Item Master CPT Code Charge 6090610 COMPREHENSIVE
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of New Drugs Approved in India from 1991 to 2000
LIST OF NEW DRUGS APPROVED IN INDIA FROM 1991 TO 2000 S. No Name of Drug Pharmacological action/ Date of Indication Approval 1 Ciprofloxacin 0.3% w/v Eye Indicated in the treatment of February-1991 Drops/Eye Ointment/Ear Drop external ocular infection of the eye. 2 Diclofenac Sodium 1gm Gel March-1991 3 i)Cefaclor Monohydrate Antibiotic- In respiratory April-1991 250mg/500mg Capsule. infections, ENT infection, UT ii)Cefaclor Monohydrate infections, Skin and skin 125mg/5ml & 250mg/5ml structure infections. Suspension. iii)Cefaclor Monohydrate 100mg/ml Drops. iv)Cefaclor 187mg/5ml Suspension (For paediatric use). 4 Sheep Pox Vaccine (For April-1991 Veterinary) 5 Omeprazole 10mg/20mg Short term treatment of April-1991 Enteric Coated Granules duodenal ulcer, gastric ulcer, Capsule reflux oesophagitis, management of Zollinger- Ellison syndrome. 6 i)Nefopam Hydrochloride Non narcotic analgesic- Acute April-1991 30mg Tablet. and chronic pain, including ii)Nefopam Hydrochloride post-operative pain, dental 20mg/ml Injection. pain, musculo-skeletal pain, acute traumatic pain and cancer pain. 7 Buparvaquone 5% w/v Indicated in the treatment of April-1991 Solution for Injection (For bovine theileriosis. Veterinary) 8 i)Kitotifen Fumerate 1mg Anti asthmatic drug- Indicated May-1991 Tablet in prophylactic treatment of ii)Kitotifen Fumerate Syrup bronchial asthma, symptomatic iii)Ketotifen Fumerate Nasal improvement of allergic Drops conditions including rhinitis and conjunctivitis. 9 i)Pefloxacin Mesylate Antibacterial- In the treatment May-1991 Dihydrate 400mg Film Coated of severe infection in adults Tablet caused by sensitive ii)Pefloxacin Mesylate microorganism (gram -ve Dihydrate 400mg/5ml Injection pathogens and staphylococci). iii)Pefloxacin Mesylate Dihydrate 400mg I.V Bottles of 100ml/200ml 10 Ofloxacin 100mg/50ml & Indicated in RTI, UTI, May-1991 200mg/100ml vial Infusion gynaecological infection, skin/soft lesion infection. -

