Pharmacodynamics of Cholinesterase Inhibitors Suggests Add-On
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Comparison of the Binding of Reversible Inhibitors to Human Butyrylcholinesterase and Acetylcholinesterase: a Crystallographic, Kinetic and Calorimetric Study
Article Comparison of the Binding of Reversible Inhibitors to Human Butyrylcholinesterase and Acetylcholinesterase: A Crystallographic, Kinetic and Calorimetric Study Terrone L. Rosenberry 1, Xavier Brazzolotto 2, Ian R. Macdonald 3, Marielle Wandhammer 2, Marie Trovaslet-Leroy 2,†, Sultan Darvesh 4,5,6 and Florian Nachon 2,* 1 Departments of Neuroscience and Pharmacology, Mayo Clinic College of Medicine, Jacksonville, FL 32224, USA; [email protected] 2 Département de Toxicologie et Risques Chimiques, Institut de Recherche Biomédicale des Armées, 91220 Brétigny-sur-Orge, France; [email protected] (X.B.); [email protected] (M.W.); [email protected] (M.T.-L.) 3 Department of Diagnostic Radiology, Dalhousie University, Halifax, NS B3H 4R2, Canada; [email protected] 4 Department of Medical Neuroscience, Dalhousie University, Halifax, NS B3H 4R2, Canada; [email protected] 5 Department of Chemistry, Mount Saint Vincent University, Halifax, NS B3M 2J6, Canada 6 Department of Medicine (Neurology and Geriatric Medicine), Dalhousie University, Halifax, NS B3H 4R2, Canada * Correspondence: [email protected]; Tel.: +33-178-65-1877 † Deceased October 2016. Received: 26 October 2017; Accepted: 27 November 2017; Published: 29 November 2017 Abstract: Acetylcholinesterase (AChE) and butyrylcholinesterase (BChE) hydrolyze the neurotransmitter acetylcholine and, thereby, function as coregulators of cholinergic neurotransmission. Although closely related, these enzymes display very different substrate specificities that only partially overlap. This disparity is largely due to differences in the number of aromatic residues lining the active site gorge, which leads to large differences in the shape of the gorge and potentially to distinct interactions with an individual ligand. Considerable structural information is available for the binding of a wide diversity of ligands to AChE. -

X-Ray Structures of Torpedo Californica Acetylcholinesterase Complexed
X-ray Structures of Torpedo californica Acetylcholinesterase Complexed with (+)-Huperzine A and (-)-Huperzine B: Structural Evidence for an Active Site Rearrangement†,‡ H. Dvir,§,| H. L. Jiang,§,⊥ D. M. Wong,§,| M. Harel,§ M. Chetrit,§ X. C. He,⊥ G. Y. Jin,⊥ G. L. Yu,⊥ X. C. Tang,⊥ I. Silman,| D. L. Bai,*,⊥ and J. L. Sussman*,§ Departments of Structural Biology and Neurobiology, Weizmann Institute of Science, RehoVot 76100, Israel, and State Key Laboratory of Drug Research, Shanghai Institute of Materia Medica, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences, Shanghai 200031, Peoples Republic of China ReceiVed February 20, 2002; ReVised Manuscript ReceiVed June 26, 2002 ABSTRACT: Kinetic and structural data are presented on the interaction with Torpedo californica acetylcholinesterase (TcAChE) of (+)-huperzine A, a synthetic enantiomer of the anti-Alzheimer drug, (-)-huperzine A, and of its natural homologue (-)-huperzine B. (+)-Huperzine A and (-)-huperzine B bind to the enzyme with dissociation constants of 4.30 and 0.33 µM, respectively, compared to 0.18 µM for (-)-huperzine A. The X-ray structures of the complexes of (+)-huperzine A and (-)-huperzine B with TcAChE were determined to 2.1 and 2.35 Å resolution, respectively, and compared to the previously determined structure of the (-)-huperzine A complex. All three interact with the “anionic” subsite of the active site, primarily through π-π stacking and through van der Waals or C-H‚‚‚π interactions with Trp84 and Phe330. Since their R-pyridone moieties are responsible for their key interactions with the active site via hydrogen bonding, and possibly via C-H‚‚‚π interactions, all three maintain similar positions and orientations with respect to it. -

