal level is charged with ensuring children’s health and safety in and around schools and ECE facilities. • No systematic means exists for collecting data on environmental exposures in these buildings. • Teachers have more protection in these buildings (unions, OSHA) than children do 3 Why Should We Be Concerned about Environmental Health in ECE? • Many people think that adults and children are exposed to, and affected by, toxic chemicals in the same way. • This is not the case. • Children • have higher exposures to toxicants in the environment, • are more vulnerable to the effects of those toxicants than adults. 4 Cleaning and Disinfec?ng Products: A Major Source of Exposure in Child Care and Schools • Products used to clean, sanitize and disinfect child care facilities and schools are a good example of the pervasive and unregulated use of toxic chemicals that put the health of our children at risk. -

Reseptregisteret 2013–2017 the Norwegian Prescription Database
LEGEMIDDELSTATISTIKK 2018:2 Reseptregisteret 2013–2017 Tema: Legemidler og eldre The Norwegian Prescription Database 2013–2017 Topic: Drug use in the elderly Reseptregisteret 2013–2017 Tema: Legemidler og eldre The Norwegian Prescription Database 2013–2017 Topic: Drug use in the elderly Christian Berg Hege Salvesen Blix Olaug Fenne Kari Furu Vidar Hjellvik Kari Jansdotter Husabø Irene Litleskare Marit Rønning Solveig Sakshaug Randi Selmer Anne-Johanne Søgaard Sissel Torheim Utgitt av Folkehelseinstituttet/Published by Norwegian Institute of Public Health Område for Helsedata og digitalisering Avdeling for Legemiddelstatistikk Juni 2018 Tittel/Title: Legemiddelstatistikk 2018:2 Reseptregisteret 2013–2017 / The Norwegian Prescription Database 2013–2017 Forfattere/Authors: Christian Berg, redaktør/editor Hege Salvesen Blix Olaug Fenne Kari Furu Vidar Hjellvik Kari Jansdotter Husabø Irene Litleskare Marit Rønning Solveig Sakshaug Randi Selmer Anne-Johanne Søgaard Sissel Torheim Acknowledgement: Julie D. W. Johansen (English text) Bestilling/Order: Rapporten kan lastes ned som pdf på Folkehelseinstituttets nettsider: www.fhi.no The report can be downloaded from www.fhi.no Grafisk design omslag: Fete Typer Ombrekking: Houston911 Kontaktinformasjon/Contact information: Folkehelseinstituttet/Norwegian Institute of Public Health Postboks 222 Skøyen N-0213 Oslo Tel: +47 21 07 70 00 ISSN: 1890-9647 ISBN: 978-82-8082-926-9 Sitering/Citation: Berg, C (red), Reseptregisteret 2013–2017 [The Norwegian Prescription Database 2013–2017] Legemiddelstatistikk 2018:2, Oslo, Norge: Folkehelseinstituttet, 2018. Tidligere utgaver / Previous editions: 2008: Reseptregisteret 2004–2007 / The Norwegian Prescription Database 2004–2007 2009: Legemiddelstatistikk 2009:2: Reseptregisteret 2004–2008 / The Norwegian Prescription Database 2004–2008 2010: Legemiddelstatistikk 2010:2: Reseptregisteret 2005–2009. Tema: Vanedannende legemidler / The Norwegian Prescription Database 2005–2009. -

