The Pectoral-Sternalis Complex: an Unusual Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

Sternalis Muscle: a Mystery Still
Folia Morphol. Vol. 63, No. 2, pp. 147–149 Copyright © 2004 Via Medica R E V I E W A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Sternalis muscle: a mystery still Marios Loukas1,2, Maggi Bowers1, Joel Hullett1 1Department of Anatomy, American University of the Caribbean, Sint Maarten, Netherlands Antilles 2Harvard Medical School, Department of Education & Development, Boston, MA, USA [Received 8 October 2003; Accepted 29 November 2003] Despite intensive anatomical research during the last century, anatomical struc- tures or variations of these structures may still cause confusion or even iatrogenic injury. A matter of debate is the sternalis muscle. We present a review of the literature of the sternalis muscle with special emphasis on its clinical anatomy. Key words: sternalis muscle For such a seemingly insignificant member of the although Kida et al. [10] maintain that this argu- human musculature, the sternalis muscle has provid- ment is no longer valid. Nevertheless, the classifica- ed a wealth of uncertainty and debate. From its first tion of this not uncommon muscular variant is es- mention by Cabrolius in 1604 (reported by Turner) sential to complete the current annals of anatomi- [19], the sternalis has undergone examination after cal knowledge. examination with regard to such vital considerations This muscle is reported as having variable preva- as its origin, nerve supply, function, ethnic prevalence, lence in society as a whole, and is found anywhere and clinical significance. It has been called by various within the range of 3% to 6%, regardless of sex [3, authors musculus sternalis, presternalis, rectus ster- 6, 15, 17, 19, 20]. -

Pocket Atlas of Human Anatomy 4Th Edition
I Pocket Atlas of Human Anatomy 4th edition Feneis, Pocket Atlas of Human Anatomy © 2000 Thieme All rights reserved. Usage subject to terms and conditions of license. III Pocket Atlas of Human Anatomy Based on the International Nomenclature Heinz Feneis Wolfgang Dauber Professor Professor Formerly Institute of Anatomy Institute of Anatomy University of Tübingen University of Tübingen Tübingen, Germany Tübingen, Germany Fourth edition, fully revised 800 illustrations by Gerhard Spitzer Thieme Stuttgart · New York 2000 Feneis, Pocket Atlas of Human Anatomy © 2000 Thieme All rights reserved. Usage subject to terms and conditions of license. IV Library of Congress Cataloging-in-Publication Data is available from the publisher. 1st German edition 1967 2nd Japanese edition 1983 7th German edition 1993 2nd German edition 1970 1st Dutch edition 1984 2nd Dutch edition 1993 1st Italian edition 1970 2nd Swedish edition 1984 2nd Greek edition 1994 3rd German edition 1972 2nd English edition 1985 3rd English edition 1994 1st Polish edition 1973 2nd Polish edition 1986 3rd Spanish edition 1994 4th German edition 1974 1st French edition 1986 3rd Danish edition 1995 1st Spanish edition 1974 2nd Polish edition 1986 1st Russian edition 1996 1st Japanese edition 1974 6th German edition 1988 2nd Czech edition 1996 1st Portuguese edition 1976 2nd Italian edition 1989 3rd Swedish edition 1996 1st English edition 1976 2nd Spanish edition 1989 2nd Turkish edition 1997 1st Danish edition 1977 1st Turkish edition 1990 8th German edition 1998 1st Swedish edition 1979 1st Greek edition 1991 1st Indonesian edition 1998 1st Czech edition 1981 1st Chinese edition 1991 1st Basque edition 1998 5th German edition 1982 1st Icelandic edition 1992 3rd Dutch edtion 1999 2nd Danish edition 1983 3rd Polish edition 1992 4th Spanish edition 2000 This book is an authorized and revised translation of the 8th German edition published and copy- righted 1998 by Georg Thieme Verlag, Stuttgart, Germany. -

