Disability and Its Prevalence and Cause in Northwestern Ethiopia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
20210714 Access Snapshot- Tigray Region June 2021 V2
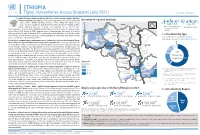
ETHIOPIA Tigray: Humanitarian Access Snapshot (July 2021) As of 31 July 2021 The conflict in Tigray continues despite the unilateral ceasefire announced by the Ethiopian Federal Government on 28 June, which resulted in the withdrawal of the Ethiopian National Overview of reported incidents July Since Nov July Since Nov Defense Forces (ENDF) and Eritrea’s Defense Forces (ErDF) from Tigray. In July, Tigray forces (TF) engaged in a military offensive in boundary areas of Amhara and Afar ERITREA 13 153 2 14 regions, displacing thousands of people and impacting access into the area. #Incidents impacting Aid workers killed Federal authorities announced the mobilization of armed forces from other regions. The Amhara region the security of aid Tahtay North workers Special Forces (ASF), backed by ENDF, maintain control of Western zone, with reports of a military Adiyabo Setit Humera Western build-up on both sides of the Tekezi river. ErDF are reportedly positioned in border areas of Eritrea and in SUDAN Kafta Humera Indasilassie % of incidents by type some kebeles in North-Western and Eastern zones. Thousands of people have been displaced from town Central Eastern these areas into Shire city, North-Western zone. In line with the Access Monitoring and Western Korarit https://bit.ly/3vcab7e May Reporting Framework: Electricity, telecommunications, and banking services continue to be disconnected throughout Tigray, Gaba Wukro Welkait TIGRAY 2% while commercial cargo and flights into the region remain suspended. This is having a major impact on Tselemti Abi Adi town May Tsebri relief operations. Partners are having to scale down operations and reduce movements due to the lack Dansha town town Mekelle AFAR 4% of fuel. -
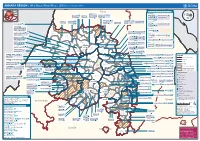
AMHARA REGION : Who Does What Where (3W) (As of 13 February 2013)
AMHARA REGION : Who Does What Where (3W) (as of 13 February 2013) Tigray Tigray Interventions/Projects at Woreda Level Afar Amhara ERCS: Lay Gayint: Beneshangul Gumu / Dire Dawa Plan Int.: Addis Ababa Hareri Save the fk Save the Save the df d/k/ CARE:f k Save the Children:f Gambela Save the Oromia Children: Children:f Children: Somali FHI: Welthungerhilfe: SNNPR j j Children:l lf/k / Oxfam GB:af ACF: ACF: Save the Save the af/k af/k Save the df Save the Save the Tach Gayint: Children:f Children: Children:fj Children:l Children: l FHI:l/k MSF Holand:f/ ! kj CARE: k Save the Children:f ! FHI:lf/k Oxfam GB: a Tselemt Save the Childrenf: j Addi Dessie Zuria: WVE: Arekay dlfk Tsegede ! Beyeda Concern:î l/ Mirab ! Concern:/ Welthungerhilfe:k Save the Children: Armacho f/k Debark Save the Children:fj Kelela: Welthungerhilfe: ! / Tach Abergele CRS: ak Save the Children:fj ! Armacho ! FHI: Save the l/k Save thef Dabat Janamora Legambo: Children:dfkj Children: ! Plan Int.:d/ j WVE: Concern: GOAL: Save the Children: dlfk Sahla k/ a / f ! ! Save the ! Lay Metema North Ziquala Children:fkj Armacho Wegera ACF: Save the Children: Tenta: ! k f Gonder ! Wag WVE: Plan Int.: / Concern: Save the dlfk Himra d k/ a WVE: ! Children: f Sekota GOAL: dlf Save the Children: Concern: Save the / ! Save: f/k Chilga ! a/ j East Children:f West ! Belesa FHI:l Save the Children:/ /k ! Gonder Belesa Dehana ! CRS: Welthungerhilfe:/ Dembia Zuria ! î Save thedf Gaz GOAL: Children: Quara ! / j CARE: WVE: Gibla ! l ! Save the Children: Welthungerhilfe: k d k/ Takusa dlfj k -