1. Magnetic Nanoparticles: from Diagnosis to Therapy
Research Signpost Trivandrum Kerala, India Recent Advances in Pharmaceutical Sciences VIII, 2018: 1-18 ISBN: 978-81-308-0579-5 Editors: Diego Muñoz-Torrero, Yolanda Cajal and Joan Maria Llobet 1. Magnetic nanoparticles: From diagnosis to therapy M. Antònia Busquets and Joan Estelrich Department of Pharmacy, Pharmaceutical Technology and Physical Chemistry Institute of Nanoscience and Nanotechnology, IN2UB Faculty of Pharmacy and Food Sciences, University of Barcelona Avda Joan XXIII, 27-31, 08028 Barcelona Abstract. Magnetic nanoparticles have proven to be promising theranostic agents, namely tools for therapy and diagnosis. Among them, superparamagnetic iron oxide nanoparticles (SPIONs) highlight for their biocompatibility and reduced toxicity. Here, we describe the synthesis and characterization of SPIONs by co-precipitation of ferric and ferrous salts under mild conditions. These particles were able to accumulate in inflamed areas fact that was increased upon the application of an external magnetic field. Resonance magnetic imaging studies have shown their suitability as negative contrast agents for diagnosis. In addition, hybrid nanoparticles were obtained by incorporating the above described SPIONs into liposomes or nanoemulsions. The findings have confirmed the high potential of these systems for biomedical applications. Introduction The impact of nanotechnology is strongly associated to the development of nanomaterials and nanoparticles (NPs) [1,2]. In particular, magnetic nanoparticles (MNs) present a number of advantages if compared to other Correspondence/Reprint request: Dr. M. Antònia Busquets, Department of Pharmacy, Pharmaceutical Technology and Physical Chemistry, Faculty of Pharmacy and Food Sciences, University of Barcelona, Avda Joan XXIII, 27-31, 08028 Barcelona. E-mail: [email protected] 2 M. Antònia Busquets & Joan Estelrich nanosystems. -
Wo 2010/117727 A2
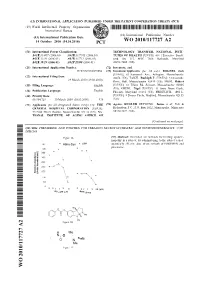
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date 14 October 2010 (14.10.2010) WO 2010/117727 A2 (51) International Patent Classification: TECHNOLOGY TRANSFER, NATIONAL INSTI¬ A61K 31/407 (2006.01) A61K 31/7105 (2006.01) TUTES OF HEALTH [US/US]; 601 1 Executive Boule A61K 31/40 (2006.01) A61K 31/711 (2006.01) vard, Ste 325, MSC 7660, Bethesda, Maryland A61K 38/16 (2006.01) A61P 25/00 (2006.01) 20892-7660 (US). (21) International Application Number: (72) Inventors; and PCT/US2010/029056 (75) Inventors/Applicants (for US only): ROGERS, Jack [USAJS]; 63 Sunnyside Ave., Arlington, Massachusetts (22) International Filing Date: 02474 (US). TANZI, Rudolph E. [US/US]; 3 Oceanside 29 March 2010 (29.03.2010) Drive, Hull, Massachusetts 02045 (US). MOIR, Robert (25) Filing Language: English [US/US]; 6 1 Tilden Rd, Scituate, Massachusetts 02066 (US). GREIG, Nigel [US/US]; 11 Anne Brent Garth, (26) Publication Language: English Phoenix, Maryland 2 113 1 (US). FRIEDLICH, Avi L. (30) Priority Data: [US/US]; 8 Dwyer Circle, Medford, Massachusetts 02155 61/164,729 30 March 2009 (30.03.2009) US (US). (71) Applicants (for all designated States except US): THE (74) Agents: KUGLER DEYOUNG, Janice et al; Fish & GENERAL HOSPITAL CORPORATION [US/US]; Richardson P.C , P.O. Box 1022, Minneapolis, Minnesota 55 Fruit Street, Boston, Massachusetts 021 14 (US). NA¬ 55440-1022 (US). TIONAL INSTITUTE OF AGING OFFICE OF [Continued on next page] (54) Title: PHENSERINE AND POSIPHEN FOR TREATING NEUROP SYCHIATRIC AND NEURODEGENERATIVE CON DITIONS Figure IA (57) Abstract: Described are methods for treating synucle- inopathy in a subject, by administering to the subject a ther 453 Abha-Syn apeutically effective dose of one or both of POSIPHEN and phenserine. -

