Molecular Pathogenesis of Peripheral Neuroblastic Tumors
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Downregulation of Nuclear and Cytoplasmic Chibby Is Associated with Advanced Cervical Cancer
6632 ONCOLOGY LETTERS 14: 6632-6644, 2017 Downregulation of nuclear and cytoplasmic Chibby is associated with advanced cervical cancer MING-CHANG YANG1,2*, SHANG-TAO CHIEN3,4*, TZU-FENG YANG2,5, SHIH-YI LIN3, TAI-MIN LEE3 and YI-REN HONG1,6,7 1 2 Department of Biological Sciences, National Sun Yat-sen University, Kaohsiung 80424; Laboratory of 3 Medical Research; Department of Pathology, Kaohsiung Armed Forces General Hospital, Kaohsiung 80284; 4Department of Medical Laboratory Sciences and Biotechnology, Fooyin University, Kaohsiung 83102; 5Department of Psychiatry, Kaohsiung Armed Forces General Hospital, Kaohsiung 80284; 6Department of Biochemistry, Faculty of Medicine, College of Medicine; 7Graduate Institute of Medicine, Kaohsiung Medical University, Kaohsiung 80708, Taiwan, R.O.C. Received March 11, 2014; Accepted June 9, 2017 DOI: 10.3892/ol.2017.7050 Abstract. Chibby has been identified as a putative tumor tumors, in which a significantly increased level of protein suppressor and antagonist to β-catenin, thereby controlling expression was detected. Chibby may be a tumor suppressor in the Wnt signaling pathway. Chibby is typically downregulated cervical cancer, since the dysregulation of Chibby expression is in numerous types of cancer and may be associated with associated with tumorigenesis in cervical cancer. Chibby and tumorigenesis. The present study aimed at clarifying the β-catenin expression together may potentially to a biomarker following: i) Whether Chibby antagonizes β-catenin in cervical for disease progression in cervical cancer. cancer; ii) whether Chibby and β-catenin mRNA expression is associated with cancer progression; and iii) whether Chibby Introduction and β-catenin expression may be used as a biomarker. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

Genome-Wide DNA Methylation Profiling Identifies Differential Methylation in Uninvolved Psoriatic Epidermis
Genome-Wide DNA Methylation Profiling Identifies Differential Methylation in Uninvolved Psoriatic Epidermis Deepti Verma, Anna-Karin Ekman, Cecilia Bivik Eding and Charlotta Enerbäck The self-archived postprint version of this journal article is available at Linköping University Institutional Repository (DiVA): http://urn.kb.se/resolve?urn=urn:nbn:se:liu:diva-147791 N.B.: When citing this work, cite the original publication. Verma, D., Ekman, A., Bivik Eding, C., Enerbäck, C., (2018), Genome-Wide DNA Methylation Profiling Identifies Differential Methylation in Uninvolved Psoriatic Epidermis, Journal of Investigative Dermatology, 138(5), 1088-1093. https://doi.org/10.1016/j.jid.2017.11.036 Original publication available at: https://doi.org/10.1016/j.jid.2017.11.036 Copyright: Elsevier http://www.elsevier.com/ Genome-Wide DNA Methylation Profiling Identifies Differential Methylation in Uninvolved Psoriatic Epidermis Deepti Verma*a, Anna-Karin Ekman*a, Cecilia Bivik Edinga and Charlotta Enerbäcka *Authors contributed equally aIngrid Asp Psoriasis Research Center, Department of Clinical and Experimental Medicine, Division of Dermatology, Linköping University, Linköping, Sweden Corresponding author: Charlotta Enerbäck Ingrid Asp Psoriasis Research Center, Department of Clinical and Experimental Medicine, Linköping University SE-581 85 Linköping, Sweden Phone: +46 10 103 7429 E-mail: [email protected] Short title Differential methylation in psoriasis Abbreviations CGI, CpG island; DMS, differentially methylated site; RRBS, reduced representation bisulphite sequencing Keywords (max 6) psoriasis, epidermis, methylation, Wnt, susceptibility, expression 1 ABSTRACT Psoriasis is a chronic inflammatory skin disease with both local and systemic components. Genome-wide approaches have identified more than 60 psoriasis-susceptibility loci, but genes are estimated to explain only one third of the heritability in psoriasis, suggesting additional, yet unidentified, sources of heritability. -

Cellular and Molecular Signatures in the Disease Tissue of Early
