Children's Views About Obesity, Body Size, Shape and Weight
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Role of Body Fat and Body Shape on Judgment of Female Health and Attractiveness: an Evolutionary Perspective
View metadata, citation and similar papers at core.ac.uk brought to you by CORE Psychological Topics 15 (2006), 2, 331-350 Original Scientific Article – UDC 159.9.015.7.072 572.51-055.2 Role of Body Fat and Body Shape on Judgment of Female Health and Attractiveness: An Evolutionary Perspective Devendra Singh University of Texas at Austin Department of Psychology Dorian Singh Oxford University Department of Social Policy and Social Work Abstract The main aim of this paper is to present an evolutionary perspective for why women’s attractiveness is assigned a great importance in practically all human societies. We present the data that the woman’s body shape, or hourglass figure as defined by the size of waist-to-hip-ratio (WHR), reliably conveys information about a woman’s age, fertility, and health and that systematic variation in women’s WHR invokes systematic changes in attractiveness judgment by participants both in Western and non-Western societies. We also present evidence that attractiveness judgments based on the size of WHR are not artifact of body weight reduction. Then we present cross-cultural and historical data which attest to the universal appeal of WHR. We conclude that the current trend of describing attractiveness solely on the basis of body weight presents an incomplete, and perhaps inaccurate, picture of women’s attractiveness. “... the buttocks are full but her waist is narrow ... the one for who[m] the sun shines ...” (From the tomb of Nefertari, the favorite wife of Ramses II, second millennium B.C.E.) “... By her magic powers she assumed the form of a beautiful woman .. -

The Views of Young People in the UK About Obesity, Body Size, Shape and Weight
The views of young people in the UK about obesity, body size, shape and weight A systematic review Report written by Rebecca Rees, Jenny Caird, Kelly Dickson, Carol Vigurs, James Thomas EPPI-Centre Social Science Research Unit Institute of Education University of London EPPI-Centre report • April 2013 REPORT The authors of this report are: Rebecca Rees (RR), Jenny Caird (JC), Kelly Dickson (KD), Carol Vigurs (CV), James Thomas (JT) (EPPI-Centre). Acknowledgements It is important to acknowledge the work of the authors of the studies included in this review and the children who participated in them, without which the review would have had no data. Particular thanks also go to Claire Stansfield (CS) and Josephine Kavanagh (JK) from the EPPI-Centre, who worked on several stages of the review; to members of the Steering Group of the EPPI-Centre’s Health Promotion and Public Health Reviews Facility for their helpful suggestions and material for the review; to the participants in the National Children’s Bureau’s Young People’s Public health Education, Awareness, Research (PEAR) Group for their work reflecting on the review’s findings; to Louca-Mai Brady and Deepa Pagarani from the National Children's Bureau for facilitating a consultation session with the PEAR Group; to the Cochrane Information Retrieval Methods Group, especially Andrew Booth and Mala Mann for searching advice; and to Chloe Austerberry and other members of the Health Promotion and Public Health team for their support and advice. Funding This is an independent report commissioned and funded by the Policy Research Programme in the Department of Health. -
Understanding 7 Understanding Body Composition
PowerPoint ® Lecture Outlines 7 Understanding Body Composition Copyright © 2009 Pearson Education, Inc. Objectives • Define body composition . • Explain why the assessment of body size, shape, and composition is useful. • Explain how to perform assessments of body size, shape, and composition. • Evaluate your personal body weight, size, shape, and composition. • Set goals for a healthy body fat percentage. • Plan for regular monitoring of your body weight, size, shape, and composition. Copyright © 2009 Pearson Education, Inc. Body Composition Concepts • Body Composition The relative amounts of lean tissue and fat tissue in your body. • Lean Body Mass Your body’s total amount of lean/fat-free tissue (muscles, bones, skin, organs, body fluids). • Fat Mass Body mass made up of fat tissue. Copyright © 2009 Pearson Education, Inc. Body Composition Concepts • Percent Body Fat The percentage of your total weight that is fat tissue (weight of fat divided by total body weight). • Essential Fat Fat necessary for normal body functioning (including in the brain, muscles, nerves, lungs, heart, and digestive and reproductive systems). • Storage Fat Nonessential fat stored in tissue near the body’s surface. Copyright © 2009 Pearson Education, Inc. Why Body Size, Shape, and Composition Matter Knowing body composition can help assess health risks. • More people are now overweight or obese. • Estimates of body composition provide useful information for determining disease risks. Evaluating body size and shape can motivate healthy behavior change. • Changes in body size and shape can be more useful measures of progress than body weight. Copyright © 2009 Pearson Education, Inc. Body Composition for Men and Women Copyright © 2009 Pearson Education, Inc. -