(12) United States Patent (10) Patent No.: US 7,074,961 B2 Wang Et Al
US007074961B2 (12) United States Patent (10) Patent No.: US 7,074,961 B2 Wang et al. (45) Date of Patent: Jul. 11, 2006 (54) ANTIDEPRESSANTS AND THEIR 6.211,171 B1 4/2001 Sawynok et al. ANALOGUES AS LONG-ACTING LOCAL 6,545,057 B1 4/2003 Wang et al. ANESTHETCS AND ANALGESCS 2001/0036943 A1 11/2001 Coe et al. (75) Inventors: Ging Kuo Wang, Westwood, MA (US); FOREIGN PATENT DOCUMENTS Peter Gerner, Weston, MA (US); Donald K. Verrecchia, Winchester, MA CH 534124 A 2, 1973 (US) WO WO95/17903 A1 7, 1995 WO WO95/1818.6 A1 7, 1995 (73) Assignee: The Brigham and Women's Hospital, WO WO 99.59.598 A1 11, 1999 Inc., Boston, MA (US) WO WO O2/060870 A2 8, 2002 (*) Notice: Subject to any disclaimer, the term of this OTHER PUBLICATIONS patent is extended or adjusted under 35 U.S.C. 154(b) by 451 days. Luo et al., Xenobiotica, vol. 25, No. 3, pp. 291-301, 1995.* (21) Appl. No.: 10/117,708 Ehlert et al., The Interaction of Amitriptyline, Doxepin, Imipramine and Their N-Methyl Quaternary Ammonium (22) Filed: Apr. 4, 2002 Derivatives with Subtypes of Muscarinic Receptors in Brain (65) Prior Publication Data and Heart, The Journal of Pharmacology and Experimental Therapeutics, Apr. 1990, vol. 253, No. 1, pp. 13–19. US 2003/00968.05 A1 May 22, 2003 Gerner, P., et al., Anesthesiology (2002) 96:1435–42. Related U.S. Application Dat e pplication Uata Khan, M.A., et al., Anesthesiology (2002) 96:109–16. (63) stripps'965,138, filed on Sep. -
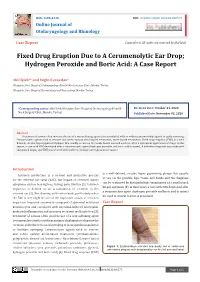
Fixed Drug Eruption Due to a Cerumenolytic Ear Drop; Hydrogen Peroxide and Boric Acid: a Case Report
ISSN: 2688-8238 DOI: 10.33552/OJOR.2020.04.000577 Online Journal of Otolaryngology and Rhinology Case Report Copyright © All rights are reserved by Akif İşlek Fixed Drug Eruption Due to A Cerumenolytic Ear Drop; Hydrogen Peroxide and Boric Acid: A Case Report Akif İşlek1* and Engin Karaaslan2 1Nusaybin State Hospital, Otolaryngology-Head & Neck Surgery Clinic, Mardin, Turkey 2Nusaybin State Hospital, Dermatology and Venereology, Mardin, Turkey *Corresponding author: Received Date: October 24, 2020 Published Date: November 03, 2020 Akif İşlek, Nusaybin State Hospital, Otolaryngology-Head & Neck Surgery Clinic, Mardin, Turkey. Abstract Treatment of earwax often involves the use of a wax softening agent (cerumenolytic) with or without antimicrobial agents to easily removing. Cerumenolytic agents used to remove and soften earwax areoil-based treatments, water-based treatments. Fixed drug eruption (FDE) is a well- defined, circular, hyperpigmented plaque that usually occurs on the trunk, hands mucosal surfaces, after a systemical application of drugs. In this report, a case with FDE developed after a cerumenolytic agent (hydrogen peroxide and boric acid in water). A definitive diagnosis was made with skin punch biopsy and FDE was treated with oral levocetirizine and topical mometasone. Introduction is a well-defined, circular, hyper pigmenting plaque that usually Cerumen production is a normal and protective process occurs on the genitals, lips, trunk, and hands and the diagnosis for the external ear canal (EAC), but impact of cerumen causes can be confirmed by histopathologic examination of a small punch symptoms such as hearing loss, itching, pain, tinnitus [1]. Cerumen biopsy specimen [5]. In this report, a case with FDE developed after impaction is defined as an accumulation of cerumen in the a cerumenolytic agent (hydrogen peroxide and boric acid in water) external ear [2]. -

Management of Specific Wounds
7 Management of Specific Wounds Bite Wounds 174 Hygroma 234 Burns 183 Snakebite 239 Inhalation Injuries 195 Brown Recluse Spider Bites 240 Chemical Burns 196 Porcupine Quills 240 Electrical Injuries 197 Lower Extremity Shearing Wounds 243 Radiation Injuries 201 Plate 10: Pipe Insulation Protective Frostbite 204 Device: Elbow 248 Projectile Injuries 205 Plate 11: Pipe Insulation to Protect Explosive Munitions: Ballistic, the Greater Trochanter 250 Blast, and Thermal Injuries 227 Plate 12: Vacuum Drain Impalement Injuries 227 Management of Elbow Pressure Ulcers 228 Hygromas 252 Atlas of Small Animal Wound Management and Reconstructive Surgery, Fourth Edition. Michael M. Pavletic. © 2018 John Wiley & Sons, Inc. Published 2018 by John Wiley & Sons, Inc. Companion website: www.wiley.com/go/pavletic/atlas 173 174 Atlas of Small Animal Wound Management and Reconstructive Surgery BITE WOUNDS to the skin. Wounds may be covered by a thick hair coat and go unrecognized. The skin and underlying Introduction issues can be lacerated, stretched, crushed, and avulsed. Circulatory compromise from the division of vessels and compromise to collateral vascular channels can result in Bite wounds are among the most serious injuries seen in massive tissue necrosis. It may take several days before small animal practice, and can account for 10–15% of all the severity of tissue loss becomes evident. All bites veterinary trauma cases. The canine teeth are designed are considered contaminated wounds: the presence of for tissue penetration, the incisors for grasping, and the bacteria in the face of vascular compromise can precipi- molars/premolars for shearing tissue. The curved canine tate massive infection. teeth of large dogs are capable of deep penetration, whereas the smaller, straighter canine teeth of domestic cats can penetrate directly into tissues, leaving a rela- tively small cutaneous hole. -

