The A.M.A. and the Supply of Physicians* Rben A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Flexner Report ― 100 Years Later
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by PubMed Central YAlE JOuRNAl OF BiOlOGY AND MEDiCiNE 84 (2011), pp.269-276. Copyright © 2011. HiSTORiCAl PERSPECTivES iN MEDiCAl EDuCATiON The Flexner Report ― 100 Years Later Thomas P. Duffy, MD Yale School of Medicine, New Haven, Connecticut The Flexner Report of 1910 transformed the nature and process of medical education in America with a resulting elimination of proprietary schools and the establishment of the bio - medical model as the gold standard of medical training. This transformation occurred in the aftermath of the report, which embraced scientific knowledge and its advancement as the defining ethos of a modern physician. Such an orientation had its origins in the enchant - ment with German medical education that was spurred by the exposure of American edu - cators and physicians at the turn of the century to the university medical schools of Europe. American medicine profited immeasurably from the scientific advances that this system al - lowed, but the hyper-rational system of German science created an imbalance in the art and science of medicine. A catching-up is under way to realign the professional commit - ment of the physician with a revision of medical education to achieve that purpose. In the middle of the 17th century, an cathedrals resonated with Willis’s delin - extraordinary group of scientists and natu - eation of the structure and function of the ral philosophers coalesced as the Oxford brain [1]. Circle and created a scientific revolution in the study and understanding of the brain THE HOPKINS CIRCLE and consciousness. -

The Art of Thinking Clearly
For Sabine The Art of Thinking Clearly Rolf Dobelli www.sceptrebooks.co.uk First published in Great Britain in 2013 by Sceptre An imprint of Hodder & Stoughton An Hachette UK company 1 Copyright © Rolf Dobelli 2013 The right of Rolf Dobelli to be identified as the Author of the Work has been asserted by him in accordance with the Copyright, Designs and Patents Act 1988. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means without the prior written permission of the publisher, nor be otherwise circulated in any form of binding or cover other than that in which it is published and without a similar condition being imposed on the subsequent purchaser. A CIP catalogue record for this title is available from the British Library. eBook ISBN 978 1 444 75955 6 Hardback ISBN 978 1 444 75954 9 Hodder & Stoughton Ltd 338 Euston Road London NW1 3BH www.sceptrebooks.co.uk CONTENTS Introduction 1 WHY YOU SHOULD VISIT CEMETERIES: Survivorship Bias 2 DOES HARVARD MAKE YOU SMARTER?: Swimmer’s Body Illusion 3 WHY YOU SEE SHAPES IN THE CLOUDS: Clustering Illusion 4 IF 50 MILLION PEOPLE SAY SOMETHING FOOLISH, IT IS STILL FOOLISH: Social Proof 5 WHY YOU SHOULD FORGET THE PAST: Sunk Cost Fallacy 6 DON’T ACCEPT FREE DRINKS: Reciprocity 7 BEWARE THE ‘SPECIAL CASE’: Confirmation Bias (Part 1) 8 MURDER YOUR DARLINGS: Confirmation Bias (Part 2) 9 DON’T BOW TO AUTHORITY: Authority Bias 10 LEAVE YOUR SUPERMODEL FRIENDS AT HOME: Contrast Effect 11 WHY WE PREFER A WRONG MAP TO NO -

Legal and Medical Education Compared: Is It Time for a Flexner Report on Legal Education?
Washington University Law Review Volume 59 Issue 3 Legal Education January 1981 Legal and Medical Education Compared: Is It Time for a Flexner Report on Legal Education? Robert M. Hardaway University of Denver Follow this and additional works at: https://openscholarship.wustl.edu/law_lawreview Part of the Health Law and Policy Commons, and the Legal Education Commons Recommended Citation Robert M. Hardaway, Legal and Medical Education Compared: Is It Time for a Flexner Report on Legal Education?, 59 WASH. U. L. Q. 687 (1981). Available at: https://openscholarship.wustl.edu/law_lawreview/vol59/iss3/4 This Symposium is brought to you for free and open access by the Law School at Washington University Open Scholarship. It has been accepted for inclusion in Washington University Law Review by an authorized administrator of Washington University Open Scholarship. For more information, please contact [email protected]. LEGAL AND MEDICAL EDUCATION COMPARED: IS IT TIME FOR A FLEXNER REPORT ON LEGAL EDUCATION? ROBERT M. HARDAWAY* I. INTRODUCTION In 1907, medical education in the United States was faced with many of the problems' that critics feel are confronting legal education today:3 an over-production of practitioners, 2 high student-faculty ratios, proliferation of professional schools, insufficient financing,4 and inade- * Assistant Professor, University of Denver College of Law. B.A., 1966, Amherst College; J.D., 1971, New York University. The author wishes to acknowledge gratefully the assistance of Heather Stengel, a third year student at the University of Denver College of Law, in the prepara- tion of this article and the tabulation of statistical data. -