Being Aware of Chlorhexidine Allergy
Being aware of chlorhexidine allergy If you have an immediate allergic reaction to chlorhexidine you may experience symptoms such as: x itching x skin rash (hives) x swelling x anaphylaxis. People who develop anaphylaxis to chlorhexidine may have experienced mild reactions, such as skin rash, to chlorhexidine before. Irritant contact dermatitis or allergic contact dermatitis Chlorhexidine can also cause irritant dermatitis. This is not a true allergic reaction. It is caused by chlorhexidine directly irritating skin and results in rough, dry and scaly Chlorhexidine is an antiseptic. Allergic reactions to skin, sometimes with weeping sores. chlorhexidine are rare but are becoming more common. Chlorhexidine is used in many products both in Chlorhexidine can also cause allergic contact hospitals and in the community. dermatitis. Symptoms look like irritant dermatitis, but the cause of the symptoms is delayed by 12-48 hours Why have I been given this factsheet? after contact with chlorhexidine. You have been given this brochure because you have had a reaction to a medication, a medical dressing Both irritant dermatitis and allergic contact dermatitis or antiseptic. This may or may not be caused by a caused by chlorhexidine are annoying but not chlorhexidine allergy. dangerous. It is important that you are aware of the possibility of an It is recommended that you avoid chlorhexidine if you allergy. experience these responses as some people have gone on to develop immediate allergic reaction to chlorhexidine. Allergic reactions to chlorhexidine Severe allergic reactions to chlorhexidine are rare, but How do I know which products contain they can be serious. Immediate allergic reactions can chlorhexidine? cause anaphlaxis (a very severe allergic reaction which can be life-threatening). -

Tanibirumab (CUI C3490677) Add to Cart
5/17/2018 NCI Metathesaurus Contains Exact Match Begins With Name Code Property Relationship Source ALL Advanced Search NCIm Version: 201706 Version 2.8 (using LexEVS 6.5) Home | NCIt Hierarchy | Sources | Help Suggest changes to this concept Tanibirumab (CUI C3490677) Add to Cart Table of Contents Terms & Properties Synonym Details Relationships By Source Terms & Properties Concept Unique Identifier (CUI): C3490677 NCI Thesaurus Code: C102877 (see NCI Thesaurus info) Semantic Type: Immunologic Factor Semantic Type: Amino Acid, Peptide, or Protein Semantic Type: Pharmacologic Substance NCIt Definition: A fully human monoclonal antibody targeting the vascular endothelial growth factor receptor 2 (VEGFR2), with potential antiangiogenic activity. Upon administration, tanibirumab specifically binds to VEGFR2, thereby preventing the binding of its ligand VEGF. This may result in the inhibition of tumor angiogenesis and a decrease in tumor nutrient supply. VEGFR2 is a pro-angiogenic growth factor receptor tyrosine kinase expressed by endothelial cells, while VEGF is overexpressed in many tumors and is correlated to tumor progression. PDQ Definition: A fully human monoclonal antibody targeting the vascular endothelial growth factor receptor 2 (VEGFR2), with potential antiangiogenic activity. Upon administration, tanibirumab specifically binds to VEGFR2, thereby preventing the binding of its ligand VEGF. This may result in the inhibition of tumor angiogenesis and a decrease in tumor nutrient supply. VEGFR2 is a pro-angiogenic growth factor receptor -

Iodine Fact Sheet & References
Iodine Fact Sheet and References What is iodine? • Essential trace mineral • Critical in the synthesis of thyroid hormones. The thyroid gland converts iodine into T3 (triiodothyronine) and T4 (thyrodine) hormones, which control metabolism throughout the body. • Excreted through urine Where do we find iodine? • Table salt (iodized salt) – Beginning in the 1920s, iodine was added to table salt and to other foods to prevent iodine deficiency. • Seafood and seaweed • Dairy and grains (amounts vary depending on source) Who’s impacted? • 2.2 billion people worldwide are at risk for Iodine Deficiency Disorders (IDDs). Of these, 30-70% have goiter and 1-10% have cretinism. • People living in the Great Lakes region (including Minnesota) may have inadequate intake due to low levels of iodine in the soil in which crops are grown. • Iodine deficiency virtually eliminated in the U.S. and many Western nations, due to iodization of salt. However: o 1970s-1990s: median U.S. urinary iodine (UI) excretion fell 50%, indicating indicate intake, and possible increased risk for moderate IDD. Experts thought this might be attributable to a decreased intake of salt; removal of iodate conditioners in store-bought breads; and an increased use of non-iodized salt in manufactured or premade convenience foods o 2001-2002 NHANES data indicated that levels had stabilized. Even so, women of reproductive age consistently had the lowest UI levels. • Women of reproductive age are an important group to monitor: o Pregnant women are vulnerable to iodine deficiency due to an increased renal clearance of iodine and transfer of iodine to fetus. o Iodine supplementation during pregnancy is often delayed, because women are unaware they are pregnant during early weeks of gestation.