Druglike Leads for Steric Discrimination Between Substrate
Chem Biol Drug Des 2011; 78: 495–504 ª 2011 John Wiley & Sons A/S doi: 10.1111/j.1747-0285.2011.01157.x Research Article Drug-like Leads for Steric Discrimination between Substrate and Inhibitors of Human Acetylcholinesterase Scott A. Wildman1,†, Xiange Zheng1,†, One focus of AChE research lies in the development of new drugs David Sept2, Jeffrey T. Auletta3, Terrone L. that could prevent and ⁄ or treat poisoning from organophosphates Rosenberry3 and Garland R. Marshall1,* (OPs), toxic agents commonly used in insecticides as well as in chemical warfare agents (2). OP poisoning causes the inactivation 1Department of Biochemistry and Molecular Biophysics, Washington of AChE that prevents synaptic transmission, leading to muscle University, St. Louis, MO 63110, USA paralysis, hypertension, and malfunction of various organ systems, 2Department of Biomedical Engineering, University of Michigan, Ann ultimately leading to death. Arbor, MI 48109, USA 3Department of Neuroscience, Mayo Clinic, Jacksonville, FL 32224, Two ligand-binding sites in AChE have been identified, the acylation USA site (A-site) at the base of a deep active-site gorge and the periph- *Corresponding author: Garland R. Marshall, eral site (P-site) near the gorge entrance through which ligands must [email protected] pass on their way to the A-site (3–5). Figure 1 shows the binding Authors contributed equally to this work. gorge of human AChE with acetylcholine modeled into both the A- site (green) and P-site (pink) as described in Methods. OPs are toxic Protection of the enzyme acetylcholinesterase because they covalently react with S203 in the A-site. Wilson and (AChE) from the toxic effects of organophosphate Ginsburg (6,7) conceived complementary oxime compounds that insecticides and chemical warfare agents (OPs) may be provided by inhibitors that bind at the could re-activate OP-poisoned AChE. -

Structural Dynamics of Acetylcholinesterase and Its Implications in Reactivators Design Gianluca Santoni
Structural dynamics of acetylcholinesterase and its implications in reactivators design Gianluca Santoni To cite this version: Gianluca Santoni. Structural dynamics of acetylcholinesterase and its implications in reactivators design. Biomolecules [q-bio.BM]. Université Grenoble Alpes, 2015. English. NNT : 2015GREAY019. tel-01212481 HAL Id: tel-01212481 https://tel.archives-ouvertes.fr/tel-01212481 Submitted on 6 Oct 2015 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. THÈSE Pour obtenir le grade de DOCTEUR DE L’UNIVERSITÉ DE GRENOBLE Spécialité : Physique pour les sciences du vivant Arrêté ministériel : 7 Aout 2006 Présentée par Gianluca SANTONI Thèse dirigée par Martin WEIK et codirigée par Florian NACHON préparée au sein de l’Institut de Biologie Structurale de Grenoble et de l’école doctorale de physique Structural dynamics of acetyl- cholinesterase and its implications in reactivator design Thèse soutenue publiquement le 30/01/2015, devant le jury composé de : Dr. Yves Bourne Directeur de recherche CNRS, AFMB Marseille, Rapporteur Dr. Etienne Derat Maitre de conference, Université Pierre et Marie Curie, Paris, Rapporteur Prof. Pierre-Yves Renard Professeur, Université de Normandie, Rouen, Examinateur Prof. Israel Silman Professeur, Weizmann Institute of Science,Rehovot, Examinateur Dr. -
Functional Brain Activity in Alzheimer Patients As