The Incentives to Preserve Digital Materials
The Incentives to Preserve Digital Materials: Roles, Scenarios, and Economic Decision-Making Brian F. Lavoie ([email protected]) Office of Research (http://www.oclc.org/research/) OCLC Online Computer Library Center, Inc. (http://www.oclc.org/) April 2003 Economic issues are a principal component of the research agenda for digital preservation. Economics is fundamentally about incentives, so a study of the economics of digital preservation should begin with an examination of the incentives to preserve. Securing the long-term viability and accessibility of digital materials requires an appropriate allocation of incentives among key decision-makers in the digital preservation process. But the circumstances under which digital preservation takes place often lead to a misalignment of preservation objectives and incentives. Identifying circumstances where insufficient incentives to preserve are likely to prevail, and how this can be remedied, are necessary first steps in developing economically sustainable digital preservation activities. http://www.oclc.org/research/projects/digipres/incentives-dp.pdf Copyright 2003 OCLC Online Computer Library Center, Inc. 6565 Frantz Road, Dublin, Ohio 43017-3395 USA http://www.oclc.org/ Reproduction of substantial portions of this publication must contain the OCLC copyright notice. Suggested citation: Lavoie, Brian F. (2003) The Incentives to Preserve Digital Materials: Roles, Scenarios, and Economic Decision-Making. White paper published electronically by OCLC Research. Available online at: http://www.oclc.org/research/projects/digipres/incentives-dp.pdf ACKNOWLEDGEMENTS The author has benefited from the insightful comments of a number of invited reviewers, including Meg Bellinger, Lorcan Dempsey, Clive Field, Dale Flecker, Clifford Lynch, Robert Martin, Ann Okerson, Edward O’Neill, Helen Shenton, Abby Smith, Hal Varian, and Deborah Woodyard. -

The Flexner Report: 100 Years Later
International Journal of Medical Education. 2010; 1:74-75 Letter ISSN: 2042-6372 DOI: 10.5116/ijme.4cb4.85c8 The Flexner report: 100 years later Douglas Page, Adrian Baranchuk Department of Cardiology, Kingston General Hospital, Queen’s University, Kingston, Ontario, Canada Correspondence: Adrian Baranchuk, Department of Cardiology, Kingston General Hospital, Queen’s University, Kingston, Canada, Email: [email protected] Accepted: October 12, 2010 One hundred years ago, medical education in the US and Following Flexner’s recommendations, accreditation Canada was very different than it is today. There was little programs and a shift in resources led to the closure of standardization regulating how medical education was many of the medical schools in existence at that time. delivered, and there was wide variation in the aptitude of Medical training became much more centralized, with practicing physicians. Though some medical education was smaller rural schools closing down as resources were delivered by the universities, many non-university affiliated concentrated in larger Universities that had better training schools still existed. Besides scientific medicine, homeo- facilities. Proprietary schools were terminated, and medi- pathic, osteopathic, chiropractic, botanical, eclectic, and cal education was delivered with the philosophy that basic physiomedical medicine were all taught and practiced by sciences and clinical experience were paramount to pro- different medical doctors at that time. In addition, there ducing effective physicians.2 -

Transcript And
TEXAS DEPARTMENT OF MOTOR VEHICLES BOARD MEETING Thursday, February 6, 2020 Lone Star Room Building 1 4000 Jackson Avenue Austin, Texas BOARD MEMBERS: Guillermo "Memo" Treviño, Chair Charles Bacarisse, Vice Chair Stacey Gillman Brett Graham Tammy McRae John Prewitt Joel Richardson Paul Scott Shelley Washburn ON THE RECORD REPORTING (512) 450-0342 2 I N D E X AGENDA ITEM PAGE 1. Roll Call and Establishment of Quorum 5 2. Pledges of Allegiance - U.S. and Texas 7 3. Chair's Reports A. Introduction of New Board Member - 8 Joel Richardson B. Chair's Annual Report to Governor on 9 State of Affairs 2019 4. Executive Director's Reports 10 Awards, Recognition of Years of Service, and Announcements 5. Memorandum of Understanding between Motor 12 Vehicle Crime Prevention Authority (MVCPA) and Texas Department of Motor Vehicles CONTESTED CASE 6. Reversed and Remanded from the Third Court of 16 Appeals to the Board for proceedings consistent with the appellate opinion (i.e. Reconsideration of the Board's August 17, 2017, Final Order) under Occupations Code, §§2301.467(a)(1), 2301.468, and 2301.478(b). Third Court of Appeals No. 03-17-00761-CV, Removed from the 201st District Court of Travis County, Cause No. D-1-GN-17-005912, SOAH Docket No. 608-14-1208.LIC, MVD Docket No. 14-0006 LIC; New World Car Nissan, Inc. d/b/a World Car Hyundai, World Car Nissan, and New World Car Imports, San Antonio, Inc., d/b/a World Car Hyundai, Complainants v. Hyundai Motor America, Respondent RULES - ADOPTIONS 7. Chapter 215, Motor Vehicle Distribution 106 Amendments, -

