Setting Local Government Priorities in Healthcare Infrastructure Using The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

City Branding Analysis to Pangandaran Regency: a Review from Tourists’ Perspective
Review of Integrative Business and Economics Research, Vol. 8, Supplementary Issue 4 135 City Branding Analysis to Pangandaran Regency: A Review from Tourists’ Perspective Pratami Wulan Tresna Business Administration Department, Universitas Padjadjaran Tetty Herawaty Business Administration Department, Universitas Padjadjaran Arianis Chan Business Administration Department, Universitas Padjadjaran ABSTRACT These days, every city or region has done much marketing effort as one of the ways to elevate the number of visit of tourists. Building a strong positioning and creating innovation different to other cities are some of the ways. It can be realized by applying city branding in city planning. Pangandaran is one of the regions in Indonesia that has high natural and tourism potentials. These potentials become the foundation of a region in doing city branding so the city can achieve brand equity. The aim of this research is to analyze how city branding of Pangandaran is seen from the perspective of its tourists. The method used in this research was quantitative research. The sample of this research was 293 people. The data analysis technique used was the SEM method with the PLS approach. The result shows that attitude has a significant influence directly to brand preference. Brand equity has a significant influence directly to brand preference. Brand image does not have a significant influence directly to brand preference. Keywords: city branding, brand equity, attitude, brand preference, brand image. 1. INTRODUCTION A city or region planning which aims at gaining a strong positioning in tourists’ mind can be achieved by applying city branding in the planning. City branding is a theoretical and practical approach that is the most accurate according to Kavaratzis (2004), moreover if talking about an image of a city (Vermeulen, 2002). -
Level of Capture Hospitality Based on the Type and Size of Shrimp Capture in Pangandaran
GSJ: Volume 8, Issue 7, July 2020 ISSN 2320-9186 2364 GSJ: Volume 8, Issue 7, July 2020, Online: ISSN 2320-9186 www.globalscientificjournal.com LEVEL OF CAPTURE HOSPITALITY BASED ON THE TYPE AND SIZE OF SHRIMP CAPTURE IN PANGANDARAN Wiji Prabowo1*, Herman Hamdani1, IzzaMahdiana Apriliani1and Dedi Supriadi1 1Department of Fisheries, Faculty of Marines and Fisheries, University of Padjadjaran, Jl. Raya Bandung–Sumedang Km 21, Jatinangor 40600, Indonesia. *E-mail address :[email protected] ABSTRAK This study aims to determine the fishing gear used to capture shrimp commodities and analyze the productive andeco-friendly fishing gear in Pangandaran. Data collection was conducted from November 1 to December 18, 2019 using fishing gear to capture shrimp commodities; three-layer nets (trammel net), dogol nets, beach seine and bernong nets. The method used in this research is the case-study method. Data analysis includes composition of catch types, catch size composition, composition of catch utilization and analysis the level of eco-friendly. The results from this study showed that the fishing gear most widely used by Pangandaran fishermen to catch shrimp commodities is the bernong nets. Fishing gear that has the highest level of eco- friendly is a three-layer net (trammel net) which belongs to the category of eco-friendly fishing gear. While fishing gear bernongnets, dogol nets and trawlers are included in the category of fishing gear that is noeco- friendly Keywords : Fishing Gear, Pangandaran, Producticity, Eco-friendly. GSJ© 2020 www.globalscientificjournal.com GSJ: Volume 8, Issue 7, July 2020 ISSN 2320-9186 2365 1. INTRODUCTION Pangandaran is one of the districts in West Java that has potential in the fisheries. -

