AAIB Bulletin 10/2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Safety Spot Winter Protection and Some Hazards
SAFETY SPOT WINTER PROTECTION AND SOME HAZARDS Take precautions over winter, plus valve spring failure, elevator trim and wing spar issues – With Malcolm McBride another packed report Airworthiness Engineer uletide Greetings. Yes, here we are again in the last few bars of the annual melody which goes by the title of Another Year in Our Lives. In my case (and I hope yours) it’s a great tune but, and I don’t want to appear Ygrumpy, the conductor seems to be playing through the chart much faster than he used to. Perhaps it’s just my imagination because, as I get older, I can now get my head around some of the more difficult phrases. As I write the first few lines of this Christmas edition of Safety Spot, Ho Ho, Hum Hum, I’m reminded of the advice given to me by an old(er) muso friend of mine when I asked him how on earth we were supposed to fit all those notes into one particularly busy phrase. “Oh,” he said, “I only play every other note, there’s plenty of time for that.” There’s a lesson in there somewhere! I hope that you and those around you are well and you haven’t spent so much of your budget on your lovely flying machine (if of course, you are lucky enough to own such a craft) that you’ve had to cut down on the heating. Whilst I’m on the subject of heating, take a look at the picture supplied by LAAer Chris Marsh showing the warm-air engine de-humidifier keeping the internals of his Van’s RV-9’s Lycoming O-320 nice and, well, de-humidified. -

Nando Groppo TRAIL with This Form
Amateur-Built Fabrication and Assembly Checklist (2011) Fixed Wing NOTE: This checklist is only applicable to Name(s) Nando Groppo (Lone Palm Aero LLC) fixed wing aircraft. Evaluation of other types of aircraft (i.e., rotorcraft, balloons, Address: 3522 SW 52nd Ave. Bushnell, FL 33513 lighter than air) will not be accomplished Aircraft Model: Nando Groppo TRAIL with this form. Date: On-Site Evaluation August 19-20, 2014 NOTE: This checklist is invalid for and Remarks: This Kit is defined by will not be used to evaluate an altered or modified type certificated aircraft with the intent to issue an Experimental Amateur- built Airworthiness Certificate. Such action Trail Kit Bill of Materials, Release 1.0 dated August 31st, 2015 violates FAA policy and DOES NOT meet the intent of § 21.191(g). Instructions For Using The Amateur-Built Fabrication and Assembly Checklist (2011): A point (each task equals 1 point) can be divided over multiple categories (Manufacturer, Commercial Assistance, Amateur Builder Assembly and Amateur Builder Fabrication) into 1/10 fractions. A Manufacturer may be a kit manufacturer, a component manufacturer or a part(s) manufacturer. Commercial assistance (for hire or compensation) may include assistance provided by kit manufacturers, commercial assistance centers, individuals (e.g. A& P mechanics or avionics technicians). For example, 0.5 (half point) can be assigned to the Manufacturer, 0.3 (3/10 - 3 tenths) as Commercial Assistance, 0.2 to the Amateur Builder as Fabrication, for a total of 1 point. Enter “N/A” in any box where a listed task is not applicable to the particular aircraft being evaluated. -

Revised Listing of Amateur Built Aircraft Kits
REVISED LISTING OF AMATEUR-BUILT AIRCRAFT KITS Updated on: June 22, 2021 The following is a revised listing of aircraft kits that have been evaluated and found eligible in meeting the “major portion” requirement of Title 14, Code of Federal Regulations (14 CFR) Part 21, Certification Procedures for Products and Parts, specifically, § 21.191(g). • This listing is only representative of those kits where the kit manufacturer or distributor requested an evaluation by the Federal Aviation Administration (FAA) for eligibility and should not be construed as meaning the kit(s) are FAA “certified,” “certificated,” or “approved.” • There are other aircraft kits that may allow a builder to meet the “major portion” requirement of § 21.191(g), but those manufacturers or distributors have not requested an FAA evaluation. • The placement of an aircraft kit on this list is not a prerequisite for airworthiness certification. • The primary purpose of this listing is to assist FAA Inspectors/Designees and other interested individuals by eliminating the duplication of evaluations for “major portion” determination when the aircraft is presented for airworthiness certification as an “Amateur-Built Experimental.” • Kit manufacturers or distributors whose status is unknown are identified with a question (?) mark and their address has been deleted. Additional Information and Guidance • Advisory Circular (AC) 20-27G, Certification and Operation of Amateur-Built Aircraft. • FAA Order 8130.35B, Amateur-Built Aircraft National Kit Evaluation Team • Contact your local FAA Flight Standards District Office (FSDO) or Manufacturing Inspection District Office (MIDO). Those publications and other information pertaining to amateur-built experimental aircraft are available online at http://www.faa.gov/aircraft. -