Reconstructive
RECONSTRUCTIVE Muscle versus Nonmuscle Flaps in the Reconstruction of Chronic Osteomyelitis Defects Christopher J. Salgado, Background: Surgical treatment of chronic osteomyelitis requires aggressive M.D. debridement followed by wound coverage and obliteration of dead space with Samir Mardini, M.D. vascularized tissue. Controversy remains as to the effectiveness of different tissue Amir A. Jamali, M.D. types in achieving these goals and in the eradication of disease. Juan Ortiz, M.D. Methods: Chronic osteomyelitis was induced in 26 goat tibias using Staphylo- Raoul Gonzales, D.V.M., coccus aureus as an infecting inoculum. In a single stage, debridement followed Ph.D. by reconstruction using either a muscle flap (n ϭ 13) or a fasciocutaneous flap Hung-Chi Chen, M.D. (n ϭ 13) was performed. Flap donor sites were closed primarily and antibiotics El Paso, Texas; Kaohsiung, Taiwan; were given for 5 days postoperatively. Daily clinical evaluation for 1 year was and Sacramento, Calif. performed and monthly radiographs were obtained for 9 months and 1 year after the reconstruction. Results: Twenty-five flaps survived completely, and one nonmuscle flap under- went partial flap loss following a period of venous congestion. There were no postoperative complications in the muscle flap group. Two goats (15 percent) in the nonmuscle group developed superficial wounds in the immediate post- operative period that resolved with conservative management. No limbs had recurrent osteomyelitis wounds at 1 year of clinical follow-up examination. Radiographic evidence of osteomyelitis was present in two goats (15 percent) in the muscle group and one goat (8 percent) in the nonmuscle group. -

(TECA) Surgery
Audit of Total Ear Canal Ablation-Lateral Bulla Osteotomy Procedures Performed by One Surgeon Audit project lead: D G Bentley Subject/area of practice: Surgery/Dermatology Date: January 2nd 2018 Reasons for Audit: To determine how complication rate of this procedure, both short and long term, compare with that in recently published literature and to be sure this procedure should be still be offered in-house rather than being referred to a surgical specialist. Background Total Ear Canal Ablation-Lateral Bulla Osteotomy (TECA-LBO) procedures on dogs (and cats) have been performed by this surgeon since 1991 and since that time over 260 procedures have been performed. The surgeon also runs a dermatology service with special interest in ear disease and wishes to provide a complete service whereby cases that are beyond medical treatment can go to surgery without being referred to a specialist surgeon. Indications for TECA-LBO are “end stage otitis”, where there is chronic irreversible change to the ear canal, intractable ear infections particularly as a result of middle ear infection and changes in the vicinity of the tympanic membrane/lower horizontal ear canal, and tumours in the ear canal which cannot be dealt with either by Lateral Wall Resection or Vertical Canal Ablation. Also sometimes, due to financial reasons, a client may prefer surgery to lengthy courses of treatment, requiring several anaesthetics and ear flushings, with no guarantee of success at the outset. The surgeon first learnt the technique that was published in video format in the “In Practice” series around 1991. This involved the use of an osteotome to separate the ear canal from the bulla and also looking for the facial nerve and pulling it out of the way using penrose drain material. -

Femoral and Sciatic Nerve Blocks for Total Knee Replacement in an Obese Patient with a Previous History of Failed Endotracheal Intubation −A Case Report−
Anesth Pain Med 2011; 6: 270~274 ■Case Report■ Femoral and sciatic nerve blocks for total knee replacement in an obese patient with a previous history of failed endotracheal intubation −A case report− Department of Anesthesiology and Pain Medicine, School of Medicine, Catholic University of Daegu, Daegu, Korea Jong Hae Kim, Woon Seok Roh, Jin Yong Jung, Seok Young Song, Jung Eun Kim, and Baek Jin Kim Peripheral nerve block has frequently been used as an alternative are situations in which spinal or epidural anesthesia cannot be to epidural analgesia for postoperative pain control in patients conducted, such as coagulation disturbances, sepsis, local undergoing total knee replacement. However, there are few reports infection, immune deficiency, severe spinal deformity, severe demonstrating that the combination of femoral and sciatic nerve blocks (FSNBs) can provide adequate analgesia and muscle decompensated hypovolemia and shock. Moreover, factors relaxation during total knee replacement. We experienced a case associated with technically difficult neuraxial blocks influence of successful FSNBs for a total knee replacement in a 66 year-old the anesthesiologist’s decision to perform the procedure [1]. In female patient who had a previous cancelled surgery due to a failed tracheal intubation followed by a difficult mask ventilation for 50 these cases, peripheral nerve block can provide a good solution minutes, 3 days before these blocks. FSNBs were performed with for operations on a lower extremity. The combination of 50 ml of 1.5% mepivacaine because she had conditions precluding femoral and sciatic nerve blocks (FSNBs) has frequently been neuraxial blocks including a long distance from the skin to the used for postoperative pain control after total knee replacement epidural space related to a high body mass index and nonpalpable lumbar spinous processes. -

