Northern Ireland Barriers to Accessing Abortion Services
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The 2013 Irish Legislation on Abortion: Turning-Point Or Missed Opportunity?
NATIONAL UNIVERSITY OF IRELAND GALWAY European Master’s Degree in Human Rights and Democratisation A.Y. 2013/2014 The 2013 Irish legislation on abortion: turning-point or missed opportunity? A critical analysis from a human rights perspective Author: Chiara Cosentino Supervisor: Noelle Higgins Ackowledgements I would like to thank Noelle Higgins, from the NUI of Galway, for the supervision of the present work and for her precise and insightful comments and suggestions. Furthermore, I would like to deeply thank the contacted civil society organisations that kindly and enthusiastically agreed on allowing me to steal a bit of their time for interviews. They were fundamental for my analysis, for the perception from the ground they gave me, and for the global picture that I could capture from their different angles of perspective on the topic. In particular I would love to thank for their availability Richie Keane (Coordinator of Doctors For Choice), Sinéad Corcoran (member of the Policy and Advocacy Team of Abortion Right Campaign), Kelly Mackey (from the Campaign Office of Amnesty International Ireland), Maeve Taylor (Senior Policy and Advocacy Officer of the Irish Family Planning Association) and Dette McLoughlin, John Walshe and Joseph Loughnane (members of Galway Pro-Choice). I would also like to thank my family, my parents, my sister and my grandmother for their unconditional support, and for making my participation in this Master possible, both with their practical help and love. I missed them throughout this year, but we all know that, wherever I am, they are always in my heart. Moreover, I would like to thank all my friends, old and new, for what they mean and they will always mean to me. -

Submission to the Citizens' Assembly
Submission to the Citizens’ Assembly SUBMISSION TO THE CITIZENS’ ASSEMBLY TABLE OF CONTENTS The Abortion Rights Campaign 4 Introduction 5 Repealing the 8th Amendment 6 Why we should repeal the 8th 7 The reality of abortion in Ireland 9 The reality of the 8th Amendment in Ireland 12 International Condemnation 13 Free, Safe, Legal 15 Why we need free, safe, legal abortion access 16 Availability in the public health system 17 Abortion on request 18 Gestational limits 19 Decriminalisation 21 Conscientious objection 23 Conclusion 26 Let women choose 27 Abortion Stories 28 3 THE ABORTION RIGHTS CAMPAIGN The Abortion Rights Campaign (ARC) is a grassroots movement for choice and change in Ireland. We organise the annual March for Choice, which this year saw 20,000 people take to the streets of Dublin to demand a change to Ireland’s abortion laws. We aim to promote broad national support for a referendum to repeal the 8th Amendment and the introduction of free, safe and legal abortion access in the State. We believe women can be trusted to choose, and we aim to ensure the health and rights of women in Ireland are protected in line with international best practice and human rights standards. We welcome the opportunity to make a submission to the Citizens’ Assembly during its consideration of the 8th Amendment to the Constitution. 4 INTRODUCTION As the largest grassroots pro-choice organisation in Ireland, we represent those people directly affected by the 8th Amendment. We represent the 12 women each day who leave Irish shores to access standard medical care. -
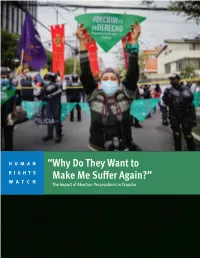
“Why Do They Want to Make Me Suffer Again?” the Impact of Abortion Prosecutions in Ecuador
HUMAN “Why Do They Want to RIGHTS WATCH Make Me Suffer Again?” The Impact of Abortion Prosecutions in Ecuador “Why Do They Want to Make Me Suffer Again?” The Impact of Abortion Prosecutions in Ecuador Copyright © 2021 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 978-1-62313-919-3 Cover design by Rafael Jimenez Human Rights Watch defends the rights of people worldwide. We scrupulously investigate abuses, expose the facts widely, and pressure those with power to respect rights and secure justice. Human Rights Watch is an independent, international organization that works as part of a vibrant movement to uphold human dignity and advance the cause of human rights for all. Human Rights Watch is an international organization with staff in more than 40 countries, and offices in Amsterdam, Beirut, Berlin, Brussels, Chicago, Geneva, Goma, Johannesburg, London, Los Angeles, Moscow, Nairobi, New York, Paris, San Francisco, Sydney, Tokyo, Toronto, Tunis, Washington DC, and Zurich. For more information, please visit our website: http://www.hrw.org JULY 2021 ISBN: 978-1-62313-919-3 “Why Do They Want to Make Me Suffer Again?” The Impact of Abortion Prosecutions in Ecuador Summary ........................................................................................................................... 1 Key Recommendations ....................................................................................................... 8 To the Presidency ................................................................................................................... -