Police Aviation News 288 April 2020 1 # ©Police Aviation Research Issue
Police Aviation News 288 April 2020 1 ©Police Aviation Research Issue 288 April 2020 Police Aviation News 288 April 2020 2 EDITORIAL I think it is fair to say that events are going further and faster than anyone had predicted just 30 days ago. Fortunately, despite the clear distraction of the virus, there is ordinary news out there. Most, if not all, governments are guiding the Coronavirus/COVID-19 crisis by the seat of their political pants. Despite the probing questions by journalists who have time to read and digest everything at their own pace, most politicians lack the shrewd analytical mind of a genius and it shows. Inject forty different opinions into a policy making session and what comes out is at best unclear. No one knows where this will end so we can but hope that for us individually it is a good outcome. Ask any emergency air support unit what planning they have made for a COVID-19 scenario and the an- swer is going to be none. It is new and unprecedented, and you can be sure the aeronautical rule books do not cater for it. What happens when a mission outside the rule book is called for? Operators flying Pub- lic Use/State Aircraft are going to be at a greater advantage than those that have signed up to the EASA or FAA rule book. Someone somewhere may well need to make a decision to overlook the rules (and hope they get away with it). My recent comment that the “shortage of cash flow may seriously effect philanthropy [air ambulances may need to rely a little more upon those reserves]” has now come to the fore. -

Consultation Response PA14. Welsh Local Government Association PDF
NAfW inquiry into international connectivity through Welsh ports and airports February 2012 INTRODUCTION 1. The Welsh Local Government Association (WLGA) represents the 22 local authorities in Wales, and the three national park authorities, the three fire and rescue authorities, and four police authorities are associate members. 2. It seeks to provide representation to local authorities within an emerging policy framework that satisfies the key priorities of our members and delivers a broad range of services that add value to Welsh Local Government and the communities they serve. 3. The WLGA welcomes this opportunity to feed comments into the NAfW‟s inquiry into international connectivity through Welsh ports and airports. Tables 1 and 2 below show that local authorities have a major interest in this issue with ten authorities having an airport/aircraft facility in their area and eight having a port – six have both. Overall, twelve authorities have an airport and/or a port – all of varying degrees of scale and activity. (In addition there are a number of former ports that have ceased to operate on a large scale but now house other activities including fishing and tourism related activity). Table 1 Airports in Wales Local authority Airport name Location Usage area Welshpool airport Welshpool Powys Public RAF Saint Athan St Athan Vale of Glamorgan Military Haverfordwest /Withybush Rudbaxton Pembrokeshire Public Aerodrome Cardiff Airport Rhoose Vale of Glamorgan Public Swansea Airport Pennard Swansea Public Pembrey airport Pembrey Carmarthenshire -