Ethiopia: Amhara Region Administrative Map (As of 05 Jan 2015)
Ethiopia: Amhara region administrative map (as of 05 Jan 2015) ! ! ! ! ! ! ! ! ! ! Abrha jara ! Tselemt !Adi Arikay Town ! Addi Arekay ! Zarima Town !Kerakr ! ! T!IGRAY Tsegede ! ! Mirab Armacho Beyeda ! Debark ! Debarq Town ! Dil Yibza Town ! ! Weken Town Abergele Tach Armacho ! Sanja Town Mekane Berhan Town ! Dabat DabatTown ! Metema Town ! Janamora ! Masero Denb Town ! Sahla ! Kokit Town Gedebge Town SUDAN ! ! Wegera ! Genda Wuha Town Ziquala ! Amba Giorges Town Tsitsika Town ! ! ! ! Metema Lay ArmachoTikil Dingay Town ! Wag Himra North Gonder ! Sekota Sekota ! Shinfa Tomn Negade Bahr ! ! Gondar Chilga Aukel Ketema ! ! Ayimba Town East Belesa Seraba ! Hamusit ! ! West Belesa ! ! ARIBAYA TOWN Gonder Zuria ! Koladiba Town AMED WERK TOWN ! Dehana ! Dagoma ! Dembia Maksegnit ! Gwehala ! ! Chuahit Town ! ! ! Salya Town Gaz Gibla ! Infranz Gorgora Town ! ! Quara Gelegu Town Takusa Dalga Town ! ! Ebenat Kobo Town Adis Zemen Town Bugna ! ! ! Ambo Meda TownEbinat ! ! Yafiga Town Kobo ! Gidan Libo Kemkem ! Esey Debr Lake Tana Lalibela Town Gomenge ! Lasta ! Muja Town Robit ! ! ! Dengel Ber Gobye Town Shahura ! ! ! Wereta Town Kulmesk Town Alfa ! Amedber Town ! ! KUNIZILA TOWN ! Debre Tabor North Wollo ! Hara Town Fogera Lay Gayint Weldiya ! Farta ! Gasay! Town Meket ! Hamusit Ketrma ! ! Filahit Town Guba Lafto ! AFAR South Gonder Sal!i Town Nefas mewicha Town ! ! Fendiqa Town Zege Town Anibesema Jawi ! ! ! MersaTown Semen Achefer ! Arib Gebeya YISMALA TOWN ! Este Town Arb Gegeya Town Kon Town ! ! ! ! Wegel tena Town Habru ! Fendka Town Dera -

Vulnerability of Mountain Communities to Climate Change and Natural Resources Scarcity in Northwest Ethiopia: the Case of Debark Woreda
JOURNAL OF DEGRADED AND MINING LANDS MANAGEMENT ISSN: 2339-076X (p); 2502-2458 (e), Volume 6, Number 1 (October 2018): 1467-1482 DOI:10.15243/jdmlm.2018.061.1467 Research Article Vulnerability of mountain communities to climate change and natural resources scarcity in Northwest Ethiopia: the case of Debark Woreda Yohannes Belay Azene1, Menberu Teshome Zeleke2*, Addisu Baye Chekole3 1 Department of Geography and Environmental Studies, University of Gondar, Ethiopia, Email: [email protected], Cell phone +251918775038 2 Department of Geography and Environmental Studies, Debre Tabor University, Ethiopia, [email protected], Cell phone +251- 930295752; fax +25105814105833; Po Box 272, Debre Tabor, Ethiopia 3 Development and Environmental Management Studies, University of Gondar, Ethiopia, [email protected]. Cell phone +251918226801 *corresponding author: [email protected] Received 11 July 2018, Accepted 8 September 2018 Abstract: In recent decades, climate change causes distressful shocks upon the poor people’s natural resources and socio-economic processes from local up to global scales. The crisis is more severe in Ethiopia, where harsh ecological changes are frequent. Therefore, the objective of this study was to determine the vulnerability levels of rural communities to climate change and natural resources scarcity in Debark woreda, Northwest Ethiopia. Livelihood Vulnerability Index (LVI) and IPCC methods were used to analyze the data. The meteorological data reveal a declining precipitation trend by 61.13 mm in the past 31 years whilst maximum and minimum temperatures increased by 0.62 0C and 0.74 0C respectively. The LVI result indicates that the Debark community is highly vulnerable with land (0.59) and forest (0.57) scarcity.Water scarcity (0.50) and climate exposure (0.30) put them in a vulnerable class. -