Government Policy Strategy in the Development of Capture Fisheries in Pangandaran Regency, West Java Province
GSJ: Volume 8, Issue 1, January 2020 ISSN 2320-9186 729 GSJ: Volume 8, Issue 1, January 2020, Online: ISSN 2320-9186 www.globalscientificjournal.com GOVERNMENT POLICY STRATEGY IN THE DEVELOPMENT OF CAPTURE FISHERIES IN PANGANDARAN REGENCY, WEST JAVA PROVINCE Aida Maulida Farhani1 *, Asep Agus Handaka2, Eddy Arianto2, and Achmad Rizal2 1Student of Fisheries, Faculty of Fisheries and Marine Sciences, Padjadjaran University, Indonesia 2Departments of Fisheries, Faculty of Fisheries and Marine Sciences, Padjadjaran University, Indonesia *E-mail address: [email protected] ABSTRACT Pangandaran Regency is one of the regencies in West Java with the capital of the Regency located in the District of Parigi. Pangandaran coast and sea is one of the areas included in the 573 Fisheries Management Area (WPP) zone, WPP 573. This area is a mainstay for capture fisheries. So that the capture fisheries sector contributes greatly to the regional economy and society in the Pangandaran region. Therefore a regional government policy strategy is needed as an effort to develop capture fisheries in Pangandaran Regency. This research aims to describe the profile of local government policy strategies in the past five years as an effort to develop capture fisheries in Pangandaran Regency and to analyze the policies that have been implemented so that they can be recommended in the field of capture fisheries. The research method used in this research is a descriptive method on the basis of case studies. Analysis of the data used in this study uses the Soft System Methodology approach. Based on an unstructured problem-solving approach, it represents an exiting condition. Exiting conditions include technical or production aspects, institutional aspects, and aspects of Human Resources. -

Development of Tourism Potential in Watersports Recreation, Santirah River, Pangandaran Regency, Indonesia
PEOPLE: International Journal of Social Sciences ISSN 2454-5899 Rahmafitria et al., 2017 Volume 3 Issue 1, pp. 712 - 720 Date of Publication: 23rd March, 2017 DOI-https://dx.doi.org/10.20319/pijss.2017.s31.712720 This paper can be cited as: Rahmafitria, F., Wirakusuma, R., M., & Riswandi, A. (2017). Development of Tourism Potential in Watersports Recreation, Santirah River, Pangandaran Regency, Indonesia. PEOPLE: International Journal of Social Sciences, 3(1), 712-720. This work is licensed under the Creative Commons Attribution-Non Commercial 4.0 International License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc/4.0/ or send a letter to Creative Commons, PO Box 1866, Mountain View, CA 94042, USA. DEVELOPMENT OF TOURISM POTENTIAL IN WATERSPORTS RECREATION, SANTIRAH RIVER, PANGANDARAN REGENCY, INDONESIA Fitri Rahmafitria Universitas Pendidikan Indonesia, Bandung, Indonesia [email protected] Reiza Miftah Wirakusuma Universitas Pendidikan Indonesia, Bandung, Indonesia [email protected] Agus Riswandi Universitas Pendidikan Indonesia, Bandung, Indonesia [email protected] Abstract River is one of a recreational resource potential of watersport in Indonesia. The growing trend of sports tourism in water-based recreation, making some rivers and rapids with unique morphology, being developed by the local community as a tourism destination. Furthermore, comprehensive planning and meticulous study, is the key to develop sustainable sports tourism. This study was conducted as a series of special interest travel planning process-based education that used the river with River Tubing Activity as an attraction. The sample was taken on Santirah River which is currently growing as one of a favorite attraction in West Java, Indonesia. -

Download This PDF File
THE INTERNATIONAL JOURNAL OF BUSINESS REVIEW (THE JOBS REVIEW), 2 (2), 2019, 107-120 Regional Typology Approach in Education Quality in West Java Based on Agricultural and Non-Agricultural Economic Structure Nenny Hendajany1, Deden Rizal2 1Program Studi Manajemen, Universitas Sangga Buana, Bandung, Indonesia 2Program Studi Keuangan Perbankan, Universitas Sangga Buana, Bandung, Indonesia Abstract. West Java is the province in Indonesia with the highest population and has a location close to the capital. However, the condition of education in West Java is generally still low. This is estimated because there are imbalances between districts / cities. The research objective is to get a clear picture of the condition of education in West Java by using secondary data issued by the Central Statistics Agency. The research method uses descriptive analysis, with analysis tools of regional typology. The division of regional typologies from the two indicators produces four regional terms, namely developed regions, developed regions constrained, potential areas to develop, and disadvantaged areas. Based on the indicators of education quality and life expectancy in 2017, from 27 municipal districts in West Java there were 33.3% in developed regions, 18.52% in developed regions were constrained, 7.4% in potential developing regions, and 40.74 % in disadvantaged areas. Bandung and Bekasi regencies are included in developed regions. While the cities of Banjar and Tasikmalaya include potential developing regions. Regional division with three indicators, namely the average length of school, Location Quation, and life expectancy. This division produces three filled quadrants. Quadrant I has 29.6%, quadrant III has 18.5%, and the remaining 51.9% is in quadrant IV. -

