Cingulum Stimulation Enhances Positive Affect and Anxiolysis to Facilitate Awake Craniotomy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Microstructural White Matter Alterations and Hippocampal Volumes Are
6 178 S Fjalldal and others Diffusion tensor imaging in 178:6 577–587 Clinical Study craniopharyngioma Microstructural white matter alterations and hippocampal volumes are associated with cognitive deficits in craniopharyngioma S Fjalldal1, C Follin1, D Svärd2, L Rylander3, S Gabery4, Å Petersén4, D van Westen2, P C Sundgren2,5, I M Björkman-Burtscher2,5, J Lätt5, B Ekman6, A Johanson7 and E M Erfurth1 1Department of Endocrinology, Skåne University Hospital, Lund, Sweden, 2Department of Diagnostic Radiology, Clinical Sciences, 3Division of Occupational and Environmental Medicine, 4Translational Neuroendocrine Research Unit, Department 5 of Experimental Medical Science, Lund University, Lund, Sweden, Department of Medical Imaging and Physiology, Correspondence 6 Skåne University Hospital, Lund, Sweden, Department of Endocrinology and Medical and Health Sciences, should be addressed 7 Linköping University, Linköping, Sweden, and Department of Psychology and Psychiatry, Skåne University Hospital, to E M Erfurth Lund, Sweden Email [email protected] Abstract Context: Patients with craniopharyngioma (CP) and hypothalamic lesions (HL) have cognitive deficits. Which neural pathways are affected is unknown. Objective: To determine whether there is a relationship between microstructural white matter (WM) alterations detected with diffusion tensor imaging (DTI) and cognition in adults with childhood-onset CP. Design: A cross-sectional study with a median follow-up time of 22 (6–49) years after operation. Setting: The South Medical Region of Sweden (2.5 million inhabitants). Participants: Included were 41 patients (24 women, ≥17 years) surgically treated for childhood-onset CP between 1958–2010 and 32 controls with similar age and gender distributions. HL was found in 23 patients. Main outcome measures: Subjects performed cognitive tests and magnetic resonance imaging, and images were analyzed using DTI of uncinate fasciculus, fornix, cingulum, hippocampus and hypothalamus as well as hippocampal European Journal European of Endocrinology volumetry. -

10041.Full.Pdf
The Journal of Neuroscience, July 23, 2014 • 34(30):10041–10054 • 10041 Systems/Circuits Frontal Cortical and Subcortical Projections Provide a Basis for Segmenting the Cingulum Bundle: Implications for Neuroimaging and Psychiatric Disorders Sarah R. Heilbronner and Suzanne N. Haber Department of Pharmacology and Physiology, University of Rochester Medical Center, Rochester, New York 14642 The cingulum bundle (CB) is one of the brain’s major white matter pathways, linking regions associated with executive function, decision-making, and emotion. Neuroimaging has revealed that abnormalities in particular locations within the CB are associated with specific psychiatric disorders, including depression and bipolar disorder. However, the fibers using each portion of the CB remain unknown. In this study, we used anatomical tract-tracing in nonhuman primates (Macaca nemestrina, Macaca fascicularis, Macaca mulatta)toexaminetheorganizationofspecificcingulate,noncingulatefrontal,andsubcorticalpathwaysthroughtheCB.Thegoalswere as follows: (1) to determine connections that use the CB, (2) to establish through which parts of the CB these fibers travel, and (3) to relate the CB fiber pathways to the portions of the CB identified in humans as neurosurgical targets for amelioration of psychiatric disorders. Results indicate that cingulate, noncingulate frontal, and subcortical fibers all travel through the CB to reach both cingulate and noncin- gulate targets. However, many brain regions send projections through only part, not all, of the CB. For example, amygdala fibers are not present in the caudal portion of the dorsal CB. These results allow segmentation of the CB into four unique zones. We identify the specific connections that are abnormal in psychiatric disorders and affected by neurosurgical interventions, such as deep brain stimulation and cingulotomy. -

White Matter Abnormalities in Adults with Bipolar Disorder Type-II