Cellular and Molecular Signatures in the Disease Tissue of Early Rheumatoid Arthritis Stratify Clinical Response to csDMARD-Therapy and Predict Radiographic Progression Frances Humby1,* Myles Lewis1,* Nandhini Ramamoorthi2, Jason Hackney3, Michael Barnes1, Michele Bombardieri1, Francesca Setiadi2, Stephen Kelly1, Fabiola Bene1, Maria di Cicco1, Sudeh Riahi1, Vidalba Rocher-Ros1, Nora Ng1, Ilias Lazorou1, Rebecca E. Hands1, Desiree van der Heijde4, Robert Landewé5, Annette van der Helm-van Mil4, Alberto Cauli6, Iain B. McInnes7, Christopher D. Buckley8, Ernest Choy9, Peter Taylor10, Michael J. Townsend2 & Costantino Pitzalis1 1Centre for Experimental Medicine and Rheumatology, William Harvey Research Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, Charterhouse Square, London EC1M 6BQ, UK. Departments of 2Biomarker Discovery OMNI, 3Bioinformatics and Computational Biology, Genentech Research and Early Development, South San Francisco, California 94080 USA 4Department of Rheumatology, Leiden University Medical Center, The Netherlands 5Department of Clinical Immunology & Rheumatology, Amsterdam Rheumatology & Immunology Center, Amsterdam, The Netherlands 6Rheumatology Unit, Department of Medical Sciences, Policlinico of the University of Cagliari, Cagliari, Italy 7Institute of Infection, Immunity and Inflammation, University of Glasgow, Glasgow G12 8TA, UK 8Rheumatology Research Group, Institute of Inflammation and Ageing (IIA), University of Birmingham, Birmingham B15 2WB, UK 9Institute of -

In a Neuroblastoma Patient Disrupts NBPF1, a Novel Putative Tumor
A Constitutional Translocation t(1;17)(p36.2;q11.2) in a Neuroblastoma Patient Disrupts NBPF1 , a novel putative tumor suppressor gene Vanessa Andries , Karl Vandepoele , Katrien Staes, and Frans van Roy Molecular Cell Biology Unit, Dept. for Molecular Biomedical Research, VIB/Ghent University, Technologiepark 927, B-9052 Ghent (Zwijnaarde) E-mail: [email protected], [email protected] Neuroblastoma (NB) is the most common extracranial solid tumor in children and is characterized by a number of recurrent genetic alterations: gain of chromosome 17q, amplification of MYCN , and deletion of 1p36. We found that a constitutional translocation t(1;17)(p36.2;q11.2) in a neuroblastoma patient (Laureys et al., 1995) resulted in the disruption of a novel gene, NBPF1 (Neuroblastoma Breakpoint Family, member 1). This gene is built of repetitive elements and is subject of structural variation in the human population. Thorough analysis of genomic sequences revealed that NBPF1 is a member of a recently expanded gene family, with gene copies located on segmental duplications of chromosome 1 (Vandepoele et al., 2005). Both in silico and in vitro analysis failed to identify any rodent orthologs for the human NBPF genes. The members of the NBPF gene family are widely expressed, both in normal and cancerous tissues, including neuroblastoma cells. Our identification of NBPF-interacting proteins may link these genes to important signalling pathways such as the Wnt and NF-kappaB signalling pathways. The high sequence identity between different NBPF paralogs has thus far disabled the analysis of gene-specific expression patterns, but the development of an NBPF1 -specific qRT-PCR assay is in progress. -

Analysis of the Indacaterol-Regulated Transcriptome in Human Airway
Supplemental material to this article can be found at: http://jpet.aspetjournals.org/content/suppl/2018/04/13/jpet.118.249292.DC1 1521-0103/366/1/220–236$35.00 https://doi.org/10.1124/jpet.118.249292 THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS J Pharmacol Exp Ther 366:220–236, July 2018 Copyright ª 2018 by The American Society for Pharmacology and Experimental Therapeutics Analysis of the Indacaterol-Regulated Transcriptome in Human Airway Epithelial Cells Implicates Gene Expression Changes in the s Adverse and Therapeutic Effects of b2-Adrenoceptor Agonists Dong Yan, Omar Hamed, Taruna Joshi,1 Mahmoud M. Mostafa, Kyla C. Jamieson, Radhika Joshi, Robert Newton, and Mark A. Giembycz Departments of Physiology and Pharmacology (D.Y., O.H., T.J., K.C.J., R.J., M.A.G.) and Cell Biology