Thesis for doctoral degree (Ph.D.) 2007 Thesis for doctoral degree (Ph.D.) 2007 Functional Brain Activity In Alzheimer Patients as Studied by Multi-tracer Positron Emission Tomography – Effects of Treatment with Cholinesterase Inhibitors Functional Brain Activity In AD Patients as Studied by Multi-tracer PET – Effects of Treatment with ChEIs Treatment of – Effects AD Patients as Studied by Multi-tracer PET Activity In Functional Brain Ahmadul Kadir MD Ahmadul Kadir Division of Alzheimer Neurobiology Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden FUNCTIONAL BRAIN ACTIVITY IN ALZHEIMER PATIENTS AS STUDIED BY MULTI-TRACER POSITRON EMISSION TOMOGRAPHY – EFFECTS OF TREATMENT WITH CHOLINESTERASE INHIBITORS AHMADUL KADIR, MD Stockholm 2007 All previously published papers were reproduced with permission from the publisher. Published by Karolinska Institutet. Printed by Larserics Digital Print AB © Ahmadul Kadir, 2007 ISBN 978-91-7357-357-3 To My parents for their support and caring & My wife for love and affection ABSTRACT Alzheimer’s disease (AD) is a progressive neurodegenerative disease accompanied by cognitive impairment and disturbances in several neurotransmitter systems, especially the cholinergic system. Studies have correlated the cognitive impairment observed in AD patients with a deficit in central cholinergic neurotransmission. The most successful therapeutic agents for symptomatic treatment of AD patients are cholinesterase inhibitors (ChEIs), e.g. donepezil, rivastigmine and galantamine, which are targeted towards enhancing cholinergic neurotransmission. One of the most valuable tools for evaluating cholinergic neurotransmission in AD patients is positron emission tomography (PET). PET with high spatial resolution, has successfully been used in the early diagnosis, differential diagnosis and evaluation of drug treatment in patients suffering from AD. -

Role of Plant Derived Alkaloids and Their Mechanism in Neurodegenerative Disorders
Int. J. Biol. Sci. 2018, Vol. 14 341 Ivyspring International Publisher International Journal of Biological Sciences 2018; 14(3): 341-357. doi: 10.7150/ijbs.23247 Review Role of Plant Derived Alkaloids and Their Mechanism in Neurodegenerative Disorders Ghulam Hussain1,3, Azhar Rasul4,5, Haseeb Anwar3, Nimra Aziz3, Aroona Razzaq3, Wei Wei1,2, Muhammad Ali4, Jiang Li2, Xiaomeng Li1 1. The Key Laboratory of Molecular Epigenetics of MOE, Institute of Genetics and Cytology, Northeast Normal University, Changchun 130024, China 2. Dental Hospital, Jilin University, Changchun 130021, China 3. Department of Physiology, Faculty of Life Sciences, Government College University, Faisalabad, 38000 Pakistan 4. Department of Zoology, Faculty of Life Sciences, Government College University, Faisalabad, 38000 Pakistan 5. Chemical Biology Research Group, RIKEN Center for Sustainable Resource Science. 2-1 Hirosawa, Wako, Saitama 351-0198 Japan Corresponding authors: Professor Xiaomeng Li, The Key Laboratory of Molecular Epigenetics of Ministry of Education, Institute of Genetics and Cytology, Northeast Normal University, 5268 People's Street, Changchun, Jilin 130024, P.R. China. E-mail: [email protected] Tel: +86 186 86531019; Fax: +86 431 85579335 or Professor Jiang Li, Department of Prosthodontics, Dental Hospital, Jilin University, 1500 Tsinghua Road, Changchun, Jilin 130021, P.R. China. E-mail: [email protected] © Ivyspring International Publisher. This is an open access article distributed under the terms of the Creative Commons Attribution (CC BY-NC) license (https://creativecommons.org/licenses/by-nc/4.0/). See http://ivyspring.com/terms for full terms and conditions. Received: 2017.10.09; Accepted: 2017.12.18; Published: 2018.03.09 Abstract Neurodegenerative diseases are conventionally demarcated as disorders with selective loss of neurons. -

Natural Product for the Treatment of Alzheimer's Disease
