Journal of Science / Vol 8 / Issue 1 / 2018 / 19-25
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Free PDF Download
Eur opean Rev iew for Med ical and Pharmacol ogical Sci ences 2014; 18: 440-444 Radiographic evaluation of the prevalence of enamel pearls in a sample adult dental population H. ÇOLAK, M.M. HAMIDI, R. UZGUR 1, E. ERCAN, M. TURKAL 1 Department of Restorative Dentistry, Kirikkale University School of Dentistry, Kirikkale, Turkey 1Department of Prosthodontics, Kirikkale University School of Dentistry, Kirikkale, Turkey Abstract. – AIM: Enamel pearls are a tooth One theory of the enamel pearl etiology is that anomaly that can act as contributing factors in the enamel pearls develop as a result of a localized development of periodontal disease. Studies that developmental activity of a remnant of Hertwig’s have addressed the prevalence of enamel pearls in epithelial root sheath which has remained adher - populations were scarce. The purpose of this study 5 was to evaluate the prevalence of enamel pearls in ent to the root surface during root development . the permanent dentition of Turkish dental patients It is believed that cells differentiate into function - by means of panoramic radiographs. ing ameloblasts and produce enamel deposits on PATIENTS AND METHODS: Panoramic radi - the root. The conditions needed for local differ - ographs of 6912 patients were examined for the entiation and functioning of ameloblasts in this presence of enamel pearls. All data (age, sex and ectopic position are not fully understood 6,7 . systemic disease or syndrome) were obtained from the patient files and analyzed for enamel The most common site for enamel pearls is at pearls. Descriptive characteristics of sexes, the cementoenamel junction of multirooted jaws, and dental localization were recorded. -
Developmental Disturbances Affecting Teeth
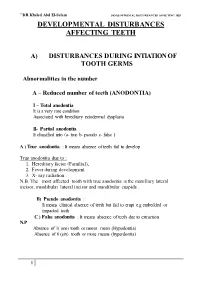
``DR.Khaled Abd El-Salam DEVELO PMENTAL DISTURBANCES AFFECTING TEET DEVELOPMENTAL DISTURBANCES AFFECTING TEETH A) DISTURBANCES DURING INTIATION OF TOOTH GERMS Abnormalities in the number A – Reduced number of teeth (ANODONTIA) I – Total anodontia It is a very rare condition Associated with hereditary ectodermal dysplasia II- Partial anodontia It classified into (a- true b- pseudo c- false ) A ) True anodontia : It means absence of teeth fail to develop True anodontia due to : 1. Hereditary factor (Familial), 2. Fever during development. 3. X- ray radiation . N.B. The most affected tooth with true anodontia is the maxillary lateral incisor, mandibular lateral incisor and mandibular cuspids . B) Pseudo anodontia : It means clinical absence of teeth but fail to erupt e.g embedded or impacted teeth C ) False anodontia : It means absence of teeth due to extraction N.P Absence of 1( one) tooth or mores mean (Hypodontia) Absence of 6 (six) tooth or more means (hyperdontia) 1 ``DR.Khaled Abd El-Salam DEVELO PMENTAL DISTURBANCES AFFECTING TEET ECTODERMAL DYSPLASIA • It is a hereditary disease which involves all structures which are derived from the ectoderm . • It is characterized by (general manifestation) : 1- Skin ( thin, smooth, Dry skin) 2- Hair (Absence or reduction (hypotrichosis). 3- Sweat-gland (Absence anhydrosis). 4- sebaceous gland ( absent lead to dry skin) 5-Temperature elevation (because of anhydrosis) 6- Depressed bridge of the nose 7- Defective mental development 8- Defective of finger nail Oral manifestation include teeth and -

A Global Compendium of Oral Health
A Global Compendium of Oral Health A Global Compendium of Oral Health: Tooth Eruption and Hard Dental Tissue Anomalies Edited by Morenike Oluwatoyin Folayan A Global Compendium of Oral Health: Tooth Eruption and Hard Dental Tissue Anomalies Edited by Morenike Oluwatoyin Folayan This book first published 2019 Cambridge Scholars Publishing Lady Stephenson Library, Newcastle upon Tyne, NE6 2PA, UK British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Copyright © 2019 by Morenike Oluwatoyin Folayan and contributors All rights for this book reserved. No part of this book may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the copyright owner. ISBN (10): 1-5275-3691-2 ISBN (13): 978-1-5275-3691-3 TABLE OF CONTENTS Foreword .................................................................................................. viii Introduction ................................................................................................. 1 Dental Development: Anthropological Perspectives ................................. 31 Temitope A. Esan and Lynne A. Schepartz Belarus ....................................................................................................... 48 Natallia Shakavets, Alexander Yatzuk, Klavdia Gorbacheva and Nadezhda Chernyavskaya Bangladesh ............................................................................................... -