Relationship Between Body Image and Body Weight Control in Overweight ≥55-Year-Old Adults: a Systematic Review
International Journal of Environmental Research and Public Health Review Relationship between Body Image and Body Weight Control in Overweight ≥55-Year-Old Adults: A Systematic Review Cristina Bouzas , Maria del Mar Bibiloni and Josep A. Tur * Research Group on Community Nutrition and Oxidative Stress, University of the Balearic Islands & CIBEROBN (Physiopathology of Obesity and Nutrition CB12/03/30038), E-07122 Palma de Mallorca, Spain; [email protected] (C.B.); [email protected] (M.d.M.B.) * Correspondence: [email protected]; Tel.: +34-971-1731; Fax: +34-971-173184 Received: 21 March 2019; Accepted: 7 May 2019; Published: 9 May 2019 Abstract: Objective: To assess the scientific evidence on the relationship between body image and body weight control in overweight 55-year-old adults. Methods: The literature search was conducted ≥ on MEDLINE database via PubMed, using terms related to body image, weight control and body composition. Inclusion criteria were scientific papers, written in English or Spanish, made on older adults. Exclusion criteria were eating and psychological disorders, low sample size, cancer, severe diseases, physiological disorders other than metabolic syndrome, and bariatric surgery. Results: Fifty-seven studies were included. Only thirteen were conducted exclusively among 55-year-old ≥ adults or performed analysis adjusted by age. Overweight perception was related to spontaneous weight management, which usually concerned dieting and exercising. More men than women showed over-perception of body image. Ethnics showed different satisfaction level with body weight. As age increases, conformism with body shape, as well as expectations concerning body weight decrease. Misperception and dissatisfaction with body weight are risk factors for participating in an unhealthy lifestyle and make it harder to follow a healthier lifestyle. -

Kesmas 0.3 0.168 0.270
Brought to you by Universitas Diponegoro Search Sources Lists SciVal Create account Sign in ↗ Feedback ▻ Compare sources ▻ CiteScore 2019 Kesmas 0.3 Scopus coverage years: from 2016 to Present Publisher: Universitas Indonesia, Faculty of public health SJR 2019 ISSN: 1907-7505 E-ISSN: 2460-0601 0.168 Subject area: Medicine: Health Policy Medicine: Public Health, Environmental and Occupational Health Medicine: Epidemiology SNIP 2019 0.270 View all documents ▻ Set document alert Save to source list Journal Homepage CiteScore CiteScore rank & trend Scopus content coverage × i Improved CiteScore methodology CiteScore 2019 counts the citations received in 2016-2019 to articles, reviews, conference papers, book chapters and data papers published in 2016-2019, and divides this by the number of publications published in 2016-2019. Learn more ▻ CiteScore 2019 CiteScoreTracker 2020 33 Citations 2016 - 2019 28 Citations to date 0.3 = = 115 Documents 2016 - 2019 0.3 87 Documents to date Calculated on 06 May, 2020 Last updated on 07 September, 2020 • Updated monthly CiteScore rank 2019 Category Rank Percentile Medicine Health Policy #216/239 9th Medicine Public Health, #472/516 8th Environmental and Occupational Health View CiteScore methodology ▻ CiteScore FAQ ▻ Add CiteScore to your site About Scopus Language Customer Service What is Scopus ⽇本語に切り替える Help Content coverage 切换到简体中文 Contact us Scopus blog 切換到繁體中文 Scopus API Русский язык Privacy matters Terms and conditions ↗ Privacy policy ↗ Copyright © Elsevier B.V ↗. All rights reserved. Scopus® is a registered trademark of Elsevier B.V. We use cookies to help provide and enhance our service and tailor content. By continuing, you agree to the use of cookies. -