J Basic Clin Physiol Pharmacol 2017; 28(5): 413–423 Review Thanh Tung Bui* and Thanh Hai Nguyen Natural product for the treatment of Alzheimer’s disease https://doi.org/10.1515/jbcpp-2016-0147 Received September 27, 2016; accepted May 28, 2017; previously Pathogenesis of Alzheimer’s disease published online July 14, 2017 Until now, the pathogenesis of AD is not yet completely Abstract: Alzheimer’s disease (AD) is related to increas- understood. The genetic susceptibility and environmental ing age. It is mainly characterized by progressive neu- factors are responsible for late onset sporadic AD, which rodegenerative disease, which damages memory and is the most common form of the disease. Many studies cognitive function. Natural products offer many options have attempted to understand the disease mechanism and to reduce the progress and symptoms of many kinds of develop a disease-modifying drug. Two main factors are diseases, including AD. Meanwhile, natural compound responsible for the development of AD: β-amyloid protein structures, including lignans, flavonoids, tannins, poly- and abnormal tau protein, or both of them. AD is charac- phenols, triterpenes, sterols, and alkaloids, have anti- teristized by the overproduction of β-amyloid proteins (Aβ) inflammatory, antioxidant, anti-amyloidogenic, and and hyperphosphorylated Tau protein, which can lead to anticholinesterase activities. In this review, we summa- the loss of synaptic connections and neurons in the hip- rize the pathogenesis and targets for treatment of AD. We pocampus and cerebral cortex, a decline in cognitive func- also present several medicinal plants and isolated com- tion, and dementia [2]. The accumulation of β-amyloid pounds that are used for preventing and reducing symp- protein and neurofibrillary tangles have been shown in toms of AD. -

Prosaic Foods and the Brain–Heart Connection in Alzheimer Disease
microorganisms Communication The Microbiota–Gut–Brain Axis–Heart Shunt Part II: Prosaic Foods and the Brain–Heart Connection in Alzheimer Disease Mark Obrenovich 1,2,3,4,5,*, Shams Tabrez 6,7, Bushra Siddiqui 8, Benjamin McCloskey 3 and George Perry 9 1 Research Service, Louis Stokes Cleveland, Department of Veteran’s Affairs Medical Center, Cleveland, OH 44106, USA 2 Department of Chemistry, Case Western Reserve University, Cleveland, OH 44106, USA 3 The Gilgamesh Foundation for Medical Science and Research, Cleveland, OH 44116, USA; [email protected] 4 Department of Medicinal and Biological Chemistry, College of Pharmacy and Pharmaceutical Sciences, University of Toledo, Toledo, OH 43606, USA 5 Departments of Chemistry and Biological and Environmental Sciences, Cleveland State University, Cleveland, OH 44115, USA 6 King Fahd Medical Research Center, King Abdulaziz University, Jeddah 21589, Saudi Arabia; [email protected] 7 Department of Medical Laboratory Technology, Faculty of Applied Medical Sciences, King Abdulaziz University, Jeddah 21589, Saudi Arabia 8 North East Ohio College of Medicine, Rootstown, OH 44272, USA; [email protected] 9 Department of Biology, University of Texas at San Antonio, San Antonio, TX 78249, USA; [email protected] * Correspondence: [email protected] Received: 31 December 2019; Accepted: 26 March 2020; Published: 31 March 2020 Abstract: There is a strong cerebrovascular component to brain aging, Alzheimer disease, and vascular dementia. Foods, common drugs, and the polyphenolic compounds contained in wine modulate health both directly and through the gut microbiota. This observation and novel findings centered on nutrition, biochemistry, and metabolism, as well as the newer insights we gain into the microbiota-gut-brain axis, now lead us to propose a shunt to this classic triad, which involves the heart and cerebrovascular systems. -

Click Chemistry in Situ