Over-The-Counter (OTC) Medications Applies To: Tufts Health Ritogether and Tufts Health Together*
Over-the-Counter (OTC) Medications Applies to: Tufts Health RITogether and Tufts Health Together* As communicated in the November 1, 2018 Provider Update, the following changes are effective for fill dates on or after January 1, 2019. As a result of this change, some OTC medications will require prior authorization in certain circumstances as outlined below: Brand-Name OTC Medication Has a Covered Interchangeable Generic Version Available Afrin No Drip Advil capsule Advil tablet Advil PM tablet Afrin Nasal Spray Original nasal solution Afrin No Drip Aveeno Oatmeal Severe nasal Aleve tablet Baciguent ointment Benadryl capsule Bath Pak Treatment solution Benadryl Allergy Benadryl Allergy Benadryl Allergy Benadryl Extra Benefiber powder tablet capsule Liquid Strength cream Caltrate 600 +D Centrum Silver Betadine Swabstick Caltrate + D tablet Centrum liquid Plus Minerals tablet tablet Centrum Silver Centrum Ultra Men’s Children’s Advil Centrum tablet Cheracol-D syrup Adult 50+ tablet tablet suspension Children’s Benadryl Citracal Calcium + Children’s Benadryl Children’s Tylenol Chlor-Trimeton Allergy chewable D Slow Release Allergy liquid suspension syrup tablet tablet Citrucel Fiber Claritin-D 12 hour Claritin-D 24 hour Clear Cough Liquid Citrucel tablet Laxative powder tablet tablet PM Dimetapp DM Dex4 Fast Acting Dimetapp Cold and Colace capsule Conceptrol 4% gel Cough and Cold Glucose liquid Allergy elixir elixir Dristan nasal spray Dulcolax tablet D-Vi-Sol liquid Ecotrin tablet Evac powder Ex-Lax chewable Gas-X chewable Feosol tablet -

VHA/Dod CLINICAL PRACTICE GUIDELINE for the MANAGEMENT of POSTOPERATIVE PAIN
VHA/DoD CLINICAL PRACTICE GUIDELINE FOR THE MANAGEMENT OF POSTOPERATIVE PAIN Veterans Health Administration Department of Defense Prepared by: THE MANAGEMENT OF POSTOPERATIVE PAIN Working Group with support from: The Office of Performance and Quality, VHA, Washington, DC & Quality Management Directorate, United States Army MEDCOM VERSION 1.2 JULY 2001/ UPDATE MAY 2002 VHA/DOD CLINICAL PRACTICE GUIDELINE FOR THE MANAGEMENT OF POSTOPERATIVE PAIN TABLE OF CONTENTS Version 1.2 Version 1.2 VHA/DoD Clinical Practice Guideline for the Management of Postoperative Pain TABLE OF CONTENTS INTRODUCTION A. ALGORITHM & ANNOTATIONS • Preoperative Pain Management.....................................................................................................1 • Postoperative Pain Management ...................................................................................................2 B. PAIN ASSESSMENT C. SITE-SPECIFIC PAIN MANAGEMENT • Summary Table: Site-Specific Pain Management Interventions ................................................1 • Head and Neck Surgery..................................................................................................................3 - Ophthalmic Surgery - Craniotomies Surgery - Radical Neck Surgery - Oral-maxillofacial • Thorax (Non-cardiac) Surgery.......................................................................................................9 - Thoracotomy - Mastectomy - Thoracoscopy • Thorax (Cardiac) Surgery............................................................................................................16 -

228 April 2003 Category 1
Laparoscopica cantireflux Edward T Chory, MD Tracey A Ross, CST, MEd surgery astroesophageal Reflux The number of undiagnosed cases Disease (GERD) is a com- promises to be much higher based mon condition with a on the millions of heartburn suf- heavy economic impact. In ferers who take over-the- G a study published in the counter medications to treat May 2002 issue of Gastroenterol- their symptoms. GERD is also the ogy, researchers calculated that most expensive of the digestive GERD is one of the most preva- conditions with annual direct lent digestive diseases in America costs at $9.3 billion.1 with 19 million diagnosed cases.1 APRIL 2003 The Surgical Technologist 13 228 APRIL 2003 CATEGORY 1 Indirect costs, such as missed work and lower (painful swallowing), esophageal spasm, and productivity, would be almost impossible to more rarely GI bleeding (hematemesis or mele- measure accurately. However, companies and na). Tertiary symptoms are unrelated to the individuals are likely to feel the financial impact esophagus, such as reflux-induced asthma, in increased insurance premiums. For example, hoarseness and pharyngitis. Tertiary symptoms in 2002, the Wall Street Journal reported that the have increasingly been considered indications cost of proton pump inhibitors (PPIs) increased for antireflux surgery, and recent reports have General Motors’ health care budget for employ- documented excellent results, particularly for ees and retirees more than $55 million.2 reflux-induced asthma.11 With increasing experience in laparoscopic Traditionally, antireflux surgery was reserved antireflux surgery over the last 10 years, mor- for patients who did not respond to medical bidity has decreased, outcomes have improved therapy. -