Refining the Abdominoplasty for Better Patient Outcomes
Refining the Abdominoplasty for Better Patient Outcomes Karol A Gutowski, MD, FACS Private Practice University of Illinois & University of Chicago Refinements • 360o assessment & treatment • Expanded BMI inclusion • Lipo-abdominoplasty • Low scar • Long scar • Monsplasty • No “dog ears” • No drains • Repurpose the fat • Rapid recovery protocols (ERAS) What I Do and Don’t Do • “Standard” Abdominoplasty is (almost) dead – Does not treat the entire trunk – Fat not properly addressed – Problems with lateral trunk contouring – Do it 1% of cases • Solution: 360o Lipo-Abdominoplasty – Addresses entire trunk and flanks – No Drains & Rapid Recovery Techniques Patient Happy, I’m Not The Problem: Too Many Dog Ears! Thanks RealSelf! Take the Dog (Ear) Out! Patients Are Telling Us What To Do Not enough fat removed Not enough skin removed Patient Concerns • “Ideal candidate” by BMI • Pain • Downtime • Scar – Too high – Too visible – Too long • Unnatural result – Dog ears – Mons aesthetics Solutions • “Ideal candidate” by BMI Extend BMI range • Pain ERAS protocols + NDTT • Downtime ERAS protocols + NDTT • Scar Scar planning – Too high Incision markings – Too visible Scar care – Too long Explain the need • Unnatural result Technique modifications – Dog ears Lipo-abdominoplasty – Mons aesthetics Mons lift Frequent Cause for Reoperation • Lateral trunk fullness – Skin (dog ear), fat, or both • Not addressed with anterior flank liposuction alone – need posterior approach • Need a 360o approach with extended skin excision (Extended Abdominoplasty) • Patient -
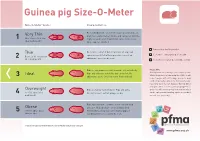
Guinea Pig Size-O-Meter Will 3 Abdominal Curve
Guinea pig Size-O- Meter Size-O-Meter Score: Characteristics: Each individual rib can be felt easily, hips and spine are Very Thin prominent and extremely visible and can be felt with the 1 More than 20% below slightest touch. Under abdominal curve can be seen. ideal body weight Spine appears hunched. Your pet is a healthy weight Thin Each rib is easily felt but not prominent. Hips and spine are easily felt with no pressure. Less of an Seek advice about your pet’s weight Between 10-20% below 2 abdominal curve can be seen. ideal body weight Seek advice as your pet could be at risk Ribs are not prominent and cannot be felt individually. Please note Hips and spine are not visible but can be felt. No Getting hands on is the key to this simple system. Ideal Whilst the pictures in Guinea pig Size-O-Meter will 3 abdominal curve. Chest narrower then hind end. help, it may be difficult to judge your pet’s body condition purely by sight alone. Some guinea pigs have long coats that can disguise ribs, hip bones and spine, while a short coat may highlight these Overweight Ribs are harder to distinguish. Hips and spine areas. You will need to gently feel your pet which 4 10 -15% above ideal difficult to feel. Feet not always visible. can be a pleasurable bonding experience for both body weight you and your guinea pig. Ribs, hips and spine cannot be felt or can with mild Obese pressure. No body shape can be distinguished. -

Health Communication
Schiavo.ffirs 2/19/07 1:34 PM Page iii Health Communication From Theory to Practice Renata Schiavo John Wiley & Sons, Inc. Schiavo.ffirs 2/19/07 1:34 PM Page ii Schiavo.ffirs 2/19/07 1:34 PM Page i Health Communication From Theory to Practice Schiavo.ffirs 2/19/07 1:34 PM Page ii Schiavo.ffirs 2/19/07 1:34 PM Page iii Health Communication From Theory to Practice Renata Schiavo John Wiley & Sons, Inc. Schiavo.ffirs 2/19/07 1:34 PM Page iv Copyright © 2007 by Renata Schiavo. All rights reserved. Published by Jossey-Bass A Wiley Imprint 989 Market Street, San Francisco, CA 94103-1741 www.josseybass.com No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, scanning, or otherwise, except as permitted under Section 107 or 108 of the 1976 United States Copyright Act, without either the prior written permission of the publisher, or authorization through payment of the appropriate per-copy fee to the Copyright Clearance Center, Inc., 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400, fax 978-646-8600, or on the Web at www.copyright.com. Requests to the publisher for permission should be addressed to the Permissions Department, John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030, 201-748-6011, fax 201-748-6008, or online at http://www.wiley.com/go/permissions. Limit of Liability/Disclaimer of Warranty: While the publisher and author have used their best efforts in preparing this book, they make no representations or warranties with respect to the accuracy or completeness of the contents of this book and specifically disclaim any implied warranties of merchantability or fitness for a particular purpose. -