and Anatomy (M.M.M., R.N.), Snyder Institute for Chronic Diseases, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada Received March 22, 2018; accepted April 11, 2018 Downloaded from ABSTRACT The contribution of gene expression changes to the adverse and activity, and positive regulation of neutrophil chemotaxis. The therapeutic effects of b2-adrenoceptor agonists in asthma was general enriched GO term extracellular space was also associ- investigated using human airway epithelial cells as a therapeu- ated with indacaterol-induced genes, and many of those, in- tically relevant target. Operational model-fitting established that cluding CRISPLD2, DMBT1, GAS1, and SOCS3, have putative jpet.aspetjournals.org the long-acting b2-adrenoceptor agonists (LABA) indacaterol, anti-inflammatory, antibacterial, and/or antiviral activity. Numer- salmeterol, formoterol, and picumeterol were full agonists on ous indacaterol-regulated genes were also induced or repressed BEAS-2B cells transfected with a cAMP-response element in BEAS-2B cells and human primary bronchial epithelial cells by reporter but differed in efficacy (indacaterol $ formoterol . -

Progressive Modulation of the Human Olfactory Bulb
www.impactjournals.com/oncotarget/ Oncotarget, 2017, Vol. 8, (No. 41), pp: 69663-69679 Research Paper Progressive modulation of the human olfactory bulb transcriptome during Alzheimer´s disease evolution: novel insights into the olfactory signaling across proteinopathies Mercedes Lachen-Montes1,2, María Victoria Zelaya1,2,3, Víctor Segura2,4, Joaquín Fernández-Irigoyen1,2,5,* and Enrique Santamaría1,2,5,* 1Clinical Neuroproteomics Group, Navarrabiomed, Departamento de Salud, Universidad Pública de Navarra, Pamplona, Spain 2IDISNA, Navarra Institute for Health Research, Pamplona, Spain 3Pathological Anatomy Department, Navarra Hospital Complex, Pamplona, Spain 4Bioinformatics Unit, Center for Applied Medical Research, University of Navarra, Pamplona, Spain 5Proteored-ISCIII, Proteomics Unit, Navarrabiomed, Departamento de Salud, Universidad Pública de Navarra, Pamplona, Spain *These authors share senior authorship Correspondence to: Enrique Santamaría, email: [email protected] Keywords: Alzheimer, neurodegeneration, dementia, olfactory bulb, transcriptomics Received: January 21, 2017 Accepted: May 07, 2017 Published: May 23, 2017 Copyright: Lachen-Montes et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License 3.0 (CC BY 3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. ABSTRACT Alzheimer´s disease (AD) is characterized by progressive dementia, initially presenting olfactory dysfunction. Despite the olfactory bulb (OB) is the first central structure of the olfactory pathway, we lack a complete molecular characterization of the transcriptional events that occurs in this olfactory area during AD progression. To address this gap in knowledge, we have assessed the genome-wide expression in postmortem OBs from subjects with varying degree of AD pathology. -

Molecular Signatures Differentiate Immune States in Type 1 Diabetes Families
Page 1 of 65 Diabetes Molecular signatures differentiate immune states in Type 1 diabetes families Yi-Guang Chen1, Susanne M. Cabrera1, Shuang Jia1, Mary L. Kaldunski1, Joanna Kramer1, Sami Cheong2, Rhonda Geoffrey1, Mark F. Roethle1, Jeffrey E. Woodliff3, Carla J. Greenbaum4, Xujing Wang5, and Martin J. Hessner1 1The Max McGee National Research Center for Juvenile Diabetes, Children's Research Institute of Children's Hospital of Wisconsin, and Department of Pediatrics at the Medical College of Wisconsin Milwaukee, WI 53226, USA. 2The Department of Mathematical Sciences, University of Wisconsin-Milwaukee, Milwaukee, WI 53211, USA. 3Flow Cytometry & Cell Separation Facility, Bindley Bioscience Center, Purdue University, West Lafayette, IN 47907, USA. 4Diabetes Research Program, Benaroya Research Institute, Seattle, WA, 98101, USA. 5Systems Biology Center, the National Heart, Lung, and Blood Institute, the National Institutes of Health, Bethesda, MD 20824, USA. Corresponding author: Martin J. Hessner, Ph.D., The Department of Pediatrics, The Medical College of Wisconsin, Milwaukee, WI 