Matrix Metalloproteinase-12 Expression Correlates with Local Recurrence and Metastatic Disease in Non–Small Cell Lung Cancer Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Epithelial-Specific Knockout of the Rac1 Gene Leads to Enamel Defects
Eur J Oral Sci 2011; 119 (Suppl. 1): 168–176 Ó 2011 Eur J Oral Sci DOI: 10.1111/j.1600-0722.2011.00904.x European Journal of Printed in Singapore. All rights reserved Oral Sciences Zhan Huang1, Jieun Kim2, Rodrigo Epithelial-specific knockout of the Rac1 S. Lacruz1, Pablo Bringas Jr1, Michael Glogauer3, Timothy G. gene leads to enamel defects Bromage4, Vesa M. Kaartinen2, Malcolm L. Snead1 1The Center for Craniofacial Molecular Biology, Huang Z, Kim J, Lacruz RS, Bringas P Jr, Glogauer M, Bromage TG, Kaartinen VM, Herman Ostrow School of Dentistry, University of Southern California, Los Angeles, CA, USA; Snead ML. Epithelial-specific knockout of the Rac1 gene leads to enamel defects. 2 Eur J Oral Sci 2011; 119 (Suppl. 1): 168–176. Ó 2011 Eur J Oral Sci Department of Biologic and Materials Sciences, School of Dentistry, University of Michigan, Ann Arbor, MI, USA; 3Matrix The Ras-related C3 botulinum toxin substrate 1 (Rac1) gene encodes a 21-kDa GTP- Dynamics Group, Faculty of Dentistry, binding protein belonging to the RAS superfamily. RAS members play important University of Toronto, Toronto, Ontario, roles in controlling focal adhesion complex formation and cytoskeleton contraction, Canada; 4New York University College of activities with consequences for cell growth, adhesion, migration, and differentiation. Dentistry, New York, NY, USA To examine the role(s) played by RAC1 protein in cell–matrix interactions and enamel matrix biomineralization, we used the Cre/loxP binary recombination system to characterize the expression of enamel matrix proteins and enamel formation in Rac1 knockout mice (Rac1)/)). Mating between mice bearing the floxed Rac1 allele and mice bearing a cytokeratin 14-Cre transgene generated mice in which Rac1 was absent Zhan Huang, The Center for Craniofacial from epithelial organs. -

Discovery and Optimization of Selective Inhibitors of Meprin Α (Part II)
pharmaceuticals Article Discovery and Optimization of Selective Inhibitors of Meprin α (Part II) Chao Wang 1,2, Juan Diez 3, Hajeung Park 1, Christoph Becker-Pauly 4 , Gregg B. Fields 5 , Timothy P. Spicer 1,6, Louis D. Scampavia 1,6, Dmitriy Minond 2,7 and Thomas D. Bannister 1,2,* 1 Department of Molecular Medicine, Scripps Research, Jupiter, FL 33458, USA; [email protected] (C.W.); [email protected] (H.P.); [email protected] (T.P.S.); [email protected] (L.D.S.) 2 Department of Chemistry, Scripps Research, Jupiter, FL 33458, USA; [email protected] 3 Rumbaugh-Goodwin Institute for Cancer Research, Nova Southeastern University, 3321 College Avenue, CCR r.605, Fort Lauderdale, FL 33314, USA; [email protected] 4 The Scripps Research Molecular Screening Center, Scripps Research, Jupiter, FL 33458, USA; [email protected] 5 Unit for Degradomics of the Protease Web, Institute of Biochemistry, University of Kiel, Rudolf-Höber-Str.1, 24118 Kiel, Germany; fi[email protected] 6 Department of Chemistry & Biochemistry and I-HEALTH, Florida Atlantic University, 5353 Parkside Drive, Jupiter, FL 33458, USA 7 Dr. Kiran C. Patel College of Allopathic Medicine, Nova Southeastern University, 3301 College Avenue, Fort Lauderdale, FL 33314, USA * Correspondence: [email protected] Abstract: Meprin α is a zinc metalloproteinase (metzincin) that has been implicated in multiple diseases, including fibrosis and cancers. It has proven difficult to find small molecules that are capable Citation: Wang, C.; Diez, J.; Park, H.; of selectively inhibiting meprin α, or its close relative meprin β, over numerous other metzincins Becker-Pauly, C.; Fields, G.B.; Spicer, which, if inhibited, would elicit unwanted effects. -

