2,4-D — 2012 03 05
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2,4-Dichlorophenoxyacetic Acid
2,4-Dichlorophenoxyacetic acid 2,4-Dichlorophenoxyacetic acid IUPAC (2,4-dichlorophenoxy)acetic acid name 2,4-D Other hedonal names trinoxol Identifiers CAS [94-75-7] number SMILES OC(COC1=CC=C(Cl)C=C1Cl)=O ChemSpider 1441 ID Properties Molecular C H Cl O formula 8 6 2 3 Molar mass 221.04 g mol−1 Appearance white to yellow powder Melting point 140.5 °C (413.5 K) Boiling 160 °C (0.4 mm Hg) point Solubility in 900 mg/L (25 °C) water Related compounds Related 2,4,5-T, Dichlorprop compounds Except where noted otherwise, data are given for materials in their standard state (at 25 °C, 100 kPa) 2,4-Dichlorophenoxyacetic acid (2,4-D) is a common systemic herbicide used in the control of broadleaf weeds. It is the most widely used herbicide in the world, and the third most commonly used in North America.[1] 2,4-D is also an important synthetic auxin, often used in laboratories for plant research and as a supplement in plant cell culture media such as MS medium. History 2,4-D was developed during World War II by a British team at Rothamsted Experimental Station, under the leadership of Judah Hirsch Quastel, aiming to increase crop yields for a nation at war.[citation needed] When it was commercially released in 1946, it became the first successful selective herbicide and allowed for greatly enhanced weed control in wheat, maize (corn), rice, and similar cereal grass crop, because it only kills dicots, leaving behind monocots. Mechanism of herbicide action 2,4-D is a synthetic auxin, which is a class of plant growth regulators. -

July 6, 2020 OPP Docket Environmental Protection Agency Docket Center (EPA/DC), (28221T) 1200 Pennsylvania Ave. NW Washington
July 6, 2020 OPP Docket Environmental Protection Agency Docket Center (EPA/DC), (28221T) 1200 Pennsylvania Ave. NW Washington, DC 20460-000 Docket ID # EPA-HQ-OPP-2014-0167 Re. Clopyralid, Case Number 7212 Dear Madam/Sir: These comments are submitted on behalf of Beyond Pesticides, Beyond Toxics, Center for Food Safety, Hawai’i Alliance for Progressive Action, Hawai'i SEED, LEAD for Pollinators, Maine Organic Farmers and Gardeners Association, Maryland Pesticide Education Network, Northeast Organic Farming Association—Massachusetts Chapter, Northwest Center for Alternatives to Pesticides, People and Pollinators Action Network, Real Organic Project, Sierra Club, Toxic Free NC, Women’s Voices for the Earth. Founded in 1981 as a national, grassroots, membership organization that represents community-based organizations and a range of people seeking to bridge the interests of consumers, farmers and farmworkers, Beyond Pesticides advances improved protections from pesticides and alternative pest management strategies that reduce or eliminate a reliance on pesticides. Our membership and network span the 50 states and the world. EPA’s proposed interim decision (PID) on the weed killer clopyralid is inadequate to protect property, nontarget plants, and pollinators from exposure to the chemical. Clopyralid poses unreasonable adverse effects that cannot be remedied by EPA’s proposed fixes. It should not be reregistered. Clopyralid has a long history of causing environmental and property damage through drift, runoff, use of treated plant material (such as straw or grass clippings) for mulch or compost, contaminated irrigation water, and urine or manure from animals consuming treated vegetation. Clopyralid (3,6-dichloro-2-pyridinecarboxylic acid) is an herbicide used to control broadleaf weeds on nonresidential lawns and turf, range, pastures, right-of ways and on several crops. -