Ethiopia: 3W - Health Cluster Ongoing Activities Map (As of 2 Feb 2016)
Ethiopia: 3W - Health Cluster Ongoing Activities map (as of 2 Feb 2016) ERITREA ☊11 Total Number of Partners Concern Concern Red Sea TIGRAY Saesie Tsaedaemba Tselemti Kola Concern SUDAN Concern Temben Concern Concern Concern Beyeda Debark Concern Dabat ACF Concern Concern Janamora Wegera ACF Concern SCI ACF Ziquala SCI Gulf of Sekota Aden SCI SCI AMREF ACF AMREF Elidar LVIA LVIA SCI Awra AMREF VSF-G SCI VSF-G SCI Kobo LVIA Gidan Ewa VSF-G SCI SCI AFAR Guba Chifra Delanta Lafto SCI AMREF AMHARA Habru LVIA IRC Concern VSF-G Guba Concern Kutaber Mile SCI Concern Concern RHB Concern AMREF Afambo DJIBOUTI Bati LVIA Goncha Concern Concern Concern VSF-G IRC Siso Enese Telalak Concern Concern Enarj Concern Dewe SCI IRC BENESHANGUL Enawga Enbise MSF-S Ayisha Sar Midir AMREF SCI IRC IRC IRC Sirba Concern LVIA Gewane Kurmuk Sherkole GUMU Abay Bulen Shebel Concern VSF-G Menge Bereta Wegde IRC IRC Concern SCI Homosha Afdem Erer SCI AMREF SCI IRC LVIA IRC Yaso AMREF Shinile VSF-G MSF-S Dembel IRC Bilidigilu IRC LVIA IRC Assosa Bambasi VSF-G IRC SCI IRC Agalometi Simurobi Gele'alo SCI Kamashi IRC Jarso Miesso MSF-S DIRE IRC CARE Bio Jiganifado DAWA IRC CARE Mieso Kersa Tulo CARE HARERI CARE ACF CARE Mesela ACF Girawa IRC Chiro ACF ACF DRSAOMALIA FT SOUTH SUDAN Zuria Bedeno ACF Anchar Wantawo ACF IRC ACF Aware ACF IRC IRC IRC ACF IRC IRC Makuey Itang Gambela Zuria Degehabur Gashamo Fik IRC IRC MSF-S MSF-S IRC Jore Abobo Akobo IRC IRC IRC Gunagado ACF Gog IRC IRC Shekosh IRC GAMBELA Godere SCI Mengesh Dima OROMIA IRC SOMALI IRC SCI Kebridehar ACF ACF Bona Guradamole Zuria MSF-S ACF SCI Aroresa Debeweyin Shilabo SNNPR Gode SCI Kochere Goro SCI SCI MSF-S Baqaqsa SCI SCI Kelafo Adadle SCI Mustahil SCI SCI Ferfer Legend Bare SCI International boundary INDIAN Regional boundary Agencies' locOaCtiEoAnNs and area of interventions are No. -

Sustainable Land Management Project Ii (Slmp-2)
Document of The World Bank Report No: PAD525 Public Disclosure Authorized INTERNATIONAL DEVELOPMENT ASSOCIATION PROJECT APPRAISAL DOCUMENT ON A PROPOSED CREDIT IN THE AMOUNT OF SDR 32.6 MILLION (US$50 MILLION EQUIVALENT) AND A PROPOSED GRANT Public Disclosure Authorized FROM THE GLOBAL ENVIRONMENT FACILITY TRUST FUND IN THE AMOUNT OF US$ 8.33 MILLION AND A PROPOSED GRANT FROM THE LEAST DEVELOPED COUNTRIES FUND TRUST FUND IN THE AMOUNT OF US$ 4.62 MILLION AND A PROPOSED GRANT FROM THE ETHIOPIA SUSTAINABLE LAND MANAGEMENT PROJECT TRUST FUND Public Disclosure Authorized IN THE AMOUNT OF US$ 42.65 MILLION TO THE FEDERAL DEMOCRATIC REPUBLIC OF ETHIOPIA FOR A SUSTAINABLE LAND MANAGEMENT PROJECT II (SLMP-2) October 29, 2013 Public Disclosure Authorized This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective September 30, 2013) Currency Unit = Ethiopia Birr Ethiopia Birr18.92 = US$1 US$1.53408 = SDR 1 FISCAL YEAR January 1 – December 31 ABBREVIATIONS AND ACRONYMS ADLI Agriculture Development-led Industrialization ATA Agricultural Transformation Agency BoA Bureau of Agriculture CBPWDG Community-Based Participatory Watershed Development Guidelines CPS Country Partnership Strategy CRGE Climate Resilient Green Economy CSA Climate-smart Agriculture CSO Civil Society Organization CWT Community Watershed Team DA Development Agent DPs Development Partners EIAR Ethiopian -