Analysis of Blank Spot Data in the Communication Area with the Geoprocessing Method in Southern West Java
Universal Journal of Electrical and Electronic Engineering 6(2A): 15-21, 2019 http://www.hrpub.org DOI: 10.13189/ujeee.2019.061304 Analysis of Blank Spot Data in the Communication Area with the Geoprocessing Method in Southern West Java R. A. E. Virgana*, Dan Dani Hamdani Department of IS, Faculty of Engineering, Widyatama University, Indonesia Copyright©2019 by authors, all rights reserved. Authors agree that this article remains permanently open access under the terms of the Creative Commons Attribution License 4.0 International License Abstract In this study, the southern part of West Java south coast roads, and some of which have just been Province, especially along the southern coastline in Cianjur created and connected after there is a national program of Regency (in part), Garut Regency, Tasikmalaya Regency, alternative road routes along the southern coast of Java. and Pangandaran Regency, has tremendous potential. For As seen in Figure 1, a blank spot survey path of BTS the southern path of West Java alone, 417.4 km connected, (Base Transceiver Station) signals in this study, is limited from the start of Sukabumi Regency to the west of West to only those lines. Java, to Pangandaran Regency in the east of West Java, the The limitation of the research path is due to limited time potential and uniqueness of almost all new roads along the and costs, and limit research problems, so only the south southern path of West Java show the extraordinary beauty coast of West Java, from Cianjur Regency (part of the and natural resources of West Java. Almost all roads on this region) in the West (the starting point of Balegede District), track it is very neat, new and sturdy bridges. -

Analysisofhumanresourc
GSJ: Volume 7, Issue 12, December 2019 ISSN 2320-9186 202 GSJ: Volume 7, Issue 12, December 2019, Online: ISSN 2320-9186 www.globalscientificjournal.com ANALYSIS OF HUMAN RESOURCES COMPETITIVENESS OF MINAPADI AQUACULTURE FISHERIES IN WEST JAVA PROVINCE Rosidah**, Annes Ilyas *, Asep. A.H. Suryana **, Atikah Nurhayati** *) Bachelor of Fisheries and Marine Sciences Faculty, University of Padjadjaran **) Lecturer of Fisheries and Marine Sciences Faculty, University of Padjadjaran Email : [email protected] ABSTRACT The fisheries sector is an important sector for the people of Indonesia and can be used as a prime mover of the national economy. Minapadi cultivation is a fisheries sector with a system of rice and fish cultivation which is cultivated together in a paddy field. West Java Province as one of the biggest producing regions of Minapadi fisheries in Indonesia, and is considered as a potential area for Minapadi cultivation. The potential of human resources affects the efforts of business entities in achieving maximum mineral production. Minapadi aquaculture competitiveness can be used as a benchmark for regional development, regional mapping, and regional development planning. This study has the objective to analysis of human resources competitiveness of Minapadi aquaculture in West Java Province. The method used in this study is the litelature survey method to determine the competitiveness of minapadi cultivation in 18 regencys and nine cities in West Java Province. After all data has been processed, the data will be analyzed descriptively. The technique used to retrieve primary data in this study in the from of expert judgment. Whereas secondary data was obtained from statistical data of the Office of Maritime Affairs and Fisheries of West Java Province. -
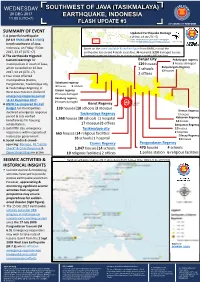
Earthquake, Indonesia 11.00 (Utc+7) Flash Update #3
WEDNESDAY SOUTHWEST OF JAVA (TASIKMALAYA) 20 DEC 2017 EARTHQUAKE, INDONESIA 11.00 (UTC+7) FLASH UPDATE #3 SUMMARY OF EVENT Updated Earthquake Damage 1. A powerful earthquake (19 Dec, 19.00 UTC +7) (M 6.9 BMKG; M 6.5 USGS) Source: Compiled based on public statement/infographic released by BNPB, BPBD West Java and BPBD Central Java 1 cm = 22.2 km struck southwest of Java, Indonesia, on Friday 15 Dec Based on the latest available & verified figure from BNPB, in total the 2017, 23.47 (UTC +7). earthquake has caused 4 death casualties, 36 injured & 3,290 damaged houses. 2. The earthquake triggered Discrepancies between local & regional data are subjected to changes as advised by BNPB latest figure. tsunami warnings for Banjar City Pekalongan regency municipalities in south of Java, 129 houses 3 houses damaged which cancelled on 16 Dec Banjarnegara Regency 2 schools 12 houses 2017, 02.26 (UTC +7). 2 offices 3. Four most affected municipalities (Ciamis, Pangandaran, Tasikmalaya city Sukabumi regency 3 houses 3 schools & Tasikmalaya Regency) in Cianjur regency West Java Province declared 2 houses damaged emergency response period Bandung regency 16-22 December 2017. M 6.9 2 houses damaged 7.75 E, 108.11 E 4. BNPB has prepared On-Call Garut Regency Depth 107 km Budget for municipalities 139 houses|10 schools|3 mosque declared emergency response Sleman Regency Tasikmalaya Regency 1 houses period & lists verified 1,568 houses|30 schools |1 hospital Kebumen Regency beneficiaries for housing 12 houses rehabilitation. 17 mosque|8 offices Banyumas Regency 5. Until fifth day, emergency Tasikmalaya city 22 houses response is within capacity of 665 houses|14 religious facilities 2 hospitals Cilacap Regency Indonesian government. -