www.nature.com/scientificreports OPEN White matter abnormalities in adults with bipolar disorder type‑II and unipolar depression Anna Manelis1*, Adriane Soehner1, Yaroslav O. Halchenko2, Skye Satz1, Rachel Ragozzino1, Mora Lucero1, Holly A. Swartz1, Mary L. Phillips1 & Amelia Versace1 Discerning distinct neurobiological characteristics of related mood disorders such as bipolar disorder type‑II (BD‑II) and unipolar depression (UD) is challenging due to overlapping symptoms and patterns of disruption in brain regions. More than 60% of individuals with UD experience subthreshold hypomanic symptoms such as elevated mood, irritability, and increased activity. Previous studies linked bipolar disorder to widespread white matter abnormalities. However, no published work has compared white matter microstructure in individuals with BD‑II vs. UD vs. healthy controls (HC), or examined the relationship between spectrum (dimensional) measures of hypomania and white matter microstructure across those individuals. This study aimed to examine fractional anisotropy (FA), radial difusivity (RD), axial difusivity (AD), and mean difusivity (MD) across BD‑II, UD, and HC groups in the white matter tracts identifed by the XTRACT tool in FSL. Individuals with BD‑II (n = 18), UD (n = 23), and HC (n = 24) underwent Difusion Weighted Imaging. The categorical approach revealed decreased FA and increased RD in BD‑II and UD vs. HC across multiple tracts. While BD‑II had signifcantly lower FA and higher RD values than UD in the anterior part of the left arcuate fasciculus, UD had signifcantly lower FA and higher RD values than BD‑II in the area of intersections between the right arcuate, inferior fronto‑occipital and uncinate fasciculi and forceps minor. -

The Papez Circuit & Perforant Pathway
The Papez Circuit & Perforant Pathway Neurology/Neurosciences - CME/MOC > Sleep, Memory, Movement > Sleep, Memory, Movement HIPPOCAMPAL PHYSIOLOGY: THE PAPEZ CIRCUIT & PERFORANT PATHWAY THE PAPEZ CIRCUIT: OVERVIEW Papez Circuit Physiology • It is the fundamental extra-hippocampal circuitry, which Papez introduced in 1937. • Originally believed to play a fundamental role in emotional processing/regulation but is now understood to be the cornerstone of memory processing/consolidation, instead. Steps The entorhinal cortex -> hippocampus -> mammillary nuclei -> anterior thalamic nuclei -> cingulate gyrus -> back to the entorhinal cortex* THE PERFORANT PATHWAY: OVERVIEW Perforant Pathway • The key intra-hippocampal circuitry (so-named because the entorhinal cortex projects through (perforates) the subiculum). • Whereas most cortical projections are bidirectional, the perforant pathway follows a specific unidirectional progression. Steps • Hippocampus: The dentate gyrus -> CA3 -> CA1 (via Schaffer collaterals) -> subiculum THE PAPEZ CIRCUIT: ANATOMY Key structures: the parahippocampal gyrus, the entorhinal cortex, the hippocampus, the anterior thalamic nucleus, mammillary nucleus, and the cingulate gyrus and specify the neocortex (external to it). • The entorhinal cortex projects to the hippocampus. • The hippocampus projects via the fornix to the mammillary nuclei. • The mammillary nuclei project to the anterior thalamic nuclei via the mammillothalamic fasciculus (aka the Vicq d'Azyr bundle). • The anterior thalamic nuclei project to the cingulate gyrus. • The cingulate gyrus projects back to the entorhinal cortex via the cingulum to close the Papez circuit loop. The fornix divides into: 1 / 2 • Crus — vertical ascent. • Body — anterior projection underneath the corpus callosum. • Column — descent. Note that the fornix descends both anterior and posterior to the anterior commissure. Key extra-hippocampal projections. • The cingulate gyrus has reciprocal connections with the neocortex. -

The Nomenclature of Human White Matter Association Pathways: Proposal for a Systematic Taxonomic Anatomical Classification