Bilateral Sternalis Muscles Were Observed During Dissection of the Thoraco-Abdominal Region of a Male Cadaver
Case Reports Ahmed F. Ibrahim, MSc, MD, Saeed A. Makarem, MSc. PhD, Hassem H. Darwish, MBBCh. ABSTRACT Bilateral sternalis muscles were observed during dissection of the thoraco-abdominal region of a male cadaver. A full description of the muscles, as well as their attachments and innervations were reported. A brief review of the existing literature, regarding the nomenclature, incidence, attachments, innervations and clinical relevance of the sternalis muscle, is also presented. Neurosciences 2005; Vol. 10 (2): 171-173 he importance of continuing to record and Case Report. A well defined sternalis muscle Tdiscuss anatomical anomalies was addressed (Figures 1 & 2) was found, bilaterally, during recently1 in light of technical advances and dissection of the thoraco-abdominal region of a interventional methods of diagnosis and treatment. male cadaver in the Department of Anatomy, The sternalis muscle is a small supernumerary College of Medicine, King Saud University, Riyadh, muscle located in the anterior thoracic region, Kingdom of Saudi Arabia. Both muscles were superficial to the sternum and the sternocostal covered by superficial fascia, located superficial to fascicles of the pectoralis major muscle.2 In the the corresponding sternocostal portion of pectoralis literature, sternalis muscle is called "a normal major and separated from it by pectoral fascia. The anatomic variant"3 and "a well-known variation",4 left sternalis was 19 cm long and 3 cm wide at its although in most textbooks of anatomy, it is broadest part. Its upper end formed a tendon insufficiently mentioned. Yet, clinicians are continuous with that of the sternal head of left surprisingly unaware of this common variation. -

Contents VII
Contents VII Contents Preface .............................. V 3.2 Supply of the Connective Tissue ....... 28 List of Abbreviations ................... VI Diffusion ......................... 28 Picture Credits ........................ VI Osmosis .......................... 29 3.3 The “Creep” Phenomenon ............ 29 3.4 The Muscle ....................... 29 Part A Muscle Chains 3.5 The Fasciae ....................... 30 Philipp Richter Functions of the Fasciae .............. 30 Manifestations of Fascial Disorders ...... 30 Evaluation of Fascial Tensions .......... 31 1 Introduction ..................... 2 Causes of Musculoskeletal Dysfunctions .. 31 1.1 The Significance of Muscle Chains Genesis of Myofascial Disorders ........ 31 in the Organism ................... 2 Patterns of Pain .................... 32 1.2 The Osteopathy of Dr. Still ........... 2 3.6 Vegetative Innervation of the Organs ... 34 1.3 Scientific Evidence ................. 4 3.7 Irvin M. Korr ...................... 34 1.4 Mobility and Stability ............... 5 Significance of a Somatic Dysfunction in the Spinal Column for the Entire Organism ... 34 1.5 The Organism as a Unit .............. 6 Significance of the Spinal Cord ......... 35 1.6 Interrelation of Structure and Function .. 7 Significance of the Autonomous Nervous 1.7 Biomechanics of the Spinal Column and System .......................... 35 the Locomotor System .............. 7 Significance of the Nerves for Trophism .. 35 .............. 1.8 The Significance of Homeostasis ....... 8 3.8 Sir Charles Sherrington 36 Inhibition of the Antagonist or Reciprocal 1.9 The Nervous System as Control Center .. 8 Innervation (or Inhibition) ............ 36 1.10 Different Models of Muscle Chains ..... 8 Post-isometric Relaxation ............. 36 1.11 In This Book ...................... 9 Temporary Summation and Local, Spatial Summation .................. 36 Successive Induction ................ 36 ......... 2ModelsofMyofascialChains 10 3.9 Harrison H. Fryette ................. 37 2.1 Herman Kabat 1950: Lovett’s Laws ..................... -