Transmembrane/Cytoplasmic, Rather Than Catalytic, Domains of Mmp14
RESEARCH ARTICLE 343 Development 140, 343-352 (2013) doi:10.1242/dev.084236 © 2013. Published by The Company of Biologists Ltd Transmembrane/cytoplasmic, rather than catalytic, domains of Mmp14 signal to MAPK activation and mammary branching morphogenesis via binding to integrin 1 Hidetoshi Mori1,*, Alvin T. Lo1, Jamie L. Inman1, Jordi Alcaraz1,2, Cyrus M. Ghajar1, Joni D. Mott1, Celeste M. Nelson1,3, Connie S. Chen1, Hui Zhang1, Jamie L. Bascom1, Motoharu Seiki4 and Mina J. Bissell1,* SUMMARY Epithelial cell invasion through the extracellular matrix (ECM) is a crucial step in branching morphogenesis. The mechanisms by which the mammary epithelium integrates cues from the ECM with intracellular signaling in order to coordinate invasion through the stroma to make the mammary tree are poorly understood. Because the cell membrane-bound matrix metalloproteinase Mmp14 is known to play a key role in cancer cell invasion, we hypothesized that it could also be centrally involved in integrating signals for mammary epithelial cells (MECs) to navigate the collagen 1 (CL-1)-rich stroma of the mammary gland. Expression studies in nulliparous mice that carry a NLS-lacZ transgene downstream of the Mmp14 promoter revealed that Mmp14 is expressed in MECs at the tips of the branches. Using both mammary organoids and 3D organotypic cultures, we show that MMP activity is necessary for invasion through dense CL-1 (3 mg/ml) gels, but dispensable for MEC branching in sparse CL-1 (1 mg/ml) gels. Surprisingly, however, Mmp14 without its catalytic activity was still necessary for branching. Silencing Mmp14 prevented cell invasion through CL-1 and disrupted branching altogether; it also reduced integrin 1 (Itgb1) levels and attenuated MAPK signaling, disrupting Itgb1- dependent invasion/branching within CL-1 gels. -

Nuclear Matrix Metalloproteinases: Functions Resemble the Evolution from the Intracellular to the Extracellular Compartment
OPEN Citation: Cell Death Discovery (2017) 3, 17036; doi:10.1038/cddiscovery.2017.36 Official journal of the Cell Death Differentiation Association www.nature.com/cddiscovery REVIEW Nuclear matrix metalloproteinases: functions resemble the evolution from the intracellular to the extracellular compartment Yingqiu Xie1,2,5, Aidana Mustafa1,5, Adina Yerzhan1,5, Dalmira Merzhakupova1, Perizat Yerlan1, Askarbek N Orakov1, Xiao Wang3, Yi Huang4 and Lixia Miao2 Matrix metalloproteinase (MMP) is defined as an endopeptidase in the extracellular matrix (ECM), which plays essential roles in physiological processes such as organogenesis, wound healing, angiogenesis, apoptosis and motility. MMPs are produced and assembled in the cytoplasm as proenzymes with a cytoplasmic domain and require extracellular activation. MMPs can degrade receptors, extracellular matrix proteins, PARPs and release apoptotic substances. MMPs have been found in the cytosol, organelles and extracellular compartments and recently many types of MMPs have been found in the nucleus. However, the mechanisms and roles of MMPs inside the cell nucleus are still poorly understood. Here we summarized the nuclear localization mechanisms of MMPs and their functions in the nucleus such as apoptosis, tissue remodeling upon injury and cancer progression. Most importantly, we found that nuclear MMPs have evolved to translocate to membrane and target ECM possibly through evolution of nuclear localization signal (NLS), natural selection and anti-apoptotic survival. Thus, the knowledge about the evolution and regulation of nuclear MMPs appears to be essential in understanding a variety of cellular processes along with the development of MMP-targeted therapeutic drugs against the progression of certain diseases. Cell Death Discovery (2017) 3, 17036; doi:10.1038/cddiscovery.2017.36; published online 14 August 2017 KEY FACTS MMP-10, MMP-13 and MMP-14. -