Offshore Rt Examiners
Air Ground Communication Service (AGCS) Examiners Safety and Airspace Regulation Group Airspace, ATM and Aerodromes List of CAA Authorised Examiners – Air Ground Communication Service (AGCS) CAA AGCS Operator’s Certificate of Competence Updated on: 06/07/2016 The information contained in this list has been supplied by the CAA Authorised Examiners. Any queries or amendments should be directed by e mail to [email protected] www.caa.co.uk Air Ground Communication Service (AGCS) Examiners This list will be updated and the latest version may be found on the CAA Website at http://www.caa.co.uk/WorkArea/DownloadAsset.aspx?id=4294975810 ABERDEEN ABERDEEN ABERDEEN Mr S Jeffrey Mr. N O R Johns Mr A Kinnear 33 The Rowans 'Eilean Donan' 9 Newburgh Crescent Insch Crichneyled Road Bridge of Don ABERDEEN St Katherines Aberdeen Aberdeenshire INVERURIE Aberdeenshire AB52 6ZD Aberdeenshire AB22 8ST Scotland AB51 8SN Scotland 01224 704551 01464821425 07703 706788 01651 891812 [email protected] ARGYLL Mr B Millar SAFISO Oban Airport North Connel Oban Argyll PA37 1SW Tel 01631 572910 [email protected] BELFAST BERKSHIRE BOURNEMOUTH Mr J Phelan Mr N A Popkin Ms E McKenzie Spectrum Aviation c/o West London Aero Club Director – ATM Training School Belfast Flying Club White Waltham Airfield Peregrine Academy Ltd Belfast International Airport MAIDENHEAD 8 St Stephens Court BELFAST Berkshire St Stephens Road County Antrim SL6 3NJ Bournemouth BT29 4AB England Dorset Northern Ireland BH2 6LA 01628 823272 02894 452153 07798 787024 -

LIST of REFERENCES ITW GSE 400 Hz Gpus AIRPORTS
Page 1 of 15 January 2017 LIST OF REFERENCES ITW GSE 400 Hz GPUs AIRPORTS Alger Airport Algeria 2005 Zvartnots Airport Armenia 2007 Brisbane Airport Australia 2013 Melbourne Airport Australia 2011-14 Perth Airport Australia 2011-12-13 Klagenfurt Airport Austria 1993 Vienna International Airport Austria 1995-2001-14-15 Bahrain International Airport Bahrain 2010-12 Minsk Airport Belarus 2014 Brussels International Airport Belgium 2001-02-08-15-16 Charleroi Airport Belgium 2006 Sofia Airport Bulgaria 2005 Air Burkina Burkina Faso 2004 Punta Arenas Chile 2001 Santiago Airport Chile 2011 Pointe Noitre Airport Congo Brazzaville 2009-10 Dubrovnik Airport Croatia 2014-16 La Habana Airport Cuba 2010 Larnaca Airport Cyprus 2008 Ostrava Airport Czech Republic 2010 Prague Airport Czech Republic 1996-97-2002-04-05-07-12-14-16 Aalborg Airport Denmark 1997-98-99-2012-15 Billund Airport Denmark 1999-2000-02-08-12-13-16 Copenhagen Airports Authorities Denmark 89-93-99-2000-01-03-07-09-10-11-12-13-14-15-16 Esbjerg Airport Denmark 2007-08-14 Hans Christian Andersen Airport (Odense) Denmark 1991-95-2015 Roenne Airport Denmark 1993 Karup Airport Denmark 1997-2016 Curacao Airport Dutch Antilles 2007 Cairo Intl. Airport Egypt 2015 Tallinn Airport Estonia 2004-05-14 Aéroport de Malabo Equatorial Guinea 2012 Vága Floghavn Faroe Islands 2015 Helsinki-Vantaa Airport Finland 1996-97-2000-05-06-09-10-13-14 Rovaniemi Airport Finland 2000 Turku Airport Finland 2014 Aéroport d’Aiglemont for Prince Aga Khan France 20007 Aéroport de Biarritz France 2009 Aéroport de Brest -
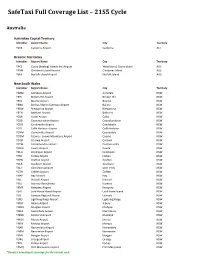
Safetaxi Full Coverage List – 21S5 Cycle
SafeTaxi Full Coverage List – 21S5 Cycle Australia Australian Capital Territory Identifier Airport Name City Territory YSCB Canberra Airport Canberra ACT Oceanic Territories Identifier Airport Name City Territory YPCC Cocos (Keeling) Islands Intl Airport West Island, Cocos Island AUS YPXM Christmas Island Airport Christmas Island AUS YSNF Norfolk Island Airport Norfolk Island AUS New South Wales Identifier Airport Name City Territory YARM Armidale Airport Armidale NSW YBHI Broken Hill Airport Broken Hill NSW YBKE Bourke Airport Bourke NSW YBNA Ballina / Byron Gateway Airport Ballina NSW YBRW Brewarrina Airport Brewarrina NSW YBTH Bathurst Airport Bathurst NSW YCBA Cobar Airport Cobar NSW YCBB Coonabarabran Airport Coonabarabran NSW YCDO Condobolin Airport Condobolin NSW YCFS Coffs Harbour Airport Coffs Harbour NSW YCNM Coonamble Airport Coonamble NSW YCOM Cooma - Snowy Mountains Airport Cooma NSW YCOR Corowa Airport Corowa NSW YCTM Cootamundra Airport Cootamundra NSW YCWR Cowra Airport Cowra NSW YDLQ Deniliquin Airport Deniliquin NSW YFBS Forbes Airport Forbes NSW YGFN Grafton Airport Grafton NSW YGLB Goulburn Airport Goulburn NSW YGLI Glen Innes Airport Glen Innes NSW YGTH Griffith Airport Griffith NSW YHAY Hay Airport Hay NSW YIVL Inverell Airport Inverell NSW YIVO Ivanhoe Aerodrome Ivanhoe NSW YKMP Kempsey Airport Kempsey NSW YLHI Lord Howe Island Airport Lord Howe Island NSW YLIS Lismore Regional Airport Lismore NSW YLRD Lightning Ridge Airport Lightning Ridge NSW YMAY Albury Airport Albury NSW YMDG Mudgee Airport Mudgee NSW YMER -