The Laminated Nature of the Pectoralis Major Muscle and the Redefinition of the Inframammary Fold Clinical Implications in Aesthetic and Reconstructive Breast Surgery
The Laminated Nature of the Pectoralis Major Muscle and the Redefinition of the Inframammary Fold Clinical Implications in Aesthetic and Reconstructive Breast Surgery Melvin M. Maclin II, MDa,*, Olivier A. Deigni, MD, MPHb, Bradley P. Bengtson, MDc KEYWORDS Pectoralis major muscle Inframammary fold Subpectoral augmentation Breast augmentation Breast reconstruction Acellular dermal matrix Breast inflection points Chest wall anatomy KEY POINTS The inframammary fold (IMF) is a critical landmark and aesthetic structure in breast surgery, yet it is poorly understood. The skin envelope is considered a separate entity from the chest wall; however, its surgical manip- ulation is not independent of chest wall anatomy. The pectoralis major muscle is a key structure in both cosmetic and reconstructive surgery, and its structure and performance are related to its inferior costal origins. A better understanding of the relationship of the IMF, pectoralis, and chest wall anatomy can offer improved outcomes in breast surgery. INTRODUCTION intimately aware of its relationship to the chest The breast is appreciated aesthetically and clini- wall and the breast soft tissues. Both are able to cally for its shape, projection, and volume. Multiple achieve outstanding outcomes; however, the au- techniques have evolved over the years to modify, thors present an alternative appreciation of the enhance, or recreate the breast mound. To this pectoralis and its relationship to the breast. The end surgical techniques have evolved to manipu- authors liken the comparison to the tale retold by late the breast skin envelope, soft tissues, and John Saxe of the 6 blind wise men and the chest wall anatomy, with and without prosthetic elephant (Fig. -
Bilateral Rectus Sternalis Muscle: an Anatomical Variant of Anterior Chest Wall
International Journal of Science and Research (IJSR) ISSN: 2319-7064 ResearchGate Impact Factor (2018): 0.28 | SJIF (2018): 7.426 Bilateral Rectus Sternalis Muscle: An Anatomical Variant of Anterior Chest Wall Dr. Aparna Vedapriya .K1, Dr. Dasarapu Priyanka2 1Associate Professor and HOD, Department of Anatomy, Osmania Medical College, Koti, Hyderabad, Telangana State, India 2Second year Post Graduate, Department of Anatomy, Osmania Medical College, Koti, Hyderabad, Telangana State, India Abstract: Introduction: Rectus Sternalis muscle, an uncommon anatomical variant of the chest wall musculature located in the anterior thoracic wall, superficial and perpendicular to the pectoralis major and parallel to the sternum. It is regularly present in lower animals and is occasionally detected in humans. A Cadaveric study which was done and the details of this muscle has been presented to establish the importance of Rectus Sternalis. Methods: The study was undertaken on 22 embalmed adult human cadavers irrespective of age and sex used for undergraduate dissection from the Department of Anatomy, Osmania Medical College over a period of 2 years. In this present study, in an elderly male cadaver, a normal anatomical variant of anterior chest wall musculature was found. Photographs and details of this muscle were taken after cleaning the dissected region. Results: In the present study, three slips of rectus sternalis was seen on either side of sternum in anterior chest wall, which were bifurcating below and blending with external oblique aponeurosis, above into the pectoral fascia superficial to pectoralis major muscle. Conclusion: Rectus Sternalis is a rare but a normal anatomical variant in the anterior chest wall musculature and knowledge on it is important, for interventional and diagnostic procedures which are related to this region Keywords: Pectoralis major (PM), Rectus sternalis (RS) 1. -