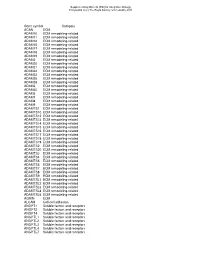
Gene Symbol Category ACAN ECM ADAM10 ECM Remodeling-Related ADAM11 ECM Remodeling-Related ADAM12 ECM Remodeling-Related ADAM15 E
Supplementary Material (ESI) for Integrative Biology This journal is (c) The Royal Society of Chemistry 2010 Gene symbol Category ACAN ECM ADAM10 ECM remodeling-related ADAM11 ECM remodeling-related ADAM12 ECM remodeling-related ADAM15 ECM remodeling-related ADAM17 ECM remodeling-related ADAM18 ECM remodeling-related ADAM19 ECM remodeling-related ADAM2 ECM remodeling-related ADAM20 ECM remodeling-related ADAM21 ECM remodeling-related ADAM22 ECM remodeling-related ADAM23 ECM remodeling-related ADAM28 ECM remodeling-related ADAM29 ECM remodeling-related ADAM3 ECM remodeling-related ADAM30 ECM remodeling-related ADAM5 ECM remodeling-related ADAM7 ECM remodeling-related ADAM8 ECM remodeling-related ADAM9 ECM remodeling-related ADAMTS1 ECM remodeling-related ADAMTS10 ECM remodeling-related ADAMTS12 ECM remodeling-related ADAMTS13 ECM remodeling-related ADAMTS14 ECM remodeling-related ADAMTS15 ECM remodeling-related ADAMTS16 ECM remodeling-related ADAMTS17 ECM remodeling-related ADAMTS18 ECM remodeling-related ADAMTS19 ECM remodeling-related ADAMTS2 ECM remodeling-related ADAMTS20 ECM remodeling-related ADAMTS3 ECM remodeling-related ADAMTS4 ECM remodeling-related ADAMTS5 ECM remodeling-related ADAMTS6 ECM remodeling-related ADAMTS7 ECM remodeling-related ADAMTS8 ECM remodeling-related ADAMTS9 ECM remodeling-related ADAMTSL1 ECM remodeling-related ADAMTSL2 ECM remodeling-related ADAMTSL3 ECM remodeling-related ADAMTSL4 ECM remodeling-related ADAMTSL5 ECM remodeling-related AGRIN ECM ALCAM Cell-cell adhesion ANGPT1 Soluble factors and receptors -
Effect of Nanoparticles on the Expression and Activity of Matrix Metalloproteinases
Nanotechnol Rev 2018; 7(6): 541–553 Review Magdalena Matysiak-Kucharek*, Magdalena Czajka, Krzysztof Sawicki, Marcin Kruszewski and Lucyna Kapka-Skrzypczak Effect of nanoparticles on the expression and activity of matrix metalloproteinases https://doi.org/10.1515/ntrev-2018-0110 Received September 14, 2018; accepted October 11, 2018; previously 1 Introduction published online November 15, 2018 Matrix metallopeptidases, commonly known as matrix Abstract: Matrix metallopeptidases, commonly known metalloproteinases (MMPs), are zinc-dependent proteo- as matrix metalloproteinases (MMPs), are a group of pro- lytic enzymes whose primary function is the degradation teolytic enzymes whose main function is the remodeling and remodeling of extracellular matrix (ECM) compo- of the extracellular matrix. Changes in the activity of nents. ECM is a complex, dynamic structure that condi- these enzymes are observed in many pathological states, tions the proper tissue architecture. MMPs by digesting including cancer metastases. An increasing body of evi- ECM proteins eliminate structural barriers and allow dence indicates that nanoparticles (NPs) can lead to the cell migration. Moreover, by hydrolyzing extracellularly deregulation of MMP expression and/or activity both in released proteins, MMPs can change the activity of many vitro and in vivo. In this work, we summarized the current signal peptides, such as growth factors, cytokines, and state of knowledge on the impact of NPs on MMPs. The chemokines. MMPs are involved in many physiological literature analysis showed that the impact of NPs on MMP processes, such as embryogenesis, reproduction cycle, or expression and/or activity is inconclusive. NPs exhibit wound healing; however, their increased activity is also both stimulating and inhibitory effects, which might be associated with a number of pathological conditions, such dependent on multiple factors, such as NP size and coat- as diabetes, cardiovascular diseases and neurodegenera- ing or a cellular model used in the research. -