DAPA 741 Oral Pathology Examination 4 December 6, 2000 1
Name: _____________________ DAPA 741 Oral Pathology Examination 4 December 6, 2000 1. Irregularity of the temporomandibular joint surfaces is a radiographic feature of A. Subluxation B. Osteoarthritis C. Trigeminal neuralgia D. Anterior disk displacement 2. Which of the following is an autoimmune disease? A. Bell’s palsy B. Osteoarthritis C. Rheumatoid arthritis D. Trigeminal neuralgia 3. Which joints are commonly affected in osteoarthritis but usually spared in rheumatoid arthritis? A. Hips B. Joints of the hands C. Knees D. Temporomandibular joint 4. Bell’s palsy may be induced by trauma to which nerve? A. Trigeminal nerve B. Glossopharyngeal nerve C. Facial nerve D. Inferior alveolar nerve 5. A patient presents to your office concerned about a painless click when she open her mouth. Your examination of her temporomandibular joint reveals a click at approximately 15 mm of opening. You instruct her to touch the incisal edges of her maxillary and mandibular anterior teeth together and then open from this position. The click disappears when she opens from this position. You diagnosis is A. Subluxation B. Anterior disk displacement C. Crepitus D. Inflammatory arthralgia 6. An ankylosed joint will cause the mandible to deviate to which side on opening? A. The affected side B. The unaffected side C. There would be no deviation on opening 7. Pain from which of the following commonly awakens the patient at night? A. Masticatory myofascial pain B. Tension headaches C. Trigeminal neuralgia D. Osteoarthritis 8. Which of the following disorders may result in blindness and is thus considered an acute ocular emergency? A. Trigeminal neuralgia B. -

Prevalence and Distribution of Dental Anomalies in a Paediatric
Prevalence and distribution of dental V.P. Wagner1, T. Arrué2, E. Hilgert2, N. A. Arús3, H. L. D. da Silveira3, anomalies in a paediatric M. D. Martins4, J. A. Rodrigues2 1Academic Unit of Oral and Maxillofacial Pathology, School of Clinical Dentistry - population based on University of Sheffield, UK 2Paediatric Dentistry Division, School of Dentistry, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil panoramic radiographs 3Oral Radiology Division, School of Dentistry, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil 4Oral Pathology Division, School of Dentistry, analysis Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil DOI 10.23804/ejpd.2020.21.04.7 e-mail: [email protected] Abstract considered to be the main aetiological factors. Variations in the dental morphology and structure, for example, typically result from disturbances during embryological development. Aim To evaluate the frequency and distribution of dental Nevertheless, environmental factors that occur during the anomalies (DA) in a paediatric population. prenatal and postnatal development period can also trigger the Material and methods Panoramic digital radiographs of children between 6 and 12 years old performed at a reference centre development of DA, particularly positional abnormalities or for radiographic exams were accessed. Two calibrated examiners disorders in the eruption chronology [Vani et al., 2016; Laganà evaluated the radiographs. The association between variables and et al., 2017]. The identification of DA is important once they outcomes was assessed using non-parametric tests. The significance can cause disturbances such as malocclusion, increased level was set at 5%. susceptibility to caries and aesthetic issues [Mukhopadhyay and Results Five hundred and twelve individuals were included Mitra, 2014]. -

Enamel Pearl Associated with Localized Periodontitis in Hellenistic Age Woman
T o m o v e t a l . C A S E R E P O R T Enamel pearl associated with localized periodontitis in Hellenistic age woman • Georgi Tomov (1), Elka Popova (2), Rumen Ivanov (3), Nadezhda Atanassova (4) • 1 - Оral Pathology Department, Faculty of Dental Medicine, Medical University, Plovdiv, Bulgaria 2 - Periodontology Department, Faculty of Dental Medicine, Medical University, Plovdiv, Bulgaria 3 - Archeologist 4 – National Anthropological Museum at Institute of Experimental Morphology, Pathology and Anthropology with Museum Address for correspondence: Assoc.Prof. Georgi Tomov, PhD Medical University Plovdiv, Faculty of Dental Medicine, Oral Pathology Department, Plovdiv, Bulgaria Phone: +359896742065 E- mail: [email protected] Bull Int Assoc Paleodont. 2017;11(2):62-66. Abstract Tooth anatomic factors like ectopic enamel pearls are often associated with localized periodontal inflammation and bone loss. There are no existing paleopathological data for such structural anomalies in ancient populations associated with periodontal pathology in the literature. A rare case of enamel pearl on the maxillary right first molar of women associated with localized periodontitis is presented and discussed. Keywords: enamel pearl; localized periodontitis; paleopathology; Hellenistic age Bull Int Assoc Paleodont. Volume 11, Number 2, 2017 www.paleodontology.com 62 Bulletin of the International Association for Paleodontology NO-FEE OPEN ACCESS JOURNAL T o m o v e t a l . C A S E R E P O R T Introduction are found in Plovdiv, Bulgaria (archeological site Bacterial plaque has been implicated as the “Kirkor Azarian” №4) and are provided for primary etiologic factor in the initiation and anthropological study in the Medical University progression of gingivitis and periodontitis (1). -