U.S. EPA, Pesticide Product Label, CLOPYRALID MEA+2,4-D, 07/07/2008
'f-;) 7 S-O - 'ta- \ ENVIRONMENTAL PROTECTION u.s. EPA Reg, Nwnber: Date of Issuance: AGENCY Office of Pesticide Programs 42750-92 Registration Division (7505P) -- 7 JtJL 2DOB Ariel Rios, Building 1200 Pennsylvania Ave., NW Washington, D.C, 20460 NOTICE OF PESTICIDE: Term of Issuance: _ Registration -X Reregistration Name of Pesticide Product: (under FIFRA, as amended) Clopyralid MEA+ 2,4- D Name and Address of Registrant (include ZIP Code): Albaugh, Inc. 121 NE 18th Street Ankeny, IA 50021 N o~e: C.h~nge,~itiIflb~ljllgl,~i:t1~1i~~J9~~~1?~!iUiC~,fJqnf.th~i.:~G~~t~4j#'qqHriet£i~riw,ii4;tl}is, :' ',' ,,',: " registratio"n ~4stl>e ,s~Drriittedto,aPQjl,~9:~pt~qby 'theRe,gi~ttatipn pivisi()i1 prior t9 ':tI~.~"Qn~~)*~eI , ,~:~~~~r:::~.~:;~~:1~~jJ:r~,2t.edf.~,~.&.~~lt;'~I~\~i,~tfl%~~~i;m)~t~~:;'~~/~~·?~~:,)~·¥'t·.'~~~i,~j~:~:i)~.:,;" ,.".;,' "' On the basis of information furnished by the registrant, the above named pesticide is hereby registered/reregistered under the Federal Insecticide, Fungicide and Rodenticide Act. Registration is in no way to be construed as an endorsement or recommendation of this product by the Agency. In order to protect health and the environment, the Administrator, on his motion, may at any time suspend or cancel the registration of a pesticide in accordance with the Act. The acceptance of any name in connection with the registration of a product under this Act is not to be construed as giving the registrant a right to exclusive use of the name or to its use ifit has been covered by others. This product is reregistered in accordance with FIFRA sec. -
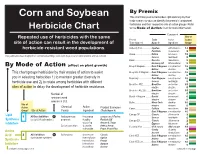
Corn and Soybean Mode of Action Herbicide Chart
By Premix Corn and Soybean This chart lists premix herbicides alphabetically by their trade names so you can identify the premix’s component herbicides and their respective site of action groups. Refer Herbicide Chart to the Mode of Action chart for more information. Component Repeated use of herbicides with the same Site of Premix Trade Active Action site of action can result in the development of Trade Name ® Name ® Ingredient Group* herbicide-resistant weed populations. Authority First ............... Spartan sulfentrazone 14 FirstRate cloransulam 2 Axiom ........................... Define flufenacet 15 This publication was designed for commercial printing, color shifts may occur on other printers and on-screeen. Sencor metribuzin 5 Basis . ........................... Resolve rimsulfuron 2 Harmony GT thifensulfuron 2 By Mode of Action (effect on plant growth) Bicep II Magnum .......... Dual II Magnum s-metolachlor 15 AAtrex atrazine 5 This chart groups herbicides by their modes of action to assist Bicep Lite II Magnum .... Dual II Magnum s-metolachlor 15 AAtrex atrazine 5 you in selecting herbicides 1) to maintain greater diversity in Boundary ...................... Dual Magnum s-metolachlor 15 herbicide use and 2) to rotate among herbicides with different Sencor metribuzin 5 Breakfree ATZ ............... Breakfree acetochlor 15 sites of action to delay the development of herbicide resistance. atrazine atrazine 5 Breakfree ATZ Lite ........ Breakfree acetochlor 15 Number of atrazine atrazine 5 resistant weed Buctril + Atrazine ......... Buctril bromoxynil 6 atrazine atrazine 5 species in U.S. Bullet ............................ Micro-Tech alachlor 15 Site of Chemical Active atrazine atrazine 5 Action Product Examples Camix ........................... Callisto mesotrione 28 Group* Site of Action Family Ingredient (Trade Name ®) Dual II Magnum s-metolachlor 15 Lipid Canopy DF .................. -

Clopyralid 7B.1
Clopyralid 7b.1 CLOPYRALID M. Tu, C. Hurd, R. Robison & J.M. Randall Herbicide Basics Synopsis Clopyralid is an auxin-mimic type herbicide. It is more Chemical formula: 3,6- selective (kills a more limited range of plants) than some dichloro-pyridinecarboxylic other auxin-mimic herbicides like picloram, triclopyr, or acid 2,4-D. Like other auxin-mimics, it has little effect on grasses and other monocots, but also does little harm to Herbicide Family: members of the mustard family (Brassicaceae) and several Pyridine (Picolinic Acid) other groups of broad-leaved plants. Clopyralid controls Target weeds: annual and many annual and perennial broadleaf weeds, particularly of perennial broadleaf weeds, esp. the Asteraceae (sunflower family), Fabaceae (legume knapweeds, thistles, and other family), Solanaceae (nightshade family), Polygonaceae members of the sunflower, (knotweed family), and Violaceae (violet family). It is legume, and knotweed families chemically similar to picloram, but clopyralid has a shorter half-life, is more water-soluble, and has a lower adsorption Forms: salt & ester capacity than picloram. Clopyralid’s half-life in the Formulations: SL, WG environment averages one to two months and ranges up to one year. It is degraded almost entirely by microbial Mode of Action: Auxin mimic metabolism in soils and aquatic sediments. Clopyralid is not Water Solubility: 1,000 ppm degraded by sunlight or hydrolysis. The inability of clopyralid to bind with soils and its persistence implies that Adsorption potential: low clopyralid has the potential to be highly mobile and a Primary degradation mech: contamination threat to water resources and non-target plant Slow microbial metabolism species, although no extensive offsite movement has been documented. -