Supplementary Table S4. FGA Co-Expressed Gene List in LUAD
Supplementary Table S4. FGA co-expressed gene list in LUAD tumors Symbol R Locus Description FGG 0.919 4q28 fibrinogen gamma chain FGL1 0.635 8p22 fibrinogen-like 1 SLC7A2 0.536 8p22 solute carrier family 7 (cationic amino acid transporter, y+ system), member 2 DUSP4 0.521 8p12-p11 dual specificity phosphatase 4 HAL 0.51 12q22-q24.1histidine ammonia-lyase PDE4D 0.499 5q12 phosphodiesterase 4D, cAMP-specific FURIN 0.497 15q26.1 furin (paired basic amino acid cleaving enzyme) CPS1 0.49 2q35 carbamoyl-phosphate synthase 1, mitochondrial TESC 0.478 12q24.22 tescalcin INHA 0.465 2q35 inhibin, alpha S100P 0.461 4p16 S100 calcium binding protein P VPS37A 0.447 8p22 vacuolar protein sorting 37 homolog A (S. cerevisiae) SLC16A14 0.447 2q36.3 solute carrier family 16, member 14 PPARGC1A 0.443 4p15.1 peroxisome proliferator-activated receptor gamma, coactivator 1 alpha SIK1 0.435 21q22.3 salt-inducible kinase 1 IRS2 0.434 13q34 insulin receptor substrate 2 RND1 0.433 12q12 Rho family GTPase 1 HGD 0.433 3q13.33 homogentisate 1,2-dioxygenase PTP4A1 0.432 6q12 protein tyrosine phosphatase type IVA, member 1 C8orf4 0.428 8p11.2 chromosome 8 open reading frame 4 DDC 0.427 7p12.2 dopa decarboxylase (aromatic L-amino acid decarboxylase) TACC2 0.427 10q26 transforming, acidic coiled-coil containing protein 2 MUC13 0.422 3q21.2 mucin 13, cell surface associated C5 0.412 9q33-q34 complement component 5 NR4A2 0.412 2q22-q23 nuclear receptor subfamily 4, group A, member 2 EYS 0.411 6q12 eyes shut homolog (Drosophila) GPX2 0.406 14q24.1 glutathione peroxidase -

Self-Organization of Engineered Epithelial Tubules by Differential Cellular Motility
Self-organization of engineered epithelial tubules by differential cellular motility Hidetoshi Moria,1, Nikolce Gjorevskib,1, Jamie L. Inmana,1, Mina J. Bissella,2, and Celeste M. Nelsonb,2 aLife Sciences Division, Lawrence Berkeley National Laboratory, Berkeley, CA 94720; and bDepartments of Chemical Engineering and Molecular Biology, Princeton University, Princeton, NJ 08544 Edited by Kenneth Yamada, National Institutes of Health, Bethesda, MD, and accepted by the Editorial Board July 16, 2009 (received for review February 4, 2009) Patterning of developing tissues arises from a number of mecha- also in many epithelial tumors, including those from breast, lung, nisms, including cell shape change, cell proliferation, and cell sorting and colon (17–19), and confers cancer cells with the pernicious from differential cohesion or tension. Here, we reveal that differences ability to degrade and penetrate the basement membrane and in cell motility can also lead to cell sorting within tissues. Using mosaic metastasize to distant sites (20–23). Intriguingly, cells at the invasive engineered mammary epithelial tubules, we found that cells sorted front of metastatic cohorts express the highest levels of MMP14 (24, depending on their expression level of the membrane-anchored 25). Understanding how the expression pattern of this protease is collagenase matrix metalloproteinase (MMP)-14. These rearrange- determined will likely yield insights into possible mechanisms of ments were independent of the catalytic activity of MMP14 but cancer progression and invasion. absolutely required the hemopexin domain. We describe a signaling Here we present evidence to suggest that cellular rearrange- cascade downstream of MMP14 through Rho kinase that allows cells ments generated by differential cellular motility determine the to sort within the model tissues. -

How the Matrix Metalloproteinase MMP14 Contributes to the Progression of Colorectal Cancer