The Pro-Choice Movement in Ireland Áine Ní Mhainnín
mhAinnín | Pro Choice 38 mhAinnín | Pro Choice The power of women’s voices: the pro-choice movement in Ireland ÁIne ní mhaInnín avita Halappanavar was 31 years old. Originally from India, she moved to the west of Ireland to be Swith her husband, Praveen. On 21st October 2012, she and Praveen arrived at University College Hospital Galway. Savita was 17 weeks pregnant and suffering from back pain. Told she was miscar- - fused each time, once given the reason that Ireland was a ‘Catholic country’. Finally, after Savita had spent 2 ½ days in agony, the foetal heartbeat stopped and the foetus was removed. Savita died on 28 October 2012. Her death was recorded as a result of severe sepsis, E. coli in the bloodstream and a miscarriage at 17 weeks. Having returned from Savita’s funeral in India, Praveen recounted her story to the Irish Times. It was woman to die through refusing her a termination, was receiving global attention. That evening, within only a few hours of the story being posted, several hundred attended a vigil outside the Dáil (Irish rallies did not occur in a bubble, but have been the focal point of a change of mood over the last year or so in relation to a woman’s right to choose. Ireland’s barbaric position came about through the suc- cess of anti-choice lobby groups in blurring the distinction between Church and State, resulting in a Background The 1861 Offences Against the Person Act prohibited the procurement of a miscarriage within the United Kingdom of Great Britain and Ireland. -
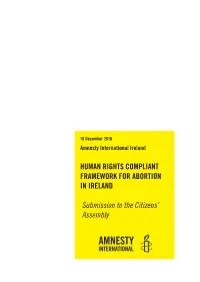
Human Rights Compliant Framework for Abortion in Ireland
16 December 2016 Amnesty International Ireland HUMAN RIGHTS COMPLIANT FRAMEWORK FOR ABORTION IN IRELAND Submission to the Citizens’ Assembly DEFINITIONS International human rights treaty: also sometimes called a Covenant or a Convention, is adopted by the international community of States, normally at the United Nations General Assembly. Each treaty sets out a range of human rights, and corresponding obligations which are legally binding on States that have ratified the treaty. Treaty monitoring body: each of the international human rights treaties is monitored by a designated treaty monitoring body. The treaty monitoring bodies are committees composed of independent experts. Their main function is to monitor the States’ compliance with the treaty in question, including through the examination of State reports. General comments/recommendations: a treaty monitoring body’s interpretation of the con- tent of human rights provisions on thematic issues or its methods of work. General com- ments seek to clarify the reporting duties of State parties with respect to certain provisions and suggest approaches to implementing treaty provisions. Concluding observations: following submission of a State report and a constructive di- alogue with the State party to the particular convention, treaty monitoring bodies issue concluding observations to the reporting State, which are compiled in an annual report and sent to the United Nations General Assembly. Human rights standards: the meaning and scope of human rights as interpreted and applied by the human rights bodies tasked with this work, e.g. international, regional and national courts, and human rights committees. Drawn from the World Health Organisation’s Safe abortion: technical and policy guidance for health systems, second edition (2012) Human Rights Compliant Framework for Abortion in Ireland - Submission to the Citizens’ Assembly CONTENTS DEFINITIONS............................................................................................................................ -

Heresa Morrow: RTÉ One TV: the Late Late Show: 8Th Jan 2016…………………………….81
Broadcasting Authority of Ireland Broadcasting Complaint Decisions September 2016 Broadcasting Complaint Decisions Contents BAI Complaints Handling Process Page 4 Upheld by the BAI Compliance Committee 26/16 - Mr. Francis Clauson: TV3: ‘The Power to Power Ourselves’ (Advert): 10th Jan 2016………………5 27/16 - Mr. Francis Clauson: RTÉ One TV: ‘The Power to Power Ourselves’ (Advert): 16th Jan 2016….…9 29/16 - Intro Matchmaking: Sunshine 106.8: Two’s Company (Advert):16th Feb 2016…………….………13 Rejected by the BAI Compliance Committee 7/16 - Mr. Brendan Burgess: RTÉ One TV: Ireland’s Great Wealth Divide: 21st Sept 2015……………….16 13/16 - Mr. Martin Hawkes: RTÉ One TV: Prime Time: 3rd Dec 2015……………………………………….23 15/16 - An Taisce: RTÉ One TV: Prime Time: 3rd Dec 2015………………………………………………….28 30/16 - Mr. Pawel Rydzewski: RTÉ One TV: The Late Late Show: 22nd Jan 2016…………………………38 32/16 - Mr Séamus Enright: TV3: TV3 Leaders’ Debate: 11th Feb 2016………………………………….…41 35/16 - Mr. John Flynn: RTÉ One TV: The Late Late Show: 19th Feb 2016…………………………………45 37/16 - Mr. Enda Fanning: RTÉ One TV: The Late Late Show: 19th Feb 2016……………………………48 Rejected by the Executive Complaints Forum 8-10/16 - Mr. Brendan O’ Regan: Newstalk: The Pat Kenny Show: 2nd – 4th Dec 2015……………………52 19/16 - Ms. Patricia Kearney: RTÉ Radio 1: When Dave Met Bob: 29th Dec 2015…………………………58 21/16 – Ms. Mary Jo Gilligan: RTÉ Radio 1: The Ray D’Arcy Show: 14th Nov 2015………………………61 22/16 - Mr. Brendan O’ Regan: Newstalk: Lunchtime: 30th Nov 2015…………………………………….…64 23/16 - Mr. Brendan O’ Regan: Newstalk: The Pat Kenny Show: 1st Dec 2015………………………….…64 25/16 - Mr. -