Herbicide Mode of Action Table High Resistance Risk
Herbicide Mode of Action Table High resistance risk Chemical family Active constituent (first registered trade name) GROUP 1 Inhibition of acetyl co-enzyme A carboxylase (ACC’ase inhibitors) clodinafop (Topik®), cyhalofop (Agixa®*, Barnstorm®), diclofop (Cheetah® Gold* Decision®*, Hoegrass®), Aryloxyphenoxy- fenoxaprop (Cheetah®, Gold*, Wildcat®), fluazifop propionates (FOPs) (Fusilade®), haloxyfop (Verdict®), propaquizafop (Shogun®), quizalofop (Targa®) Cyclohexanediones (DIMs) butroxydim (Factor®*), clethodim (Select®), profoxydim (Aura®), sethoxydim (Cheetah® Gold*, Decision®*), tralkoxydim (Achieve®) Phenylpyrazoles (DENs) pinoxaden (Axial®) GROUP 2 Inhibition of acetolactate synthase (ALS inhibitors), acetohydroxyacid synthase (AHAS) Imidazolinones (IMIs) imazamox (Intervix®*, Raptor®), imazapic (Bobcat I-Maxx®*, Flame®, Midas®*, OnDuty®*), imazapyr (Arsenal Xpress®*, Intervix®*, Lightning®*, Midas®* OnDuty®*), imazethapyr (Lightning®*, Spinnaker®) Pyrimidinyl–thio- bispyribac (Nominee®), pyrithiobac (Staple®) benzoates Sulfonylureas (SUs) azimsulfuron (Gulliver®), bensulfuron (Londax®), chlorsulfuron (Glean®), ethoxysulfuron (Hero®), foramsulfuron (Tribute®), halosulfuron (Sempra®), iodosulfuron (Hussar®), mesosulfuron (Atlantis®), metsulfuron (Ally®, Harmony®* M, Stinger®*, Trounce®*, Ultimate Brushweed®* Herbicide), prosulfuron (Casper®*), rimsulfuron (Titus®), sulfometuron (Oust®, Eucmix Pre Plant®*, Trimac Plus®*), sulfosulfuron (Monza®), thifensulfuron (Harmony®* M), triasulfuron (Logran®, Logran® B-Power®*), tribenuron (Express®), -

INDEX to PESTICIDE TYPES and FAMILIES and PART 180 TOLERANCE INFORMATION of PESTICIDE CHEMICALS in FOOD and FEED COMMODITIES
US Environmental Protection Agency Office of Pesticide Programs INDEX to PESTICIDE TYPES and FAMILIES and PART 180 TOLERANCE INFORMATION of PESTICIDE CHEMICALS in FOOD and FEED COMMODITIES Note: Pesticide tolerance information is updated in the Code of Federal Regulations on a weekly basis. EPA plans to update these indexes biannually. These indexes are current as of the date indicated in the pdf file. For the latest information on pesticide tolerances, please check the electronic Code of Federal Regulations (eCFR) at http://www.access.gpo.gov/nara/cfr/waisidx_07/40cfrv23_07.html 1 40 CFR Type Family Common name CAS Number PC code 180.163 Acaricide bridged diphenyl Dicofol (1,1-Bis(chlorophenyl)-2,2,2-trichloroethanol) 115-32-2 10501 180.198 Acaricide phosphonate Trichlorfon 52-68-6 57901 180.259 Acaricide sulfite ester Propargite 2312-35-8 97601 180.446 Acaricide tetrazine Clofentezine 74115-24-5 125501 180.448 Acaricide thiazolidine Hexythiazox 78587-05-0 128849 180.517 Acaricide phenylpyrazole Fipronil 120068-37-3 129121 180.566 Acaricide pyrazole Fenpyroximate 134098-61-6 129131 180.572 Acaricide carbazate Bifenazate 149877-41-8 586 180.593 Acaricide unclassified Etoxazole 153233-91-1 107091 180.599 Acaricide unclassified Acequinocyl 57960-19-7 6329 180.341 Acaricide, fungicide dinitrophenol Dinocap (2, 4-Dinitro-6-octylphenyl crotonate and 2,6-dinitro-4- 39300-45-3 36001 octylphenyl crotonate} 180.111 Acaricide, insecticide organophosphorus Malathion 121-75-5 57701 180.182 Acaricide, insecticide cyclodiene Endosulfan 115-29-7 79401 -