Minasari Village Unit Cooperative Role to Improve Fishermen Welfare in Pangandaran Regency, West Javaprovince
GSJ: Volume 7, Issue 6, June 2019 ISSN 2320-9186 944 GSJ: Volume 7, Issue 6, June 2019, Online: ISSN 2320-9186 www.globalscientificjournal.com MINASARI VILLAGE UNIT COOPERATIVE ROLE TO IMPROVE FISHERMEN WELFARE IN PANGANDARAN REGENCY, WEST JAVA PROVINCE Annisa Heydi Oktafiani1, Atikah Nurhayati2, Achmad Rizal2, Isni Nurruhwati2 1) Student of the Faculty of Fisheries and Marine Sciences, Universitas Padjadjaran 2) Staff Lecture of the Faculty of Fisheries and Marine Sciences, Universitas Padjadjaran Fisheries Study Program, Faculty of Fisheries and Marine Sciences, Universitas Padjadjaran Jl. Raya Bandung – Sumedang Km 21, Jatinangor 40600 Email: [email protected] ABSTRACT This research aims to analyze the role of Minasari Village Unit Cooperative in Pangandaran Regency and evaluate the performance of Minasari Village Unit Cooperative in Pangandaran Regency to increase the welfare of fishermen. The research was conducted at the Minasari Village Unit Cooperative in Pangandaran Regency starting from January to February 2019. The method used in this research is the descriptive method by using primary data in the form of questionnaires and secondary data. The collected data used purposive sampling for 60 respondent members of the Village Unit Cooperative (KUD) Minasari who worked as fishermen. The analyzed research by Likert Scale in the data processing. The research results of fishermen who are members of the Village Unit Cooperative (KUD) Minasari have the role of Minasari Village Unit Cooperative Pangandaran has an average index value at 67,07. This average index means the role of Minasari Village Unit Cooperative to increase the welfare of fishermen in Pangandaran Regency is considered good by its respondent which catches layur fish the most using gillnet as fishing gear and boat with 3-5 GT of the fishing fleets. -

Indication of Source in West Java Province: the First Government's Certification on Local Products in Indonesia
Indication of Source in West Java Province: the First Government's Certification on Local Products in Indonesia Miranda Risang Ayu Palar, S.H., LL.M., Ph.D. Head of Intellectual Property Centre for Regulation and Application Studies, Department of Law on Information Technology and Intellectual Property, Faculty of Law, Universitas Padjadjaran, West Java, Indonesia Intellectual Property Rights Exclusive Rights Communal IPR Inclusive Rights Intellectual Property Rights Individual IPR Exclusive Rights Communal Intellectual Property Rights Exclusive Rights Lisbon System Paris Convention System EU System TRIPS Agreement Trade Names Controlled Appellations of Origin Geographical Collective Marks Indications Protected Designations of Certification Origin Marks Traditional Indications Specialized of Source Guarrantee Communal Intellectual Property Rights Inclusive Rights Moral Rights Economic & Moral Rights Traditional Intangible Traditional Genetic Indications Cultural Cultural Knowledge Resources of Source Heritage Expression IS, GI, AO in International Legal Instruments Indications of Source (IS) . Paris Convention for the Protection of Industrial Property of 1883 and the 1911 Revision . Madrid Agreement of 1891 for the Repression of False or Deceptive Indications of Source on Goods Geographical Indications (GIs) . Agreement on the Establishment of the World Trade Organization – Agreement on the Trade Related Aspects of Intellectual Property Rights 1994 IS, GIs, AO in International Legal Instruments Appellations of Origin . Lisbon Agreement of 1958 for the Protection of Appellations of Origin and their Registration (rev. 1967, amn. 1979) . Administrative Instructions for the Application of the Lisbon Agreement 2010 . International Convention of 1951 on the Use of Appellations of Origin and Denominations of Cheeses (Stresa Convention) Appellations of Origin & Geographical Indications . Geneva Act of the Lisbon Agreement on Appellations of Origin and Geographical Indications 2015 . -