Cedaw/C/Op.8/Gbr/1
CEDAW/C/OP.8/GBR/1 Distr.: General 23 February 2018 Original: English ADVANCE UNEDITED VERSION Committee on the Elimination of Discrimination against Women Report of the inquiry concerning the United Kingdom of Great Britain and Northern Ireland under article 8 of the Optional Protocol to the Convention on the Elimination of All Forms of Discrimination against Women I. Introduction 1. On 9 December 2010, the Committee on the Elimination of Discrimination against Women (Committee) received information from several organisations1 (sources) pursuant to article 8 of the Optional Protocol (OP) to the Convention on the Elimination of All Forms of Discrimination against Women (Convention). The sources allege that the United Kingdom of Great Britain and Northern Ireland (UK) has committed grave and systematic violations of rights under the Convention due to restrictive access to abortion for women and girls in Northern Ireland (NI). 2. The UK ratified the Convention on 7 April 1986 and acceded to the OP on 17 December 2004. II. Submission by the sources of information 3. The sources submit that in NI, assisting with or procuring an abortion is criminalised, punishable by a maximum sentence of life imprisonment2 and the availability of abortion is highly restricted. They allege failure of the UK, inter alia, to: (a) establish a comprehensive legal framework to protect and guarantee NI women’s right to abortion; (b) ensure that NI women are not exposed to the health risks of unsafe abortion; and, (c) address social, practical and financial obstacles in accessing abortion, which disproportionately affect rural women. The sources allege that the legal framework on abortion discriminates against NI women. -
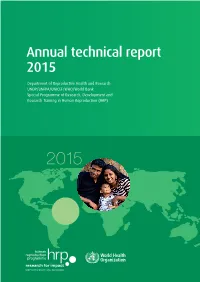
Annual Technical Report 2015
Annual technical report 2015 Department of Reproductive Health and Research UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) 2015 For more information, please contact: Department of Reproductive Health and Research World Health Organization Avenue Appia 20, CH-1211 Geneva 27, Switzerland Fax: +41 22 791 4171 E-mail: [email protected] www.who.int/reproductivehealth Department of Reproductive Health and Research, including the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) Annual Technical Report, 2015 WHO/RHR/HRP/16.08 UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP). Annual Technical Report 2015 © World Health Organization 2016 All rights reserved. Publications of the World Health Organization are available on the WHO website (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications –whether for sale or for non-com- mercial distribution– should be addressed to WHO Press through the WHO website (www.who.int/about/ licensing/copyright_ form/en/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. -

Abortion and the Law in New
NSW PARLIAMENTARY LIBRARY RESEARCH SERVICE Abortion and the law in New South Wales by Talina Drabsch Briefing Paper No 9/05 ISSN 1325-4456 ISBN 0 7313 1784 X August 2005 © 2005 Except to the extent of the uses permitted under the Copyright Act 1968, no part of this document may be reproduced or transmitted in any form or by any means including information storage and retrieval systems, without the prior written consent from the Librarian, New South Wales Parliamentary Library, other than by Members of the New South Wales Parliament in the course of their official duties. Abortion and the law in New South Wales by Talina Drabsch NSW PARLIAMENTARY LIBRARY RESEARCH SERVICE David Clune (MA, PhD, Dip Lib), Manager..............................................(02) 9230 2484 Gareth Griffith (BSc (Econ) (Hons), LLB (Hons), PhD), Senior Research Officer, Politics and Government / Law .........................(02) 9230 2356 Talina Drabsch (BA, LLB (Hons)), Research Officer, Law ......................(02) 9230 2768 Lenny Roth (BCom, LLB), Research Officer, Law ...................................(02) 9230 3085 Stewart Smith (BSc (Hons), MELGL), Research Officer, Environment ...(02) 9230 2798 John Wilkinson (MA, PhD), Research Officer, Economics.......................(02) 9230 2006 Should Members or their staff require further information about this publication please contact the author. Information about Research Publications can be found on the Internet at: www.parliament.nsw.gov.au/WEB_FEED/PHWebContent.nsf/PHPages/LibraryPublications Advice on -