The 24Th Annual Research Conference Abstract Booklet
Wright State University CORE Scholar University of Gondar Research Conferences University of Gondar 6-2014 The 24th Annual Research Conference Abstract Booklet Nikki Lynn Rogers Wright State University - Main Campus, [email protected] Follow this and additional works at: https://corescholar.libraries.wright.edu/gondar_conference Part of the Agricultural and Resource Economics Commons, Agriculture Commons, Arts and Humanities Commons, Business Commons, Economics Commons, Medical Sciences Commons, and the Veterinary Medicine Commons Repository Citation Rogers, N. L. (2014). The 24th Annual Research Conference Abstract Booklet. https://corescholar.libraries.wright.edu/gondar_conference/2 This Conference Proceeding is brought to you for free and open access by the University of Gondar at CORE Scholar. It has been accepted for inclusion in University of Gondar Research Conferences by an authorized administrator of CORE Scholar. For more information, please contact [email protected]. UNIVERSITY OF GONDAR THE 24™ ANNUAL RESEARCH CONFERENCE ( JUNE 13-14, 2014 MAIN THEME: Addressing Socio-Economic Problems through Thematic and Team Based Research ABSTRACT BOOKLET GONDAR, ETHIOPIA I UNIVERSITY OF GONDAR THE 24Tn ANNUAL RESEARCH CONFERENCE JUNE 13-14, 2014 MAIN THEME: Addressing Socio-Economic Problems through Thematic and Team Based Research ABSTRACT BOOKLET GONDAR, ETHIOPIA Preface The 24th annual staff-student research conference of university of Gondar will be held on June 13 and 14, 2014 at a science Amba auditorium of the University. This year's annual research conference is special as the year marks the Diamond Jubilee of the University of Gondar. Drawing on the experiences we accumulated for six decades, we strive to realize the development and transformation of the country through research and community services. -

Profile of Dabat Health and Demographic Surveillance System / Dabat Research Center
PROFILE OF DABAT HEALTH AND DEMOGRAPHIC SURVEILLANCE SYSTEM / DABAT RESEARCH CENTER Dabat Health and Demographic Surveillance System Dabat Health and Demographic Surveillance System (HDSS), also called the Dabat Research Center (DRC), was established at Dabat District in 1996 by the then Gondar College of Medical Sciences. Currently the surveillance is being run by the College of Medicine and Health Sciences which is one of the colleges/faculties of the University of Gondar. Dabat district is one of the 21 districts in North Gondar Administrative Zone of Amhara Region in Ethiopia (Figure 1). According to the report published by the Central Statistical Agency in 2007, the district has an estimated total population of 145,458 living in 27 rural and 3 urban Kebeles (sub-districts). The altitude of the district ranges from about 1000 meters to over 2500 meters above sea level. The district population largely depends on subsistence agriculture economy. There are two health centers, three health stations, and twenty-nine health posts providing health services for the community. An all-weather road runs from Gondar town through Dabat to some towns of Tigray. Dabat town, the capital of Dabat District, is located approximately 821 km northwest of Addis Ababa and 75 kms north of Gondar town. Dabat district was initially selected purposively as a surveillance site for its unique three climatic conditions, namely Dega (high land and cold), Woina dega (mid land and temperate) and Kolla (low land and hot). The choice was made with the assumption that there would be differences in morbidity and mortality in the different climatic areas. -

Minority Rights Protection in the Amhara National Regional State: the Case of the Kemant People in North Gondar
MINORITY RIGHTS PROTECTION IN THE AMHARA NATIONAL REGIONAL STATE: THE CASE OF THE KEMANT PEOPLE IN NORTH GONDAR BY BELAY SHIBESHI AWOKE GRADUATE PROGRAMS FACULTY OF LAW, ADDIS ABABA UNIVERSITY ADDIS ABABA, ETHIOPIA JANUARY 2010 www.chilot.me GRADUATE PROGRAMS FACULTY OF LAW, ADDIS ABABA UNIVERSITY MINORITY RIGHTS PROTECTION IN THE AMHARA NATIONAL REGIONAL STATE: THE CASE OF THE KEMANT PEOPLE IN NORTH GONDAR BY BELAY SHIBESHI AWOKE APPROVED BY BOARD OF EXAMINERS: _______________________________ _______________________ ADVISOR SIGNATURE/DATE _______________________________ ________________________ EXTERNAL EXAMINER SIGNATURE/DATE _______________________________ ________________________ INTERNAL EXAMINER SIGNATURE/DATE www.chilot.me MINORITY RIGHTS PROTECTION IN THE AMHARA NATIONAL REGIONAL STATE: THE CASE OF THE KEMANT PEOPLE IN NORTH GONDAR BY BELAY SHIBESHI AWOKE ADVISOR TSEGAYE REGASSA A THESIS SUBMITTED TO THE GRADUATE PROGRAMS OF FACULTY OF LAW, ADDIS ABABA UNIVERSITY, IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF LAWS IN HUMAN RIGHTS (LL. M) ADDIS ABABA, ETHIOPIA JANUARY 2010 www.chilot.me Acknowledgements I would like to express my gratitude to those who have contributed a lot to this piece of work. In the first place , my gratitude goes to my advisor Ato Tsegaye Regassa, not only for his invaluable and constructive comments and suggestions throughout the work, but also for his willingness to be my advisor at a time when he was so busy advising so many students. In addition, he assisted me a lot by giving source materials relevant to the study. I thank him for all! Secondly, Dr. Salah Hammad deserves thanks for his financial contribution for the research, and Ato Getachew Assefa for making such arrangements. -