The Nomenclature of Human White Matter Association Pathways: Proposal for a Systematic Taxonomic Anatomical Classification Emmanuel Mandonnet, Silvio Sarubbo, Laurent Petit To cite this version: Emmanuel Mandonnet, Silvio Sarubbo, Laurent Petit. The Nomenclature of Human White Matter Association Pathways: Proposal for a Systematic Taxonomic Anatomical Classification. Frontiers in Neuroanatomy, Frontiers, 2018, 12, pp.94. 10.3389/fnana.2018.00094. hal-01929504 HAL Id: hal-01929504 https://hal.archives-ouvertes.fr/hal-01929504 Submitted on 21 Nov 2018 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. REVIEW published: 06 November 2018 doi: 10.3389/fnana.2018.00094 The Nomenclature of Human White Matter Association Pathways: Proposal for a Systematic Taxonomic Anatomical Classification Emmanuel Mandonnet 1* †, Silvio Sarubbo 2† and Laurent Petit 3* 1Department of Neurosurgery, Lariboisière Hospital, Paris, France, 2Division of Neurosurgery, Structural and Functional Connectivity Lab, Azienda Provinciale per i Servizi Sanitari (APSS), Trento, Italy, 3Groupe d’Imagerie Neurofonctionnelle, Institut des Maladies Neurodégénératives—UMR 5293, CNRS, CEA University of Bordeaux, Bordeaux, France The heterogeneity and complexity of white matter (WM) pathways of the human brain were discretely described by pioneers such as Willis, Stenon, Malpighi, Vieussens and Vicq d’Azyr up to the beginning of the 19th century. -

Relationships Between Hippocampal Atrophy, White Matter Disruption, and Gray Matter Hypometabolism in Alzheimer's Disease
6174 • The Journal of Neuroscience, June 11, 2008 • 28(24):6174–6181 Neurobiology of Disease Relationships between Hippocampal Atrophy, White Matter Disruption, and Gray Matter Hypometabolism in Alzheimer’s Disease Nicolas Villain,1 Be´atrice Desgranges,1 Fausto Viader,1,2 Vincent de la Sayette,1,2 Florence Me´zenge,1 Brigitte Landeau,1 Jean-Claude Baron,3 Francis Eustache,1 and Gae¨l Che´telat1 1Institut National de la Sante´ et de la Recherche Me´dicale–Ecole Pratique des Hautes Etudes–Universite´ de Caen/Basse-Normandie, Unite´ U923, Groupement d’Inte´reˆt Public Cyceron, Centre Hospitalier Universitaire (CHU) Coˆte de Nacre, 14074 Caen, France, 2De´partement de Neurologie, CHU Coˆte de Nacre, 14033 Caen Cedex, France, and 3Department of Clinical Neurosciences, Neurology Unit, University of Cambridge, Cambridge CB2 2SP, United Kingdom In early Alzheimer’s disease (AD), the hippocampal region is the area most severely affected by cellular and structural alterations, yet glucose hypometabolism predominates in the posterior association cortex and posterior cingulate gyrus. One prevalent hypothesis to account for this discrepancy is that posterior cingulate hypometabolism results from disconnection from the hippocampus through disruptionofthecingulumbundle.However,onlypartialandindirectevidencecurrentlysupportsthishypothesis.Thus,usingstructural 18 magnetic resonance imaging and 2-[ F]fluoro-2-deoxy-D-glucose positron emission tomography in 18 patients with early AD, we assessed the relationships between hippocampal atrophy, white matter integrity, and gray matter metabolism by means of a whole-brain voxel-based correlative approach. We found that hippocampal atrophy is specifically related to cingulum bundle disruption, which is in turn highly correlated to hypometabolism of the posterior cingulate cortex but also of the middle cingulate gyrus, thalamus, mammillary bodies, parahippocampal gyrus, and hippocampus (all part of Papez’s circuit), as well as the right temporoparietal associative cortex. -
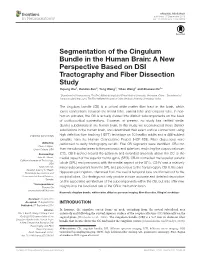
Segmentation of the Cingulum Bundle in the Human Brain
ORIGINAL RESEARCH published: 07 September 2016 doi: 10.3389/fnana.2016.00084 Segmentation of the Cingulum Bundle in the Human Brain: A New Perspective Based on DSI Tractography and Fiber Dissection Study Yupeng Wu 1, Dandan Sun 2, Yong Wang 1, Yibao Wang 1 and Shaowu Ou 1* 1 Department of Neurosurgery, The First Affiliated Hospital of China Medical University, Shenyang, China, 2 Department of Cardiovascular Ultrasound, The First Affiliated Hospital of China Medical University, Shenyang, China The cingulum bundle (CB) is a critical white matter fiber tract in the brain, which forms connections between the frontal lobe, parietal lobe and temporal lobe. In non- human primates, the CB is actually divided into distinct subcomponents on the basis of corticocortical connections. However, at present, no study has verified similar distinct subdivisions in the human brain. In this study, we reconstructed these distinct subdivisions in the human brain, and determined their exact cortical connections using high definition fiber tracking (HDFT) technique on 10 healthy adults and a 488-subject template from the Human Connectome Project (HCP-488). Fiber dissections were Edited by: performed to verify tractography results. Five CB segments were identified. CB-I ran Dave J. Hayes, Union College, USA from the subrostral areas to the precuneus and splenium, encircling the corpus callosum Reviewed by: (CC). CB-II arched around the splenium and extended anteriorly above the CC to the John M. Allman, medial aspect of the superior frontal gyrus (SFG). CB-III connected the superior parietal California Institute of Technology, USA lobule (SPL) and precuneus with the medial aspect of the SFG. -