Defending the Human Right to Life in Latin America
Defending the Human Right to Life in Latin America Translated from the Spanish Americans United for Life, Washington, DC 20005 Copyright © 2012 by Americans United for Life All rights reserved First edition published 2012 Published in the United States of America ISBN 978-0-9777204-8-4 Defending the Human Right to Life in Latin America Dr. Charmaine Yoest, President & CEO Editors M. Laura Farfán Bertrán, Lawyer & Project Coordinator William L. Saunders, Senior Vice President & Senior Counsel Jeanneane Maxon, Vice President of External Affairs & Corporate Counsel Translator Noelia Estefanía Marchetti Translated from the Spanish Copyright 2012 by Americans United for Life. All rights reserved under International and Pan-American Copyright Conventions. No part of Defending the Human Right to Life in Latin América may be reproduced or transmitted in any form, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system now known or to be invented, without permission in writing from the publisher, except by a reviewer who wishes to quote brief passages in an article or a review written for inclusion in a magazine, newspaper, or broadcast. For information, please contact: Americans United for Life 655 15th Street NW, Suite 410, Washington, DC 20005, United States of America; 202-289-1478 www.aul.org Table of Contents Introduction – Human Rights and the Right to Life William L. Saunders 11 Overview – Latin America Reaffirms its Commitment to Life M. Laura Farfán Bertrán 15 Legislation Guidelines for Latin America 21 I. General Guidelines to a Constitutional Amendment 21 II. Prohibition of Hormonal “Emergency Contraception” 22 III. Rights Acknowledgement 23 A. -

Constitutionalizing Fetal Rights : a Salutary Tale from Ireland.', Michigan Journal of Gender and the Law., 22 (2)
Durham Research Online Deposited in DRO: 21 April 2015 Version of attached le: Accepted Version Peer-review status of attached le: Peer-reviewed Citation for published item: de Londras, Fiona (2015) 'Constitutionalizing fetal rights : a salutary tale from Ireland.', Michigan journal of gender and the law., 22 (2). pp. 243-289. Further information on publisher's website: http://repository.law.umich.edu/mjgl/vol22/iss2/1 Publisher's copyright statement: Additional information: Use policy The full-text may be used and/or reproduced, and given to third parties in any format or medium, without prior permission or charge, for personal research or study, educational, or not-for-prot purposes provided that: • a full bibliographic reference is made to the original source • a link is made to the metadata record in DRO • the full-text is not changed in any way The full-text must not be sold in any format or medium without the formal permission of the copyright holders. Please consult the full DRO policy for further details. Durham University Library, Stockton Road, Durham DH1 3LY, United Kingdom Tel : +44 (0)191 334 3042 | Fax : +44 (0)191 334 2971 https://dro.dur.ac.uk CONSTITUTIONALIZING FETAL RIGHTS: A SALUTARY TALE FROM IRELAND Fiona de Londras I. Introduction ................................................................................................................................ 1 II. Abortion in Ireland: The Current Legal Regime ............................................................. 4 III. The Constitutionalization of Fetal Rights -

World Health Organization
Sofia Flores Colombres- President Melissa Peniche Yunes - Moderator 1 Daniela Navarro Buendía - First Official assistant World Health Organization of the organization is currently Dr. Tedros Adhanom Topic B: Global access to Ghebreyesus. The World Health Organization is a assisted, safe and legal worldwide standard on medical and related issues in the abortion in special cases modern-day. One of the most relevant and ongoing situations the World Health Organization is currently analyzing is establishing global access to assisted, safe and legal INTRODUCTION abortion in special cases. First of all, the term “abortion” is defined as the removal of pregnancy tissue, products The world has always tried to evolve and adapt to the of conception and placenta from the uterus of a female growth of current medical-related circumstances; to terminate a pregnancy. There are various other terms in order to provide worldwide standards, solutions, for abortion, such as elective abortion, termination of humanitarian aid, and much more. The World Health pregnancy, therapeutic abortion, along with others. Organization (WHO) was officially established on April 7, 1948, after the Constitution adopted by the International Nowadays, abortion policies and laws vary among Health Conference came into place. This organization nations and individual states across the globe, currently counts with 7,000 individuals from 150 depending on each of the countries’ current needs. countries in 150 national offices around the world. It has As a medical definition, abortion is defined as the its headquarters in Geneva. complete removal of a pregnancy. Now, the making of this procedure around the world has different conditions The purpose of the World Health Organization is in what will be illegal and what would lay within the to “promote health, keep the world safe, and serve law.