Executive Summary the General Aviation Awareness Council
The General Aviation Awareness Council President: The Lord Rotherwick Co-ordinating Office: Bicester Airfield Skimmingdish Lane Bicester Oxfordshire OX26 5HA e-mail: [email protected] Website: www.gaac.org.uk This paper responds to the question:- “Set out how you would identify a Network of Airfields of strategic significance to General Aviation so that these could be brought to the attention of the relevant authorities”. Executive Summary 1. There is no single essential network of airfields. The UK’s existing network effectively comprises a number of user based and often interdependent networks using airfields suitable for its activities. Each network has a hierarchy reflecting its user groups: the requirements of business aviation differ greatly from those of Gliders, which, in turn, differ from Microlights or balloons. 2. What we have is very largely what we need to maintain an effective GA network and support the commercial aviation industry. It has some capacity for expansion but there are concerns over whether it will be sufficient to meet the anticipated increase. 3. The UK already has an international reputation for excellence in aviation. We must continue to develop it or the industry will decline with the loss of jobs and profitable trade opportunities. 4. GA is the ‘grass roots’ for a combined contribution of £53 billion to UK plc. 5. Our Town planning system must be clear, consistent, and balanced. Planning Authorities need appropriate guidance to enable informed policy and decision making. 6. Legislative protection, similar to that for Railway Stations and other national infrastructure, would engender certainty and investor confidence to make the long term capital investment essential to the commercial viability of airfields. -

UK & Ireland HEMS & Air Ambulance Call Signs Summary
www.ukemergencyaviation.co.uk Last Updated: 17th August 2019 UK & Ireland HEMS & Air Ambulance Call Signs Summary Air Ambulance Operation Call Sign Based At Children’s Helimed 80 Oxford Airport Helimed 81 Doncaster Sheffield Airport Cornwall Helimed 01 Newquay Airport Derbyshire, Leicestershire & Rutland Helimed 54 East Midlands Airport Devon Helimed 70 Exeter Airport Helimed 71 Eaglescott Airfield Dorset & Somerset Helimed 10 Henstridge Airfield East Anglian Helimed 85 Norwich Airport Helimed 88 Cambridge Airport Essex & Herts Helimed 07 Earls Colne Airfield Helimed 55 North Weald Airfield Great North Helimed 58 Langwathby (Frank Bird) Helimed 63 Durham Tees Valley Airport Great Western Helimed 65 Almondsbury Hampshire & Isle of Wight Helimed 56 Thruxton Circuit Irish Air Corps Air Corps 112 Custume Barracks, Athlone Emergency Aeromedical Service Irish Community Rapid Response Helimed 92 Rathcoole Aerodrome, Co Cork Kent, Surrey & Sussex Helimed 21 Redhill Aerodrome Both a/c also have use of Rochester Airport FOB Helimed 60 Redhill Aerodrome Lincolnshire & Nottinghamshire Helimed 29 RAF Waddington London Helimed 27 Royal London Hospital Primary c/s Both a/c hangared RAF Northolt Magpas Helimed 66 RAF Wyton Midlands Helimed 03 RAF Cosford Helimed 06 Strensham M5 Services Northbound Helimed 09 Tatenhill Airfield North West Helimed 08 Blackpool Airport Helimed 72 Barton Aerodrome Helimed 75 Barton Aerodrome #1 www.ukemergencyaviation.co.uk Last Updated: 17th August 2019 Northern Ireland Helimed 23 Maze Long Kesh! Second offline a/c hangared Enniskillen -