Pectoral Region and Axilla Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Pectoral Region and Axilla Doctors Notes Notes/Extra explanation Editing File Objectives By the end of the lecture the students should be able to : Identify and describe the muscles of the pectoral region. I. Pectoralis major. II. Pectoralis minor. III. Subclavius. IV. Serratus anterior. Describe and demonstrate the boundaries and contents of the axilla. Describe the formation of the brachial plexus and its branches. The movements of the upper limb Note: differentiate between the different regions Flexion & extension of Flexion & extension of Flexion & extension of wrist = hand elbow = forearm shoulder = arm = humerus I. Pectoralis Major Origin 2 heads Clavicular head: From Medial ½ of the front of the clavicle. Sternocostal head: From; Sternum. Upper 6 costal cartilages. Aponeurosis of the external oblique muscle. Insertion Lateral lip of bicipital groove (humerus)* Costal cartilage (hyaline Nerve Supply Medial & lateral pectoral nerves. cartilage that connects the ribs to the sternum) Action Adduction and medial rotation of the arm. Recall what we took in foundation: Only the clavicular head helps in flexion of arm Muscles are attached to bones / (shoulder). ligaments / cartilage by 1) tendons * 3 muscles are attached at the bicipital groove: 2) aponeurosis Latissimus dorsi, pectoral major, teres major 3) raphe Extra Extra picture for understanding II. Pectoralis Minor Origin From 3rd ,4th, & 5th ribs close to their costal cartilages. Insertion Coracoid process (scapula)* 3 Nerve Supply Medial pectoral nerve. 4 Action 1. Depression of the shoulder. 5 2. Draw the ribs upward and outwards during deep inspiration. *Don’t confuse the coracoid process on the scapula with the coronoid process on the ulna Extra III. -
Muscles of Mastication Muscles That Move the Head
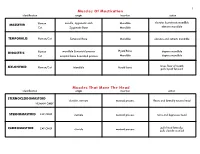
1 Muscles Of Mastication identification origin insertion action maxilla, zygomatic arch Mandible elevates & protracts mandible MASSETER Human Cat Zygomatic Bone Mandible elevates mandible TEMPORALIS Human/Cat Temporal Bone Mandible elevates and retracts mandible Hyoid Bone DIGASTRIC Human mandible & mastoid process depress mandible Cat occipital bone & mastoid process Mandible depress mandible raises floor of mouth; MYLOHYOID Human/Cat Mandible Hyoid bone pulls hyoid forward Muscles That Move The Head identification origin insertion action STERNOCLEIDOMAStoID clavicle, sternum mastoid process flexes and laterally rotates head HUMAN ONLY STERNOMAStoID CAT ONLY sternum mastoid process turns and depresses head pulls head laterally; CLEIDOMAStoID CAT ONLY clavicle mastoid process pulls clavicle craniad 2 Muscles Of The Hyoid, Larynx And Tongue identification origin insertion action Human Sternum Hyoid depresses hyoid bone STERNOHYOID Cat costal cartilage 1st rib Hyoid pulls hyoid caudally; raises ribs and sternum sternum Throid cartilage of larynx Human depresses thyroid cartilage STERNothYROID Cat costal cartilage 1st rib Throid cartilage of larynx pulls larynx caudad elevates thyroid cartilage and Human thyroid cartilage of larynx Hyoid THYROHYOID depresses hyoid bone Cat thyroid cartilage of larynx Hyoid raises larynx GENIOHYOID Human/Cat Mandible Hyoid pulls hyoid craniad 3 Muscles That Attach Pectoral Appendages To Vertebral Column identification origin insertion action Human Occipital bone; Thoracic and Cervical raises clavicle; adducts, -

A Mystery Muscle
Research Article Musculus sternalis : a mystery muscle Vaibhav Vasudevrao Phad 1* , S. A. Syed 2, R. A. Joshi 3, N. G. Herekar 4 1Assistant Professor, 2Assistant Professor, 4Professor and HOD, Department of Anatomy, Government Medical College, Miraj, District Sangli 416410, Maharashtra, INDIA. 3Professor and HOD, Department of Anatomy, RCSM Government Medical College, Kolhapur, Maharashtra, INDIA. Email: [email protected] Abstract Introduction: Rectus column gives rise to various muscles extending from pubic symphysis to symphysis menti. These are well developed in neck region represented by supra -hyoid and infra-hyoid muscles, in abdominal region represented by rectus abdominis. In thorax this l ayer usually disappears but occasionally remains as musculus sternalis. During study we dissected 12 cadavers and encountered a musculus sternalis on right side of 60 -year-old male cadaver covered by superficial fascia and located anterior to the pectorali s major muscle. Knowledge regarding the muscular variations of the anterior wall of chest and their identification is important for radiological examinations such as mammography. The existence of the musculus sternalis should not be overlooked in the surgi cal and diagnostic procedures. Keywords: Pubic symphysis, symphysis menti, supra -hyoid, musculus sternalis. *Address for Correspondence: Dr Vaibhav Vasudevrao Phad, Assistant Professor, Department of Anatomy, Government Medical College, Miraj- 416410 Dist Sangali, Maharashtra, INDIA. Email: [email protected] Received Date: 14/07/2014 Accepted Date: 28 /07 /2014 musculus sternalis, presternalis, rectus sternalis, sternalis Access this article online brutorum, or thoracicus , sternalis, the episternalis, the Quick Response Code: rectus thoracis, the superficial rectus abdominis..... and 3 Website: so many names. During the dissection of 12 cadavers we www.statperson.com have found presence of one unilateral musculus sternalis. -