White Matter Anatomy: What the Radiologist Needs to Know
White Matter Anatomy What the Radiologist Needs to Know Victor Wycoco, MBBS, FRANZCRa, Manohar Shroff, MD, DABR, FRCPCa,*, Sniya Sudhakar, MBBS, DNB, MDb, Wayne Lee, MSca KEYWORDS Diffusion tensor imaging (DTI) White matter tracts Projection fibers Association Fibers Commissural fibers KEY POINTS Diffusion tensor imaging (DTI) has emerged as an excellent tool for in vivo demonstration of white matter microstructure and has revolutionized our understanding of the same. Information on normal connectivity and relations of different white matter networks and their role in different disease conditions is still evolving. Evidence is mounting on causal relations of abnormal white matter microstructure and connectivity in a wide range of pediatric neurocognitive and white matter diseases. Hence there is a pressing need for every neuroradiologist to acquire a strong basic knowledge of white matter anatomy and to make an effort to apply this knowledge in routine reporting. INTRODUCTION (Fig. 1). However, the use of specific DTI sequences provides far more detailed and clini- DTI has allowed in vivo demonstration of axonal cally useful information. architecture and connectivity. This technique has set the stage for numerous studies on normal and abnormal connectivity and their role in devel- DIFFUSION TENSOR IMAGING: THE BASICS opmental and acquired disorders. Referencing established white matter anatomy, DTI atlases, Using appropriate magnetic field gradients, and neuroanatomical descriptions, this article diffusion-weighted sequences can be used to summarizes the major white matter anatomy and detect the motion of the water molecules to and related structures relevant to the clinical neurora- from cells. This free movement of the water mole- diologist in daily practice. -
Essential Neuromodulation This Page Intentionally Left Blank Essential Neuromodulation
Essential Neuromodulation This page intentionally left blank Essential Neuromodulation Jeffrey E. Arle Director, Functional Neurosurgery and Research, Department of Neurosurgery Lahey Clinic Burlington, MA Associate Professor of Neurosurgery Tufts University School of Medicine, Boston, MA Jay L. Shils Director of Intraoperative Monitoring, Dept of Neurosurgery Lahey Clinic Burlington, MA AMSTERDAM • BOSTON • HEIDELBERG • LONDON NEW YORK • OXFORD • PARIS • SAN DIEGO SAN FRANCISCO • SINGAPORE • SYDNEY • TOKYO Academic Press is an Imprint of Elsevier Academic Press is an imprint of Elsevier 32 Jamestown Road, London NW1 7BY, UK 30 Corporate Drive, Suite 400, Burlington, MA 01803, USA 525 B Street, Suite 1800, San Diego, CA 92101-4495, USA First edition 2011 Copyright © 2011 Elsevier Inc. All rights reserved No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means electronic, mechanical, photocopying, recording or otherwise without the prior written permission of the publisher Permissions may be sought directly from Elsevier's Science & Technology Rights Department in Oxford, UK: phone ( + 44) (0) 1865 843830; fax ( +44) (0) 1865 853333; email: [email protected]. Alternatively, visit the Science and Technology Books website at www.elsevierdirect.com/rights for further information Notice No responsibility is assumed by the publisher for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of -

Recollection Et Familiarité Chez 12 Patients Présentant Un Infarctus