Annual Safety Review 2018 Air Accidents Investigation Branch Annual Safety Review 2018 Aair Accidentsa Investigationib Branch
AAir AccidentsA InvestigationIB Branch Annual Safety Review 2018 Air Accidents Investigation Branch Annual Safety Review 2018 AAir AccidentsA InvestigationIB Branch © Crown Copyright 2019 All rights reserved. Copies of this publication may be reproduced for personal use, or for use within a company or organisation, but may not otherwise be reproduced for publication. Extracts may be published without specific permission providing that the source is duly acknowledged, the material is reproduced accurately and it is not used in a derogatory manner or in a misleading context. Published 18 April 2019 Enquiries regarding the content of this publication should be addressed to: Air Accidents Investigation Branch Farnborough House Berkshire Copse Road Aldershot Hampshire GU11 2HH. This document is also available in electronic (pdf) format at www.aaib.gov.uk Air Accidents Investigation Branch Annual Safety Review 2018 AAir AccidentsA InvestigationIB Branch Foreword Investigations The AAIB’s purpose is to improve aviation safety by determining the circumstances and causes of accidents and serious incidents, and promoting action to prevent reoccurrence. I am pleased to introduce the AAIB’s 2018 Foreword Annual Safety Review which includes information on our and Contents activity and the safety action taken or planned, by operators, manufacturers and the aviation authorities, in response to investigations concluded in 2018. The AAIB received 706 occurrence notifications in 2018 and opened 26 field investigations, 9 of which were into fatal accidents in the UK resulting in 16 deaths. A further 221 investigations were opened by correspondence. In addition, the AAIB appointed an accredited representative to 64 overseas investigations, including 23 involving UK registered aircraft. -

Noise Mapping Under the END Is Not Required for Airports in Wales
REGULATORY APPRAISAL ENVIRONMENTAL PROTECTION, WALES THE ENVIRONMENTAL NOISE (WALES) REGULATIONS 2006 Purpose and intended effect of the measure 1. These Regulations implement Directive 2002/49/EC of the European Parliament and of the Council of 25 June 2002, relating to the assessment and management of environmental noise (the Environmental Noise Directive (END)). In order to transpose the Directive Member States must designate the competent authorities and bodies responsible for implementing the Directive, including the authorities responsible for: • making and approving noise maps and action plans for large continuous urban areas (known as agglomerations), major roads, major railways and major airports; and • collecting noise maps and action plans for submission when required to the European Commission. 2. The proposed Regulations will give the National Assembly for Wales the responsibility of preparing, reviewing and revising noise maps under the END, except for maps applying to noise from non-designated major airports (all UK airports apart from Heathrow, Gatwick and Stanstead) where the airport operators will fulfil this role. In addition, the Regulations will give the National Assembly for Wales responsibility for drawing up, reviewing and revising action plans (except for plans applying to places near major airports, where the airport operators will fulfil this role). Currently, no airport in Wales meets the threshold for the preparation of a noise map or production of an action plan, as such noise mapping under the END is not required for airports in Wales. 3. As a result of implementing these Regulations, all legal responsibilities for the mapping and action planning under the END for roads, rail and agglomerations would rest with the National Assembly for Wales.