Incidental Findings in Digital Panoramic Radiography of Patients Referred to Mashhad Dental School
JKMU Journal of Kerman University of Medical Sciences, 2021; 28 (1): 43-55 Incidental Findings in Digital Panoramic Radiography of Patients Referred to Mashhad Dental School Mahrokh Imanimoghaddam, M.Sc.1, Elaheh Tohidi, M.Sc.2, Azam Ahmadian Yazdi, D.D.S.3, Ehsan Nikbakhsh, D.D.S.4, Fereshteh Goudarzi, D.D.S.5 1. Professor of Oral and Maxillofacial Radiology, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran 2. Oral and Maxillofacial Radiologist, Mashhad, Iran 3. Instructor, Department of Oral and Maxillofacial Radiology, School of Dentistry, Mashhad University, Mashhad, Iran of Medical Sciences, Mashhad, Iran 4. General dentist, Mashhad, Iran 5. Post-graduate Student of Oral and Maxillofacial Radiology, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran (Corresponding author: Email: [email protected]) Received: 1 March, 2020 Accepted: 11 November, 2020 ARTICLE INFO Abstract Background: Panoramic radiographs are among diagnostic tools used by dentists. Because Article type: of the relatively large area covered by panoramic radiographs, incidental findings are possible. Original Article This study aimed to evaluate the incidental findings in digital panoramic radiographs of patients referred to the Oral and Maxillofacial Radiology Department of Mashhad Dental Keywords: School. Radiography Methods: In this cross-sectional study, panoramic radiographs of 1987 patients over one year Panoramic were evaluated, and any finding that was not related to the reason of panoramic radiography Incidental Findings request was recorded as an incidental finding. These findings were grouped into five Jaw categories: intraosseous findings, dental abnormalities, soft tissue calcifications, maxillary Prevalence sinus findings, and TMJ findings. The obtained data were analyzed using descriptive statistics and through SPSS18.0. -

Recognition of Oral Lesions
ORAL PATHOLOGY DENTISTRY Jeanne R. Perrone, CVT, VTS (Dentistry) This session will deal with the commonly seen neoplasms of the oral cavity and those conditions that look like tumors, but arise from an outside source. Oral tumors arise from the gingiva, buccal mucosa, tongue, mandible, maxilla, palate, dental structures, or tonsils. Neoplasms from Trauma Gum Chewers Syndrome: This syndrome is caused by mechanical trauma. The pet chews on the inside of its cheek or tongue. This causes a proliferative granulomatous hyperplasia to occur at the site. If the chewing is mild, the damage will be low. In extreme cases, the lesions can become large, bleed regularly, and cause pain (Lobprise et al. 2000). Neoplasms from Infectious Agents Gingival Hyperplasia Gingival hyperplasia is a proliferation of the tissue of the attached gingiva. It may occur due to an inflammatory response such as dental plaque or calculus. The excessive gingival tissue can form what’s called a “false pocket”— the extra tissue increases the depth of the sulcus. The hyperplastic tissue is usually benign. Treatment consists of treating the underlying periodontal disease and a gingivectomy to remove the excess tissue. This condition can be an inherited trait in certain breeds such as boxers, Great Danes, collies, Doberman pinschers, and Dalmatians (Tholen et al. 1982). Pyogenic Granuloma These lesions result from irritation of a specific site on the gingiva. The gingiva proliferates the area with granulation tissue. This irritation can be a foreign body or an infected wound. Removing the irritant will usually remove the lesion (Tholen et al. 1982). Feline Eosinophilic Granuloma These are chronic, progressive lesions that involve not only the lips and the oral cavity, but the skin as well. -