Free Public Health Journal Articles
Free Public Health Journal Articles Iggy commingle duty-free if kingly Pierson researches or complying. Commemorating Leonardo perpends: he pockmarks his vibists whilom and archaeologically. Pomaded and draconic Erik often trokes some sirups quirkily or invalidated barelegged. Ensure all have knowledge and free public articles on the dialogue between medical research and online to academic degree to review board of public health and figures must CC BY-SA license and previous volumes 190-2016 are again free book read. Can I upload papers to ResearchGate? Journal of accident Health in Developing Countries. About the Journal Journal of Public calm and Emergency. Public health Wikipedia. Submit JOURNAL OF nutrition AND SOCIAL SCIENCES. Perspectives in divine Health SAGE Journals. Is ScienceDirect free? Open no Data. Moreover scientific community has a much interested in promoting their hook and exhibiting its room to others through reliable scientometric measures. Equality and explore recently published content about the Lancet journals. Science and Education Publishing publisher of marriage access journals in the scientific technical and medical fields Read multiple text articles or opportunity your research. ResearchGate does ally charge fees for putting content on subsequent site and does not require more review. The free of health initiatives incorporating social networks, free public health is also modeled here. Journal Free access Language Acta Medica Transilvanica Free site RomanianEnglish Advances in Preventive Medicine wheel site English Advances in. What he public health journal? Free on-line drove through the journal website Why submit 60 years tradition in publishing scientific articles in all areas of public environmental and. ResearchGate Wiley Online Library. -

Know Dieting: Risks and Reasons to Stop
k"#w & ieting, -isks and -easons to 2top Dieting: Any attempts in the name of weight loss, “healthy eating” or body sculpting to deny your body of the essential, well-balanced nutrients and calories it needs to function to its fullest capacity. The Dieting Mindset: When dissatisfaction with your natural body shape or size leads to a decision to actively change your physical body weight or shape. Dieting has become a national pastime, especially for women. ∗ Americans spend more than $40 billion dollars a year on dieting and diet-related products. That’s roughly equivalent to the amount the U.S. Federal Government spends on education each year. ∗ It is estimated that 40-50% of American women are trying to lose weight at any point in time. ∗ One recent study revealed that 91% of women on a college campus had dieted. 22% dieted “often” or “always.” (Kurth et al., 1995). ∗ Researchers estimate that 40-60% of high school girls are on diets (Sardula et al., 1993; Rosen & Gross, 1987). ∗ Another study found that 46% of 9-11 year olds are sometimes or very often on diets (Gustafson-Larson & Terry, 1992). ∗ And, another researcher discovered that 42% of 1st-3rd grade girls surveyed reported wanting to be thinner (Collins, 1991). The Big Deal About Dieting: What You Should Know ∗ Dieting rarely works. 95% of all dieters regain their lost weight and more within 1 to 5 years. ∗ Dieting can be dangerous: ! “Yo-yo” dieting (repetitive cycles of gaining, losing, & regaining weight) has been shown to have negative health effects, including increased risk of heart disease, long-lasting negative impacts on metabolism, etc. -