53226, USA Tel: 011-1-414-955-4496; Fax: 011-1-414-955-6663; E-mail: [email protected]. Running title: Innate Inflammation in T1D Families Word count: 3999 Number of Tables: 1 Number of Figures: 7 1 For Peer Review Only Diabetes Publish Ahead of Print, published online April 23, 2014 Diabetes Page 2 of 65 ABSTRACT Mechanisms associated with Type 1 diabetes (T1D) development remain incompletely defined. Employing a sensitive array-based bioassay where patient plasma is used to induce transcriptional responses in healthy leukocytes, we previously reported disease-specific, partially IL-1 dependent, signatures associated with pre and recent onset (RO) T1D relative to unrelated healthy controls (uHC). -

The Driver of Extreme Human-Specific Olduvai Repeat Expansion Remains Highly Active in the Human
Genetics: Early Online, published on November 21, 2019 as 10.1534/genetics.119.302782 1 The Driver of Extreme Human-Specific Olduvai Repeat Expansion Remains Highly Active in the Human 2 Genome 3 Ilea E. Heft,1,* Yulia Mostovoy,2,* Michal Levy-Sakin,2 Walfred Ma,2 Aaron J. Stevens,3 Steven 4 Pastor,4 Jennifer McCaffrey,4 Dario Boffelli,5 David I. Martin,5 Ming Xiao,4 Martin A. Kennedy,3 5 Pui-Yan Kwok,2,6,7 and James M. Sikela1 6 7 1Department of Biochemistry and Molecular Genetics, and Human Medical Genetics and 8 Genomics Program, University of Colorado School of Medicine, Aurora CO 80045 9 2Cardiovascular Research Institute, 6Department of Dermatology, and 7Institute for Human 10 Genetics, University of California, San Francisco, San Francisco, CA, USA 11 3Department of Pathology, University of Otago, Christchurch, New Zealand 8140 12 4School of Biomedical Engineering, Drexel University, Philadelphia, PA 19104 13 5Children's Hospital Oakland Research Institute, Oakland, CA, 94609 14 15 Corresponding author: James M. Sikela: [email protected] 16 *Ilea E. Heft and Yulia Mostovoy contributed equally to this article. 17 1 Copyright 2019. 18 Abstract 19 Sequences encoding Olduvai protein domains (formerly DUF1220) show the greatest 20 human lineage-specific increase in copy number of any coding region in the genome and have 21 been associated, in a dosage-dependent manner, with brain size, cognitive aptitude, autism, 22 and schizophrenia. Tandem intragenic duplications of a three-domain block, termed the Olduvai 23 triplet, in four NBPF genes in the chromosomal 1q21.1-.2 region are primarily responsible for 24 the striking human-specific copy number increase. -
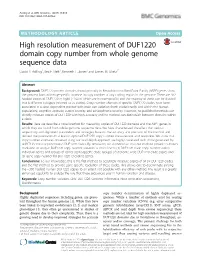
High Resolution Measurement of DUF1220 Domain Copy Number from Whole Genome Sequence Data David P
Astling et al. BMC Genomics (2017) 18:614 DOI 10.1186/s12864-017-3976-z METHODOLOGYARTICLE Open Access High resolution measurement of DUF1220 domain copy number from whole genome sequence data David P. Astling1, Ilea E. Heft1, Kenneth L. Jones2 and James M. Sikela1* Abstract Background: DUF1220 protein domains found primarily in Neuroblastoma BreakPoint Family (NBPF) genes show the greatest human lineage-specific increase in copy number of any coding region in the genome. There are 302 haploid copies of DUF1220 in hg38 (~160 of which are human-specific) and the majority of these can be divided into 6 different subtypes (referred to as clades). Copy number changes of specific DUF1220 clades have been associated in a dose-dependent manner with brain size variation (both evolutionarily and within the human population), cognitive aptitude, autism severity, and schizophrenia severity. However, no published methods can directly measure copies of DUF1220 with high accuracy and no method can distinguish between domains within a clade. Results: Here we describe a novel method for measuring copies of DUF1220 domains and the NBPF genes in which they are found from whole genome sequence data. We have characterized the effect that various sequencing and alignment parameters and strategies have on the accuracy and precision of the method and defined the parameters that lead to optimal DUF1220 copy number measurement and resolution. We show that copy number estimates obtained using our read depth approach are highly correlated with those generated by ddPCR for three representative DUF1220 clades. By simulation, we demonstrate that our method provides sufficient resolution to analyze DUF1220 copy number variation at three levels: (1) DUF1220 clade copy number within individual genes and groups of genes (gene-specific clade groups) (2) genome wide DUF1220 clade copies and (3) gene copy number for DUF1220-encoding genes. -