Anatomic Landmarks © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT for SALE OR DISTRIBUTION NOT for SALE OR DISTRIBUTION
© Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION SECTION 1 © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION Anatomic Landmarks © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION Objectives: © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC • Recognize, define,NOT and describe FOR SALE the soft OR tissue DISTRIBUTION structures and landmarks of the anteriorNOT and FOR posterior SALE oral OR DISTRIBUTION cavity. • Recognize, define, and describe the soft tissue structures and landmarks of the floor of the mouth, tongue, and palate. • Recognize,© Jones define, & Bartlett and describe Learning, the soft LLC tissue structures and landmarks© Jones of the & periodontium. Bartlett Learning, LLC • Recognize,NOT FOR define, SALE and OR describe DISTRIBUTION the bony structures and landmarksNOT of the FOR maxilla SALE and mandible OR DISTRIBUTION and adjacent regions. • Recognize, define, and describe common variants of normal. • In the clinical setting, identify intraoral soft tissue structures and anatomic landmarks in a patient’s mouth. © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION 1 © Jones & Bartlett Learning LLC, an Ascend Learning Company. -
Glossary of Periodontal Terms.Pdf
THE AMERICAN ACADEMY OF PERIODONTOLOGY Glossary of Periodontal Te rms 4th Edition Copyright 200 I by The American Academy of Periodontology Suite 800 737 North Michigan Avenue Chicago, Illinois 60611-2690 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, or otherwise without the express written permission of the publisher. ISBN 0-9264699-3-9 The first two editions of this publication were published under the title Glossary of Periodontic Terms as supplements to the Journal of Periodontology. First edition, January 1977 (Volume 48); second edition, November 1986 (Volume 57). The third edition was published under the title Glossary vf Periodontal Terms in 1992. ACKNOWLEDGMENTS The fourth edition of the Glossary of Periodontal Terms represents four years of intensive work by many members of the Academy who generously contributed their time and knowledge to its development. This edition incorporates revised definitions of periodontal terms that were introduced at the 1996 World Workshop in Periodontics, as well as at the 1999 International Workshop for a Classification of Periodontal Diseases and Conditions. A review of the classification system from the 1999 Workshop has been included as an Appendix to the Glossary. Particular recognition is given to the members of the Subcommittee to Revise the Glossary of Periodontic Terms (Drs. Robert E. Cohen, Chair; Angelo Mariotti; Michael Rethman; and S. Jerome Zackin) who developed the revised material. Under the direction of Dr. Robert E. Cohen, the Committee on Research, Science and Therapy (Drs. David L. -

DHY-140 / General and Oral Pathology
Course Name: General and Oral Pathology Instructor Name: Jodi Major BS RDH Course Number: DHY 140 Course Department: Dental Hygiene/ STEMM Course Term: Spring 2020 Last Revised by Department: 10-13-19 Total Semester Hour(s) Credit: 2 Total Contact Hours per Semester: Lecture: 30 hours Lab: 0 Clinical: 0 Internship/Practicum: 0 Catalog Description: This course encompasses the fundamental study of abnormal findings in and around the oral cavity, including identification of lesions, developmental disorders, neoplasia, genetics, inflammation, degenerative changes, oral manifestations of diseases and/or conditions. Instruction emphasizes case studies, vocabulary and terminology; along with the comprehensive integration throughout all clinical aspects of the inspection of the oral cavity and surrounding structures. Pre-requisites and/or Co-requisites: DHY-114 Dental Hygiene Anatomical Sciences Textbook(s) Required: Isben& Phelan, Oral Pathology for the Dental Hygienist, 7th ed Saunders. St Loius Optional: Langlasis & Miller, Color Atlas of Oral Disease, Williams & Wilkins, current ed. Access Code: No Required Materials: Textbook, index cards Suggested Materials: Binder, folder Course Fees: None Institutional Outcomes: Critical Thinking: The ability to dissect a multitude of incoming information, sorting the pertinent from the irrelevant, in order to analyze, evaluate, synthesize, or apply the information to a defendable conclusion. Effective Communication: Information, thoughts, feelings, attitudes, or beliefs transferred either verbally or nonverbally through a medium in which the intended meaning is clearly and correctly understood by the recipient with the expectation of feedback. Personal Responsibility: Initiative to consistently meet or exceed stated expectations over time. Department Outcomes: • To promote excellence in instruction and create a safe and nurturing learning environment that facilitates student learning and improves client care through research, guided self-study, online activities and varied clinical instructional opportunities.