Download Article (PDF)
Advances in Social Science, Education and Humanities Research, volume 510 6th International Conference on Social and Political Sciences (ICOSAPS 2020) The Role of Cultural Community in the Development of Local Culture in Pangandaran Region Priyo Subekti1* Hanny Hafiar2 Iriana Bakti3 1,2,3Faculty of Communication Sciences, Universitas Padjadjaran, Jawa Barat, Indonesia 1Corresponding author Email: [email protected] ABSTRACT Pangandaran Regency is rich in culture and art that have not been published, so that many Indonesian people do not know. Pangandaran distinctive cultures being preserved and introduced to the public currently are Ronggeng Gunung (typical culture of Pangandaran Regency), the ocean, the leuweung celebration and the charm of the coastal full moon. The Pangandaran Regency Government cooperates with Kompepar (tourism driving community) in disseminating information on the potential of both nature and culture that can provide a positive image about Pangandaran as a world tourist destination. For this reason, the Cultural Community in Pangandaran cooperates with the government in order to control the administration of arts environment groups. The government has a role to play in providing recommendations for whether or not a cultural group is given an art operational permit. The research method used in this study is the descriptive method via qualitative data. This descriptive research aims to describe what currently applies. Inside it, there are efforts to describe, to record, to analyze and to interpret the conditions currently happening or existing. In other words, this descriptive study aims to obtain information about existing conditions Pengandaran is prepared to be one of the tourist destinations, both natural (natural) based tourism and local cultural based tourism. -
The Contribution of Fisheries Sector in Regional Development of Pangandaran Regency West Java Province
GSJ: Volume 8, Issue 1, January 2020 ISSN 2320-9186 1217 GSJ: Volume 8, Issue 1, January 2020, Online: ISSN 2320-9186 www.globalscientificjournal.com THE CONTRIBUTION OF FISHERIES SECTOR IN REGIONAL DEVELOPMENT OF PANGANDARAN REGENCY WEST JAVA PROVINCE. Ridho Julianto1, Asep Agus Handaka Suryana2, Achmad Rizal2, Atikah Nurhayati2 1Student at Faculty of Fisheries and Marine Science, Padjadjaran University, Bandung – Sumedang KM. 21 Jatinangor 45363, Indonesia E-mail address: [email protected] 2Lecturer at Faculty of Fisheries and Marine Science, Padjadjaran University, Bandung – Sumedang KM. 21 Jatinangor 45363, Indonesia KeyWords Contribution of Fisheries Sector, Regional Development, Growth Indices Analysis, Trade Area Capture and the Pull Factor Analysis, Minimum Requirement Approach Analysis. ABSTRACT The purpose of this research is to analyze the growth of the fisheries sector, analyze the strength of the commodity market, and analyze the strength of the fisheries sector-based sector in regional development in Pangandaran Regency. The method used in this study is a quantita- tive method using secondary data which is then analyzed using descriptive statistics and qualitative methods using primary data obtained through interviews. The analysis used is growth analysis, Trade Area Capture (TAC) analysis, Pull Factor analysis (PF) and Minimum Needs Approach (MRA) analysis. The results of the growth index analysis show that the GDP of the fisheries sector in the Pangandaran Regency increased revenue by 3% within two years. The results of the 2014-2016 TAC analysis showed the value of the TAC> population showed that Pangandaran Regency was able to estimate the trade value of other regional fishery products. The PF value of the Pangandaran Regency fisheries sector> 1 which shows that the Pangandaran Regency region can attract customers from other regions.