How the matrix metalloproteinase MMP14 contributes to the progression of colorectal cancer Lena Claesson-Welsh J Clin Invest. 2020. https://doi.org/10.1172/JCI135239. Commentary Certain matrix metalloproteinase (MMP) family proteins have been associated with cell proliferation and invasion in aggressive cancers. However, attempts to target the MMPs with the hope of treating tumors have thus far failed. In this issue of the JCI, Ragusa and coworkers identified an intestinal cancer subgroup of slow-growing, chemotherapy-resistant, and very aggressive matrix-rich tumors that mimic a hard-to-treat colorectal cancer subtype in humans. These tumors showed downregulated levels of the transcription factor prospero homeobox protein 1 (PROX1), which relieved repression of the matrix metalloproteinase MMP14. Upregulated MMP14 levels correlated with blood vessel dysfunction and a lack of cytotoxic T cells. Notably, blockade of proangiogenic factors in combination with stimulation of the CD40 pathway in the mouse cancer model boosted cytotoxic T cell infiltration. The study illustrates how combinatorial treatments for aggressive, T cell–deficient cancers can launch an antitumor immune response. Find the latest version: https://jci.me/135239/pdf The Journal of Clinical Investigation COMMENTARY How the matrix metalloproteinase MMP14 contributes to the progression of colorectal cancer Lena Claesson-Welsh Uppsala University, Beijer and Science for Life Laboratories, Department of Immunology, Genetics and Pathology, Uppsala, Sweden. expression (8). What happens in the low- PROX1–expressing tumors? This is now Certain matrix metalloproteinase (MMP) family proteins have been resolved by Ragusa and coworkers, who associated with cell proliferation and invasion in aggressive cancers. used a range of genetic mouse models However, attempts to target the MMPs with the hope of treating tumors in which intestinal cancer developed have thus far failed. -

Human Induced Pluripotent Stem Cell–Derived Podocytes Mature Into Vascularized Glomeruli Upon Experimental Transplantation
BASIC RESEARCH www.jasn.org Human Induced Pluripotent Stem Cell–Derived Podocytes Mature into Vascularized Glomeruli upon Experimental Transplantation † Sazia Sharmin,* Atsuhiro Taguchi,* Yusuke Kaku,* Yasuhiro Yoshimura,* Tomoko Ohmori,* ‡ † ‡ Tetsushi Sakuma, Masashi Mukoyama, Takashi Yamamoto, Hidetake Kurihara,§ and | Ryuichi Nishinakamura* *Department of Kidney Development, Institute of Molecular Embryology and Genetics, and †Department of Nephrology, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan; ‡Department of Mathematical and Life Sciences, Graduate School of Science, Hiroshima University, Hiroshima, Japan; §Division of Anatomy, Juntendo University School of Medicine, Tokyo, Japan; and |Japan Science and Technology Agency, CREST, Kumamoto, Japan ABSTRACT Glomerular podocytes express proteins, such as nephrin, that constitute the slit diaphragm, thereby contributing to the filtration process in the kidney. Glomerular development has been analyzed mainly in mice, whereas analysis of human kidney development has been minimal because of limited access to embryonic kidneys. We previously reported the induction of three-dimensional primordial glomeruli from human induced pluripotent stem (iPS) cells. Here, using transcription activator–like effector nuclease-mediated homologous recombination, we generated human iPS cell lines that express green fluorescent protein (GFP) in the NPHS1 locus, which encodes nephrin, and we show that GFP expression facilitated accurate visualization of nephrin-positive podocyte formation in -

Extracellular Matrix Alterations in Metastatic Processes