COMMUNICATIONS Click Chemistry In Situ: Acetylcholinesterase of connecting reactions: formation of hydrazone or Schiff as a Reaction Vessel for the Selective Assembly base adducts, disulfide bond formation, alkylation of free of a Femtomolar Inhibitor from an Array of thiols or amines, epoxide ring-opening, or olefin metathe- [5, 6, 8, 11, 15±19] Building Blocks** sis. Most closely related to the work described herein is the generation of carbonic anhydrase inhibitors by a Warren G. Lewis, Luke G. Green, Flavio Grynszpan, using the SN2reaction of a thiol with an -chloroketone in the Zoran Radic¬, Paul R. Carlier, Palmer Taylor, presence of the enzyme target.[16] M. G. Finn,* and K. Barry Sharpless* Most of the above strategies share the limitation that the reactive groups on the ligand probes (building blocks), being The generation and/or optimization of lead compounds by either electrophiles or nucleophiles, are likely to react in combinatorial methods has become widely accepted in undesired ways within biochemical systems. An alternative is medicinal chemistry, and is the subject of continued improve- offered by the ™cream of the crop∫ among ™click reac- ment.[1±3] However, most combinatorial strategies remain tions∫[20]–the Huisgen 1,3-dipolar cycloaddition of azides and dependent upon iterative cycles of synthesis and screening. acetylenes to give 1,2,3-triazoles [Eq. (1)].[21±23] This water- The direct involvement of the target, usually a receptor or enzyme, in the selection, evolution, and screening of drug candidates can accelerate the discovery process by short- circuiting its traditionally stepwise nature.[4±11] The use of an enzyme target to select building blocks and synthesize its own inhibitor is a relatively unexplored option. -

Research Strategies Developed for the Treatment of Alzheimer's
426 Drug Design and Discovery in Alzheimer’s Disease, 2014, 426-477 CHAPTER 8 Research Strategies Developed for the Treatment of Alzheimer’s Disease. Reversible and Pseudo-Irreversible Inhibitors of Acetylcholinesterase: Structure-Activity Relationships and Drug Design Mauricio Alcolea-Palafoxa,*, Paloma Posada-Morenob,c, Ismael Ortuño- Sorianob,c, José L. Pacheco-del-Cerroc, Carmen Martínez-Rincónc, Dolores Rodríguez-Martínezc and Lara Pacheco-Cuevasc aChemical-Physics Department, Chemistry Faculty, Complutense University of Madrid, Spain; bInstitute for Health Research at the San Carlos Clinical Hospital (IdISSC), Madrid, Spain; cNursing Department, Complutense University of Madrid, Spain Abstract: Although several research strategies have been developed in the last decades, the current therapeutic options for the treatment of Alzheimer’s disease are limited to three acetylcholinesterase inhibitors: galantamine, donepezil and rivastigmine. However, they have only offered a modest improvement in memory and cognitive function. Moreover, these drugs show side effects, and relatively low bioavailability among other problems. These features limit their use in medicine and they lead to a great demand for discovering new acetylcholinesterase inhibitors. In addition to its important role in cholinergic neurotransmission, acetylcholinesterase also participates in other functions related to neuronal development, differentiation, adhesion and amyloid-β processing. Acetylcholinesterase accelerates amyloid-β aggregation and this effect is sensitive to peripheral anionic site blockers. Both features have lead to the development of dual inhibitors of both catalytic active and peripheral anionic sites. These compounds are promising disease-modifying Alzheimer’s disease drug candidates. On the other hand, due to the pathological complexity of Alzheimer’s disease, multifunctional molecules with two or more complementary biological activities may represent an important advance for the treatment of this disease.