Congenital Absence of the Pectoral Muscles
Arch Dis Child: first published as 10.1136/adc.12.68.123 on 1 April 1937. Downloaded from CONGENITAL ABSENCE OF THE PECTORAL MUSCLES BY E. D. IRVINE, M.D., AND J. B. TILLEY, M.D. (Blackburn). The four patients described in this paper exhibit congenital absence of the pectoral muscles in varying degree, and illustrate many points of interest. Three of them were observed during routine and special medical examinations of approximately 15,000 elementary school children, and one was a pre-school child in hospital: it is interesting to note that Scheslinger, according to Rector', discovered five cases in 54,000 patients. Case 1 was discovered during the examination of a boy aged ten, the second of four children, who complained of cough: he is under observation http://adc.bmj.com/ on September 30, 2021 by guest. Protected copyright. FIG. 1. as a tuberculosis contact. The sterno-costal portion of the left pectoralis major and the left pectoralis minor are both missing. Although not previously noted, this is believed to be a congenital defect. The clavicular head of the pectoralis major is well developed and arises from the inner half of the clavicle; the deltoid is not hypertrophied (fig. 1). When the arms are extended above the head, a well-marked fold of skin running vertically across the axilla to the second left rib and interspace can be seen and in Arch Dis Child: first published as 10.1136/adc.12.68.123 on 1 April 1937. Downloaded from I 2d4 AIICIlIVES 0O' DISEASE IN CHILDHOOD the fold fibrous tissue can be felt deep to the skin: whether this is simply fascia or a vestigial or degenerated muscle is not known. -

VARIATION in PECTORALIS MAJOR MUSCLE FOUND DURING DISSECTION- a CASE REPORT 1Dr
Case Report International Ayurvedic Medical Journal ISSN:2320 5091 VARIATION IN PECTORALIS MAJOR MUSCLE FOUND DURING DISSECTION- A CASE REPORT 1Dr. Chhaya Gupta 2Dr. J. Manohar 3Dr. Sandeep M. Lahange 1MD scholar, Dept. of Sharira Rachana, NIA, Jaipur, Rajasthan, India 2Assistant Professor, Dept. Of Sharira Rachana, NIA, Jaipur, Rajasthan, India 3Assistant Professor, Dept. Of Sharira Rachana, NIA, Jaipur, Rajasthan, India ABSTRACT The pectoral region covers the anterior thoracic wall and part of the lateral thoracic wall. There are four muscles in the pectoral region: pectoralis major, pectoralis minor, subclavius and ser- ratus anterior. The muscles of the pectoral region attach the upper limb to the axial skeleton. The pectoralis major muscle is positioned immediately deep to the superficial fascia. The pecto- ralis major muscle comprises two heads 1) Clavicular head 2) Sternocostal head. It originates from the clavicle, manubrium, sternum, costal cartilage, aponeurosis of external oblique muscle of abdomen and inserted on humerus. The present case is a report of an unusual variation of pectoralis major muscle in pectoral region. Key words: - Clavicular, pectoral, sternocostal. INTRODUCTION lage, the first to the seven costal cartilages, The pectoral word is originated the sternal end of the sixth rib and the apo- from the latin word ‘pectus’ means chest, neurosis of external oblique. Slight cleft which is found on the exterior of anterior separates the clavicular fibres from the thoracic wall and on the region of the lat- sternal fibres. The muscle tends to become eral thoracic wall1 . Generally, the region a flat tendon, approximately 5 cm across. covering both the walls is termed as the The tendon is bilaminar.