Recollection et familiarité chez 12 patients présentant un infarctus thalamique gauche : étude comportementale, en imagerie structurale et fonctionnelle de repos Lola Danet To cite this version: Lola Danet. Recollection et familiarité chez 12 patients présentant un infarctus thalamique gauche : étude comportementale, en imagerie structurale et fonctionnelle de repos. Neurosciences. Université Paul Sabatier - Toulouse III, 2015. Français. NNT : 2015TOU30335. tel-01453172 HAL Id: tel-01453172 https://tel.archives-ouvertes.fr/tel-01453172 Submitted on 2 Feb 2017 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. 1 « c’est, on l’a dit, une réflexion nostalgique sur l’impuissance de la réalité à recomposer les tableaux de la mémoire. » Antoine Compagnon, à propos de la Recherche du temps perdu de Marcel Proust. 2 A Yvette Rose Loria et à Charlotte Danet 3 Je remercie Jean-François Démonet et Christine Bastin pour avoir bien voulu évaluer mon travail. Je remercie Olivier Félician, Christopher Moulin et Patrice Péran d’avoir accepté de faire partie de mon jury de thèse. Jérémie Pariente, directeur de ma thèse, mais aussi collègue et partenaire de réflexion scientifique et clinique depuis plusieurs années. Merci pour cette belle aventure, les aventures passées et futures, merci pour ton engagement, ton exigence et ta sincérité. -

A Revised Limbic System Model for Memory, Emotion and Behaviour
Neuroscience and Biobehavioral Reviews 37 (2013) 1724–1737 Contents lists available at ScienceDirect Neuroscience and Biobehavioral Reviews j ournal homepage: www.elsevier.com/locate/neubiorev Review A revised limbic system model for memory, emotion and behaviour a,∗ a,b,c a,d,∗ Marco Catani , Flavio Dell’Acqua , Michel Thiebaut de Schotten a Natbrainlab, Department of Forensic and Neurodevelopmental Sciences, Institute of Psychiatry, King’s College London, UK b Department of Neuroimaging Sciences, Institute of Psychiatry, King’s College London, UK c NIHR Biomedical Research Centre for Mental Health at South London and Maudsley NHS Foundation Trust and Institute of Psychiatry, King’s College London, UK d UMR S 975; CNRS UMR 7225, Centre de Recherche de l’Institut du Cerveau et de la Moelle épinière, Groupe Hospitalier Pitié-Salpêtrière, 75013 Paris, France a r t i c l e i n f o a b s t r a c t Article history: Emotion, memories and behaviour emerge from the coordinated activities of regions connected by the Received 27 November 2012 limbic system. Here, we propose an update of the limbic model based on the seminal work of Papez, Received in revised form 15 May 2013 Yakovlev and MacLean. In the revised model we identify three distinct but partially overlapping networks: Accepted 1 July 2013 (i) the Hippocampal-diencephalic and parahippocampal-retrosplenial network dedicated to memory and spatial orientation; (ii) The temporo-amygdala-orbitofrontal network for the integration of visceral sen- Keywords: sation and emotion with semantic memory and behaviour; (iii) the default-mode network involved in Limbic system autobiographical memories and introspective self-directed thinking. -
Neuromodulation for Intractable Pain • Tipu Aziz and Alex Green Neuromodulation for Intractable Pain
Neuromodulation for Intractable Neuromodulation for Pain • Tipu Aziz and Alex Green Neuromodulation for Intractable Pain Edited by Tipu Aziz and Alex Green Printed Edition of the Special Issue Published in Brain Sciences www.mdpi.com/journal/brainsci Neuromodulation for Intractable Pain Neuromodulation for Intractable Pain Special Issue Editors Tipu Aziz Alex Green MDPI • Basel • Beijing • Wuhan • Barcelona • Belgrade • Manchester • Tokyo • Cluj • Tianjin Special Issue Editors Tipu Aziz Alex Green University of Oxford University of Oxford UK UK Editorial Office MDPI St. Alban-Anlage 66 4052 Basel, Switzerland This is a reprint of articles from the Special Issue published online in the open access journal Brain Sciences (ISSN 2076-3425) (available at: https://www.mdpi.com/journal/brainsci/special issues/neuromodulation pain). For citation purposes, cite each article independently as indicated on the article page online and as indicated below: LastName, A.A.; LastName, B.B.; LastName, C.C. Article Title. Journal Name Year, Article Number, Page Range. ISBN 978-3-03936-950-8 (Hbk) ISBN 978-3-03936-951-5 (PDF) c 2020 by the authors. Articles in this book are Open Access and distributed under the Creative Commons Attribution (CC BY) license, which allows users to download, copy and build upon published articles, as long as the author and publisher are properly credited, which ensures maximum dissemination and a wider impact of our publications. The book as a whole is distributed by MDPI under the terms and conditions of the Creative Commons license CC BY-NC-ND. Contents About the Special Issue Editors ..................................... vii Alexander L. Green and Tipu Z.