A Brief Guide to Osteopathic Medicine for Students, by Students
A Brief Guide to Osteopathic Medicine For Students, By Students By Patrick Wu, DO, MPH and Jonathan Siu, DO ® Second Edition Updated April 2015 Copyright © 2015 ® No part of this publication may be reproduced or transmitted in any form or by any means electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the publisher. American Association of Colleges of Osteopathic Medicine 5550 Friendship Boulevard, Suite 310 Chevy Chase, MD 20815-7231 Visit us on Facebook Please send any comments, questions, or errata to [email protected]. Cover Photos: Surgeons © astoria/fotolia; Students courtesy of A.T. Still University Back to Table of Contents Table of Contents Contents Dedication and Acknowledgements ................................................................................................................. ii Acknowledgements ............................................................................................................................................ ii Introduction ........................................................................................................................................................ 1 Myth or Fact?....................................................................................................................................................... 2 CHAPTER 1: What is a DO? .............................................................................................................................. -

Incentive Engineering for Collaborative Online Work: The
INCENTIVE ENGINEERING FOR COLLABORATIVE ONLINE WORK:THE CASE OF CROWDSOURCING Zur Erlangung des akademischen Grades eines Doktors der Wirtschaftswissenschaften (Dr. rer. pol.) von der Fakultät für Wirtschaftswissenschaften am Karlsruher Institut für Technologie (KIT) genehmigte DISSERTATION von M.Sc. Tim Jochen Straub Tag der mündlichen Prüfung: 15.03.2017 Referent: Prof. Dr. Christof Weinhardt Korreferent: Prof. Dr. Orestis Terzidis Karlsruhe, 2017 Contents List of Abbreviationsv List of Figures ix List of Tables xi I Introduction1 1 Introduction3 1.1 Motivation........................................ 3 1.2 Research Outline .................................... 6 1.3 Structure of the Thesis................................. 9 1.4 Research Development................................. 11 II Foundations and Related Work 15 2 Aspects of Collaborative Online Work 17 2.1 Crowdsourcing ..................................... 19 2.1.1 Classification of Crowdsourcing ...................... 22 2.1.2 Exemplary Crowdsourcing Platforms ................... 25 2.1.3 Related Concepts ............................... 27 2.2 Existing Work on Collaborative Online Work and Incentives.......... 29 3 The Theory of Motivation and Incentives 31 3.1 Definitions ........................................ 32 3.2 Motivation Theory ................................... 34 3.2.1 Content Theories ............................... 34 3.2.2 Process Theories................................ 36 3.2.3 Intrinsic and Extrinsic Motivation ..................... 37 III Insights from Collaborative -
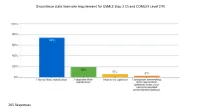
Discontinue State Licensure Requirement for USMLE Step 2 CS and COMLEX Level 2 PE
Discontinue state licensure requirement for USMLE Step 2 CS and COMLEX Level 2 PE 205 Responses Please indicate your view of this resolution as an ISMS priority. 202 Responses Survey Title: Resolution Survey Report Type: Verbatim Comments SR No. Response No. Response Text 1 5 Agree 2 7 Consider continued requirement for IMGs to complete USMLE Step 2 Clinical Skills for licensure in Illinois. 3 11 This is an undue burden on US medical students. 4 12 We need some standards for the graduating and new doctors! 5 15 Cost savings for new grads. no loss of competency 6 18 so what happens to the graduates of schools outside the US? so they still take the exam. are we setting up differential qualifications for licensure by stating that this test is not required of US graduates of allopathic and osteopathic schools? 7 83 Need to know the pros and c 8 27 I agree 9 35 The best reflection as to how a student is test results. I am concerned you would lose all ways to judge. 10 38 Strongly support. We pay so much for medical school and are subsequently nickeled and dimed for USMLE exams as well. There are many issues at stake here but do not overlook the financial burden of CS. 11 40 If this issue has been studied by the AMA and if they have come to the conclusion after study that these exams should be stopped, then I agree with the resolution. 12 45 Make perfect sense, making one wonder why such a modification wasn't enacted a generation or two ago. -
SCCCD New Employee Handbook Spring 2021
SCCCD New Employee Handbook Spring 2021 STATE CENTER COMMUNITY COLLEGE DISTRICT Fresno City College | Reedley College | Clovis Community College Madera Community College Center | Oakhurst Community College Center New Employee Handbook 1 | Page SCCCD New Employee Handbook Spring 2021 Section 1 – Welcome and Overview Learning Objectives Understand the mission, vision and values of the Community College system. Understand the structure of the Community College system. Understand the mission, vision and values of State Center Community College District. Understand the organizational structure of State Center Community College District. Understand or know where to access information needed to be successful in your position within State Center Community College District. California Community Colleges Chancellors Office Mission The mission of the California Community Colleges Board of Governors and the state Chancellor’s Office is to empower the community colleges through leadership, advocacy and support. Vision The California Community Colleges Board of Governors and the Chancellor share a vision of a better future for Californians by exemplifying exceptional leadership, advocacy and support on behalf of the community colleges. Their guidance provides access to lifelong learning for all citizens and creates a skilled, progressive workforce to advance the state’s interests. California Community Colleges Chancellor’s Office 1102 Q Street, Suite 4554 Sacramento, CA 95811 (916) 445-8752 Website: http://www.cccco.edu/ About Chancellor Eloy Ortiz Oakley The California Community Colleges Board of Governors appointed Eloy Ortiz Oakley as chancellor for the California Community Colleges beginning December 19, 2016. Eloy Ortiz Oakley is best known throughout California and the nation for implementing innovative programs and policies that help students succeed in college. -