International Journal of Molecular Sciences Review Extracellular Matrix Alterations in Metastatic Processes Mayra Paolillo * and Sergio Schinelli Department of Drug Sciences, University of Pavia, 27100 Pavia, Italy; [email protected] * Correspondence: [email protected] Received: 17 September 2019; Accepted: 30 September 2019; Published: 7 October 2019 Abstract: The extracellular matrix (ECM) is a complex network of extracellular-secreted macromolecules, such as collagen, enzymes and glycoproteins, whose main functions deal with structural scaffolding and biochemical support of cells and tissues. ECM homeostasis is essential for organ development and functioning under physiological conditions, while its sustained modification or dysregulation can result in pathological conditions. During cancer progression, epithelial tumor cells may undergo epithelial-to-mesenchymal transition (EMT), a morphological and functional remodeling, that deeply alters tumor cell features, leading to loss of epithelial markers (i.e., E-cadherin), changes in cell polarity and intercellular junctions and increase of mesenchymal markers (i.e., N-cadherin, fibronectin and vimentin). This process enhances cancer cell detachment from the original tumor mass and invasiveness, which are necessary for metastasis onset, thus allowing cancer cells to enter the bloodstream or lymphatic flow and colonize distant sites. The mechanisms that lead to development of metastases in specific sites are still largely obscure but modifications occurring in target tissue ECM are being intensively studied. Matrix metalloproteases and several adhesion receptors, among which integrins play a key role, are involved in metastasis-linked ECM modifications. In addition, cells involved in the metastatic niche formation, like cancer associated fibroblasts (CAF) and tumor associated macrophages (TAM), have been found to play crucial roles in ECM alterations aimed at promoting cancer cells adhesion and growth. -
Ultra-Processed Food Targets Bone Quality Via Endochondral Ossification
Bone Research www.nature.com/boneres ARTICLE OPEN Ultra-processed food targets bone quality via endochondral ossification Janna Zaretsky1, Shelley Griess-Fishheimer1, Adi Carmi1, Tamara Travinsky Shmul1, Lior Ofer2, Tali Sinai1, Svetlana Penn1, Ron Shahar2 and Efrat Monsonego-Ornan 1 Ultra-processed foods have known negative implications for health; however, their effect on skeletal development has never been explored. Here, we show that young rats fed ultra-processed food rich in fat and sugar suffer from growth retardation due to lesions in their tibial growth plates. The bone mineral density decreases significantly, and the structural parameters of the bone deteriorate, presenting a sieve-like appearance in the cortices and poor trabecular parameters in long bones and vertebrae. This results in inferior mechanical performance of the entire bone with a high fracture risk. RNA sequence analysis of the growth plates demonstrated an imbalance in extracellular matrix formation and degradation and impairment of proliferation, differentiation and mineralization processes. Our findings highlight, for the first time, the severe impact of consuming ultra-processed foods on the growing skeleton. This pathology extends far beyond that explained by the known metabolic effects, highlighting bone as a new target for studies of modern diets. Bone Research (2021) ;9:14 https://doi.org/10.1038/s41413-020-00127-9 1234567890();,: INTRODUCTION penetration of blood vessels and bone tissue formation by The vertebrate skeleton has evolved as a dynamic system that osteoblasts.1,2,4,6 The EO process is tightly orchestrated by various serves numerous functions, such as protecting internal organs, signaling molecules and transcription factors, including transform- creating attachment sites for muscles to produce locomotion, ing growth factor β/bone morphogenetic protein (BMP), fibroblast providing a reservoir for minerals, and serving as a hematopoietic growth factor (FGF), Wnt, hedgehog, and the transcription factor niche.