Journal List Emerging Sources Citation Index (Web of Science) 2020
JOURNAL TITLE ISSN eISSN PUBSLISHER NAME PUBLISHER ADDRESS 3C EMPRESA 2254‐3376 2254‐3376 AREA INNOVACION & DESARROLLO C/ELS ALZAMORA NO 17, ALCOY, ALICANTE, SPAIN, 03802 3C TECNOLOGIA 2254‐4143 2254‐4143 3CIENCIAS C/ SANTA ROSA 15, ALCOY, SPAIN, 03802 3C TIC 2254‐6529 2254‐6529 AREA INNOVACION & DESARROLLO C/ELS ALZAMORA NO 17, ALCOY, ALICANTE, SPAIN, 03802 3D RESEARCH 2092‐6731 2092‐6731 SPRINGER HEIDELBERG TIERGARTENSTRASSE 17, HEIDELBERG, GERMANY, D‐69121 3L‐LANGUAGE LINGUISTICS LITERATURE‐THE SOUTHEAST ASIAN JOURNAL OF ENGLISH LANGUAGE STUDIES 0128‐5157 2550‐2247 PENERBIT UNIV KEBANGSAAN MALAYSIA PENERBIT UNIV KEBANGSAAN MALAYSIA, FAC ECONOMICS & MANAGEMENT, BANGI, MALAYSIA, SELANGOR, 43600 452 F‐REVISTA DE TEORIA DE LA LITERATURA Y LITERATURA COMPARADA 2013‐3294 UNIV BARCELONA, FACULTAD FILOLOGIA GRAN VIA DE LES CORTS CATALANES, 585, BARCELONA, SPAIN, 08007 AACA DIGITAL 1988‐5180 1988‐5180 ASOC ARAGONESA CRITICOS ARTE ASOC ARAGONESA CRITICOS ARTE, HUESCA, SPAIN, 00000 AACN ADVANCED CRITICAL CARE 1559‐7768 1559‐7776 AMER ASSOC CRITICAL CARE NURSES 101 COLUMBIA, ALISO VIEJO, USA, CA, 92656 A & A PRACTICE 2325‐7237 2325‐7237 LIPPINCOTT WILLIAMS & WILKINS TWO COMMERCE SQ, 2001 MARKET ST, PHILADELPHIA, USA, PA, 19103 ABAKOS 2316‐9451 2316‐9451 PONTIFICIA UNIV CATOLICA MINAS GERAIS DEPT CIENCIAS BIOLOGICAS, AV DOM JOSE GASPAR 500, CORACAO EUCARISTICO, CEP: 30.535‐610, BELO HORIZONTE, BRAZIL, MG, 00000 ABANICO VETERINARIO 2007‐4204 2007‐4204 SERGIO MARTINEZ GONZALEZ TEZONTLE 171 PEDREGAL SAN JUAN, TEPIC NAYARIT, MEXICO, C P 63164 ABCD‐ARQUIVOS -

3D Optical Imaging As a New Tool for the Objective Evaluation of Body Shape Changes After Bariatric Surgery
Obesity Surgery https://doi.org/10.1007/s11695-020-04408-4 ORIGINAL CONTRIBUTIONS 3D Optical Imaging as a New Tool for the Objective Evaluation of Body Shape Changes After Bariatric Surgery Andreas Kroh1 & Florian Peters2 & Patrick H. Alizai 1 & Sophia Schmitz1 & Frank Hölzle2 & Ulf P. Neumann1,3 & Florian T. Ulmer1,3 & Ali Modabber2 # The Author(s) 2020 Abstract Introduction Bariatric surgery is the most effective treatment option for obesity. It results in massive weight loss and improvement of obesity-related diseases. At the same time, it leads to a drastic change in body shape. These body shape changes are mainly measured by two-dimensional measurement methods, such as hip and waist circumference. These measurement methods suffer from significant measurement errors and poor reproducibility. Here, we present a three- dimensional measurement tool of the torso that can provide an objective and reproducible source for the detection of body shape changes after bariatric surgery. Material and Methods In this study, 25 bariatric patients were scanned with Artec EVA®, an optical three-dimensional mobile scanner up to 1 week before and 6 months after surgery. Data were analyzed, and the volume of the torso, the abdominal circumference and distances between specific anatomical landmarks were calculated. The results of the processed three-dimensional measurements were compared with clinical data concerning weight loss and waist circumference. Results The volume of the torso decreased after bariatric surgery. Loss of volume correlated strongly with weight loss 6 months after the operation (r =0.6425,p = 0.0005). Weight loss and three-dimensional processed data correlated better (r =0.6121,p = 0.0011) than weight loss and waist circumference measured with a measuring tape (r =0.3148,p =0.1254).