Pay to Play: the Future of Clinical Clerkships?
Pay to Play: The Future of Clinical Clerkships? Mary Ann Forciea MD Clinical Professor of Medicine May 25, 2016 Brief History of Medical Education in the United States • 19th Century Models of Medical Training: – Apprenticeship: students worked with a practicing physician – Proprietary schools: students attended courses given by physicians who owned the college – University : clinical and didactic training at a University affiliated school In what year did African American medical students have the LEAST ACCESS TO TRAINING? • A 1895 • B 1925 • C 2000 19th Century Models • Problems: – No admission standards – No length of training standards • No equipment or laboratory standards – No curricular standards – No financing uniformity • Benefits – Diverse training possibilities – Wide ranging content available Meanwhile, at the University of Pennsylvania….. • Who was the first Dean of the College of Medicine? – Benjamin Rush – Benjamin Franklin – John Morgan – Ichabod Wright The School of Medicine created a Paradigm Shift (in the 1870s) by: • Paying faculty to teach courses • Integrating community service into the curriculum • Building its own teaching hospital • Accepting women Medical Education at University of Pennsylvania • Medical School created at the ‘College of Pennsylvania’ in 1765 – Creating the ‘University of Pennsylvania” • John Morgan the first Dean • Medical faculty distinct from College Faculty – Clinical work at Pennsylvania Hospital (1751) • West Philadelphia campus move 1870s – HUP the first teaching hospital built FOR the -

Allopathic and Osteopathic Medicine Unify GME Accreditation: a Historic Convergence Abdul-Kareem H
SPECIAL ARTICLES Allopathic and Osteopathic Medicine Unify GME Accreditation: A Historic Convergence Abdul-Kareem H. Ahmed, SM; Peter F. Schnatz, DO, NCMP; Eli Y. Adashi, MD, MS BACKGROUND AND OBJECTIVES: In 1968, the American Medical As- this latest development redefines sociation resolved to accept qualified graduates of osteopathic medical the allopathic-osteopathic interface schools into its accredited Graduate Medical Education (GME) programs. in a manner reminiscent of the his- An equally momentous decision was arrived at in 2014 when the Accredi- toric 1968 decision of the American tation Council for Graduate Medical Education (ACGME), the American Os- Medical Association (AMA) to accept teopathic Association (AOA), and the American Association of Colleges of qualified graduates of osteopathic Osteopathic Medicine (AACOM) resolved to institute a single unified GME medical schools into AMA-accredit- accreditation system by July 1, 2020. As envisioned, the unified accredi- ed GME programs.3 tation system will all but assure system-wide consistency of purpose and practice in anticipation of the Next Accreditation System (NAS) of the AC- Osteopathic Medicine GME. Governance integration replete with AOA and AACOM and osteopath- and the ACGME ic representation on the ACGME Board of Directors is now well underway. Central to this transition is the des- What is more, osteopathic representation on current Review Committees (RCs) and in a newly established one with an osteopathic focus has been ignation of the AOA and AACOM instituted. Viewed broadly, the unification of the GME accreditation system as member organizations of the goes a long way toward recognizing the overlapping characteristics in the ACGME and their representation training and practice of allopathic and osteopathic medicine.