Exploring the Regulatory Mechanism of the Notch Ligand Receptor Jagged1 Via the Aryl Hydrocarbon Receptor in Breast Cancer Sean Alan Piwarski
Marshall University Marshall Digital Scholar Theses, Dissertations and Capstones 2018 Exploring the Regulatory Mechanism of the Notch Ligand Receptor Jagged1 Via the Aryl Hydrocarbon Receptor in Breast Cancer Sean Alan Piwarski Follow this and additional works at: https://mds.marshall.edu/etd Part of the Biological Phenomena, Cell Phenomena, and Immunity Commons, Medical Molecular Biology Commons, Medical Toxicology Commons, and the Oncology Commons EXPLORING THE REGULATORY MECHANISM OF THE NOTCH LIGAND RECEPTOR JAGGED1 VIA THE ARYL HYDROCARBON RECEPTOR IN BREAST CANCER A dissertation submitted to the Graduate College of Marshall University In partial fulfillment of the requirements for the degree of Doctor of Philosophy In Biomedical Sciences by Sean Alan Piwarski Approved by Dr. Travis Salisbury, Committee Chairperson Dr. Gary Rankin Dr. Monica Valentovic Dr. Richard Egleton Dr. Todd Green Marshall University July 2018 APPROVAL OF DISSERTATION We, the faculty supervising the work of Sean Alan Piwarski, affirm that the dissertation, Exploring the Regulatory Mechanism of the Notch Ligand Receptor JAGGED1 via the Aryl Hydrocarbon Receptor in Breast Cancer, meets the high academic standards for original scholarship and creative work established by the Biomedical Sciences program and the Graduate College of Marshall University. This work also conforms to the editorial standards of our discipline and the Graduate College of Marshall University. With our signatures, we approve the manuscript for publication. ii © 2018 SEAN ALAN PIWARSKI ALL RIGHTS RESERVED iii DEDICATION To my mom and dad, This dissertation is a product of your hard work and sacrifice as amazing parents. I could never have accomplished something of this magnitude without your love, support, and constant encouragement. -

The Somatic Mutation Landscape of Chinese Colorectal Cancer
Journal of Cancer 2020, Vol. 11 1038 Ivyspring International Publisher Journal of Cancer 2020; 11(5): 1038-1046. doi: 10.7150/jca.37017 Research Paper The somatic mutation landscape of Chinese Colorectal Cancer Rong Ma1#, Changwen Jing1#, Yuan Zhang1#, Haixia Cao1, Siwen Liu1, Zhuo Wang1, Dan Chen1, Junying Zhang1, Yang Wu1, Jianzhong Wu1 and Jifeng Feng2 1. Clinical Cancer Research Center, Jiangsu Cancer Hospital &Jiangsu Institute of Cancer Research &The Affiliated Cancer Hospital of Nanjing Medical University, China. 2. Department of Chemotherapy, Jiangsu Cancer Hospital &Jiangsu Institute of Cancer Research &The Affiliated Cancer Hospital of Nanjing Medical University, China. # These authors contributed equally to this work. Corresponding author: J.W. ([email protected]) or J. F. ([email protected]) © The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See http://ivyspring.com/terms for full terms and conditions. Received: 2019.05.26; Accepted: 2019.10.27; Published: 2020.01.01 Abstract Colorectal cancer (CRC) is the fifth leading cause of cancer-related death in China. The incidence of Chinese CRC has increased dramatically with the changes of dietary and lifestyle. However, the genetic landscape of Chinese colorectal cancer mutation is still poorly understood. In this study, we have performed whole exome-sequencing analysis of 63 CRC cases. We found that Chinese CRC were hypermutated, which were enriched in ECM-receptor interaction, antigen processing and presentation, and focal adhesion. Analysis with clinical characteristics indicated that the deficiency of CRC driver gene, FCGBP and NBPF1 conferred CRC development and was showed worse survival rates, which could be the novel regulators and, diagnostic and prognostic biomarkers for Chinese CRC.