Common Ear, Nose & Throat Problems
Common Ear, Nose & Throat Problems The information provided in this presentation is not intended to guide treatment or aid in making a diagnosis. Always consult a physician or nurse practitioner. Copyright 2002, 2014, Kevin T. Kavanagh All Rights Reserved www.entusa.com Normal Larynx Normal larynx in a 44 yr old non-smoker Go to http://www.entusa.com/normal_larynx.htm to View Video Copyright 2002, 2014, Kevin T. Kavanagh All Rights Reserved www.entusa.com Acute Laryngitis This video shows the function of the larynx in a 24 yr old patient with acute laryngitis. Talking was painful and she only talked in a faint whisper. Go to http://www.entusa.com/laryngitis.htm to View Video Copyright 2002, 2014, Kevin T. Kavanagh All Rights Reserved www.entusa.com Vocal Cord Paralysis This video shows the function of a larynx with a paralyzed left true vocal cord. The patient has lung cancer. She has a poorly compensated breathy voice which is difficult to understand. This patient had a 55 pack year history of smoking. Go to http://www.entusa.com/vocal_cord_paralysis_2.htm to View Video Copyright 2002, 2014, Kevin T. Kavanagh All Rights Reserved www.entusa.com Vocal Cord Polyp This video shows the function of a larynx with a vocal cord polyp on the right true vocal cord. This patient smoked one pack a day for 30 years. Go to http://www.entusa.com/larynx_polyp-9.htm to View Video Copyright 2002, 2014, Kevin T. Kavanagh All Rights Reserved www.entusa.com Laryngeal Cancer This video shows the function of a larynx with a large T1b Cancer on both true vocal cords and anterior commissure in 72 yr old male with a 150 pack year history of smoking. -

MEDICATIONS to AVOID PRIOR to ALLERGY SKIN TESTING Allergy
MEDICATIONS TO AVOID PRIOR TO ALLERGY SKIN TESTING Allergy testing requires the ‘histamine response’ in order to be accurate and reliable. There are many types of antihistamines. Antihistamines are found in many different medicines, either as a single drug or mixed with a combination of chemicals. Please review all medicines you take (including Over-The-Counter) in order to make your allergy testing appointment most efficient and accurate. Generic names are in all lower case, trade names Capitalized. Oral antihistamines to be stopped 3 (THREE) days prior to your appointment: - brompheniramine (Actifed, Atrohist, Dimetapp, Drixoral) - cetirizine (Zyrtec, Zyrtec D) - chlopheniramine (Chlortrimeton, Deconamine, Kronofed A, Novafed A, Rynatan, Tussinex) - clemastine (Tavist, Antihist) - cyproheptadine (Periactin) - diphenhydramine (Benadryl, Allernix, Nytol) - doxylamine (Bendectin, Nyquil) - hydroxyzine (Atarax, Marax, Vistaril) - levocetirizine (Xyzal) - promethazine (Phenergan) Oral antihistamines to be stopped 7 (SEVEN) days prior to your appointment: - desloratadine (Clarinex) - fexofenadine (Allegra, Allegra D) - loratadine (Claritin, Claritin D, Alavert) Nose spray and eye drop antihistamines to stop 5 (FIVE) days prior to your appointment: - azelastine (Astelin, Astepro, Dymista, Optivar) - bepotastine (Bepreve) - ketotifen (Zaditor, Alaway) - olapatadine (Pataday, Patanase) - pheniramine (Visine A, Naphcon A) – OK to stop for 2 days Antacid medications (different type of antihistamine) to stop 3 (THREE) days prior to your appointment: - cimetidine (Tagamet) - famotidine (Pepcid) - ranitidine (Zantac) Note: Antihistamines are found in many over the counter medications, including Tylenol Allergy, Actifed Cold and Allergy, Alka-Seltzer Plus Cold with Cough Formula, and many others. Make sure you read and check the ingredients carefully and stop those containing antihistamines at least 3 (THREE) days prior to the appointment.