US EPA, Pesticide Product Label, Alligare Clopyralid 3 SL,10/09/2018
U.S. ENVIRONMENTAL PROTECTION AGENCY EPA Reg. Number: Date of Issuance: Office of Pesticide Programs Registration Division (7505P) 81927-69 10/9/18 1200 Pennsylvania Ave., N.W. Washington, D.C. 20460 NOTICE OF PESTICIDE: Term of Issuance: X Registration Reregistration Conditional (under FIFRA, as amended) Name of Pesticide Product: Alligare Clopyralid 3 SL Name and Address of Registrant (include ZIP Code): Michael Kellogg Agent for Alligare, LLC c/o Pyxis Regulatory Consulting, Inc. 4110 136th St. Ct. NW Gig Harbor, WA 98332 Note: Changes in labeling differing in substance from that accepted in connection with this registration must be submitted to and accepted by the Registration Division prior to use of the label in commerce. In any correspondence on this product always refer to the above EPA registration number. On the basis of information furnished by the registrant, the above named pesticide is hereby registered under the Federal Insecticide, Fungicide, and Rodenticide Act (FIFRA). Registration is in no way to be construed as an endorsement or recommendation of this product by the Agency. In order to protect health and the environment, the Administrator, on his motion, may at any time suspend or cancel the registration of a pesticide in accordance with the Act. The acceptance of any name in connection with the registration of a product under this Act is not to be construed as giving the registrant a right to exclusive use of the name or to its use if it has been covered by others. This product is conditionally registered in accordance with FIFRA section 3(c)(7)(A). -

List of Herbicide Groups
List of herbicides Group Scientific name Trade name clodinafop (Topik®), cyhalofop (Barnstorm®), diclofop (Cheetah® Gold*, Decision®*, Hoegrass®), fenoxaprop (Cheetah® Gold* , Wildcat®), A Aryloxyphenoxypropionates fluazifop (Fusilade®, Fusion®*), haloxyfop (Verdict®), propaquizafop (Shogun®), quizalofop (Targa®) butroxydim (Falcon®, Fusion®*), clethodim (Select®), profoxydim A Cyclohexanediones (Aura®), sethoxydim (Cheetah® Gold*, Decision®*), tralkoxydim (Achieve®) A Phenylpyrazoles pinoxaden (Axial®) azimsulfuron (Gulliver®), bensulfuron (Londax®), chlorsulfuron (Glean®), ethoxysulfuron (Hero®), foramsulfuron (Tribute®), halosulfuron (Sempra®), iodosulfuron (Hussar®), mesosulfuron (Atlantis®), metsulfuron (Ally®, Harmony®* M, Stinger®*, Trounce®*, B Sulfonylureas Ultimate Brushweed®* Herbicide), prosulfuron (Casper®*), rimsulfuron (Titus®), sulfometuron (Oust®, Eucmix Pre Plant®*), sulfosulfuron (Monza®), thifensulfuron (Harmony®* M), triasulfuron, (Logran®, Logran® B Power®*), tribenuron (Express®), trifloxysulfuron (Envoke®, Krismat®*) florasulam (Paradigm®*, Vortex®*, X-Pand®*), flumetsulam B Triazolopyrimidines (Broadstrike®), metosulam (Eclipse®), pyroxsulam (Crusader®Rexade®*) imazamox (Intervix®*, Raptor®,), imazapic (Bobcat I-Maxx®*, Flame®, Midas®*, OnDuty®*), imazapyr (Arsenal Xpress®*, Intervix®*, B Imidazolinones Lightning®*, Midas®*, OnDuty®*), imazethapyr (Lightning®*, Spinnaker®) B Pyrimidinylthiobenzoates bispyribac (Nominee®), pyrithiobac (Staple®) C Amides: propanil (Stam®) C Benzothiadiazinones: bentazone (Basagran®, -

Clopyralid (Transline) - Final Report
SERA TR 99-21-11/12-01d Clopyralid (Transline) - Final Report Prepared for: USDA, Forest Service Task Nos. 11/12 USDA/FS Contract No. 53-3187-5-12 USDA/FS Order Nos.43-3187-8-0167 and 43-3187-8-0220 Submitted to: Leslie Rubin, COTR Animal and Plant Health Inspection Service (APHIS) Biotechnology, Biologics and Environmental Protection Environmental Analysis and Documentation United States Department of Agriculture Suite 5A44, Unit 149 4700 River Road Riverdale, MD 20737 Submitted by: Syracuse Environmental Research Associates, Inc. 5100 Highbridge St., 42C Fayetteville, New York 13066-0950 Telephone: (315) 637-9560 Fax: (315) 637-0445 Internet: [email protected] Report Date: April 11, 1999 TABLE OF CONTENTS LIST OF TABLES ......................................................... v ACRONYMS, ABBREVIATIONS, AND SYMBOLS ............................. vi COMMON UNIT CONVERSIONS ........................................... viii CONVERSION OF SCIENTIFIC NOTATION ................................... ix EXECUTIVE SUMMARY ....................................................x 1. INTRODUCTION ...................................................... 1-1 2. PROGRAM DESCRIPTION .............................................. 2-1 2.1. OVERVIEW ...................................................... 2-1 2.2. CHEMICAL DESCRIPTION AND COMMERCIAL FORMULATIONS ........ 2-2 2.3. APPLICATION METHODS .......................................... 2-2 2.4. MIXING AND APPLICATION RATES ................................. 2-4 3. HUMAN HEALTH RISK ASSESSMENT .................................. -

Chemical Weed Control
2014 North Carolina Agricultural Chemicals Manual The 2014 North Carolina Agricultural Chemicals Manual is published by the North Carolina Cooperative Extension Service, College of Agriculture and Life Sciences, N.C. State University, Raleigh, N.C. These recommendations apply only to North Carolina. They may not be appropriate for conditions in other states and may not comply with laws and regulations outside North Carolina. These recommendations are current as of November 2013. Individuals who use agricultural chemicals are responsible for ensuring that the intended use complies with current regulations and conforms to the product label. Be sure to obtain current information about usage regulations and examine a current product label before applying any chemical. For assistance, contact your county Cooperative Extension agent. The use of brand names and any mention or listing of commercial products or services in this document does not imply endorsement by the North Carolina Cooperative Extension Service nor discrimination against similar products or services not mentioned. VII — CHEMICAL WEED CONTROL 2014 North Carolina Agricultural Chemicals Manual VII — CHEMICAL WEED CONTROL Chemical Weed Control in Field Corn ...................................................................................................... 224 Weed Response to Preemergence Herbicides — Corn ........................................................................... 231 Weed Response to Postemergence Herbicides — Corn ........................................................................ -

Recommended Classification of Pesticides by Hazard and Guidelines to Classification 2019 Theinternational Programme on Chemical Safety (IPCS) Was Established in 1980
The WHO Recommended Classi cation of Pesticides by Hazard and Guidelines to Classi cation 2019 cation Hazard of Pesticides by and Guidelines to Classi The WHO Recommended Classi The WHO Recommended Classi cation of Pesticides by Hazard and Guidelines to Classi cation 2019 The WHO Recommended Classification of Pesticides by Hazard and Guidelines to Classification 2019 TheInternational Programme on Chemical Safety (IPCS) was established in 1980. The overall objectives of the IPCS are to establish the scientific basis for assessment of the risk to human health and the environment from exposure to chemicals, through international peer review processes, as a prerequisite for the promotion of chemical safety, and to provide technical assistance in strengthening national capacities for the sound management of chemicals. This publication was developed in the IOMC context. The contents do not necessarily reflect the views or stated policies of individual IOMC Participating Organizations. The Inter-Organization Programme for the Sound Management of Chemicals (IOMC) was established in 1995 following recommendations made by the 1992 UN Conference on Environment and Development to strengthen cooperation and increase international coordination in the field of chemical safety. The Participating Organizations are: FAO, ILO, UNDP, UNEP, UNIDO, UNITAR, WHO, World Bank and OECD. The purpose of the IOMC is to promote coordination of the policies and activities pursued by the Participating Organizations, jointly or separately, to achieve the sound management of chemicals in relation to human health and the environment. WHO recommended classification of pesticides by hazard and guidelines to classification, 2019 edition ISBN 978-92-4-000566-2 (electronic version) ISBN 978-92-4-000567-9 (print version) ISSN 1684-1042 © World Health Organization 2020 Some rights reserved.