Multiagency and Multisectoral Rapid Need Assessment in North Gondar and West Tigray Zones Among Conflict Affected Idps and Host Communities
Multiagency and Multisectoral Rapid Need Assessment in North Gondar and West Tigray Zones Among Conflict Affected IDPs and Host Communities Figures: IDPs on Pre-assessment briefing in Addi Arikay, Tselimti and Beyada Woredas. January 2021 Ethiopia 1 | P a g e TABLE OF CONTENTS 1. INTRODUCTION ............................................................................................................................... 3 2. JOINT RAPID ASSESSMENT TEAM MEMBERS ....................................................................... 5 3. OBJECTIVE OF THE ASSESSMENT ............................................................................................ 7 4. METHODOLOGY ............................................................................................................................. 7 5. FINDINGS ........................................................................................................................................... 8 5.1 Situation overview ....................................................................................................................... 8 5.2 Water Supply, Sanitation and Hygiene (WASH) ................................................................... 11 5.3 Shelter and Non-Food Items (NFI) .......................................................................................... 12 5.4 Food Security ............................................................................................................................. 13 5.5 Health and Nutrition ................................................................................................................ -

Based Natural Resource Management in Wodebeyes
Action Oriented Training of Natural Resource Management Case Study of Community- Based Natural Resource Management in Wodebeyesus Village, Debaitilatgin Woreda, Ethiopia Research Report submitted to Larenstein University of Applied Sciences In Partial fulfillment of the Requirements for the Degree of Master of Development, specialization Training in Rural Extension and Transformation (TREAT) BY Habtamu Sahilu Kassa September 2008 Wageningen the Netherlands © Copyright Habtamu Sahilu Kassa, 2008. All rights reserved PERMISSION TO USE In presenting this research project in partial fulfillment of the requirements for a post graduate degree, I agree that the library of the university may make it freely available for inspection. I further agree that permission for copying of this research project in any manner, in whole or in part, for scholarly purpose may be granted by Larenstein Director of Research. It is understood that any copying or publication or use of this research project or parts thereof for financial gain shall not be allowed without my written permission. It is also understood that due recognition shall be given to me and the University in any scholarly use which may be made of any material in my research project. Requests for permission to copy or to make other use of material in this research project in whole or part should be addressed to: Director of Research Larenstein University of Professional Education P.O.Box9001 6880GB Velp The Netherlands Fax: 31 26 3615287 ii ACKNOWLEDGEMENT My sincere thanks is to the Amahara National Regional State and the Sida support program, who offered me to study my masters in development program in the Netherlands. -

Dabat Golmasa Site Profile 23 April 2021 Dabat Woreda, North Gondar Zone April 2021
Dabat Golmasa Site Profile 23 April 2021 Dabat Woreda, North Gondar Zone April 2021 Methodology To ensure that Site Profiles use the most accurate and up-to-date data available, IOM's SMS Team employs multiple methods such as KIIs, FGDs, regular service mapping/monitoring and the analysis of its Complaints and Feedback Mechanism. In addition, IOM's SMS team consults with various data sources from the Government, IDP Community, IDP Representatives, Cluster Coordinators & partners as well as other relevant actors at site and/or area level. Demographic information is sourced from IOM's DTM or the relevant Government authority, depending on availability. Sector Overview Sector Indicator Target Achieved Implementing Agencies Key Target IDP Committee(s) have been formed or IDPs meaningfully represented in Kebele Committee Yes Yes IOM . reached . % of women represented in Community Representation Structures 35% 45% IOM Community Feedback Mechanism is operational IOM . Yes Yes Target 50% . % of IDPs living in adequate shelter (i.e. shelters that provide protection and safety ) ≥ 90% 50% IOM, CRS reached or more 2 . Average no. square metres of covered space per person ≥ 3.5m 2 IOM, CRS Target less than . % of target households that received non-food items in the last 18 months 100% 37% CRS 50% reached . # of functional latrines available on site 94 20 IOM . # of persons per (functional) latrine < 20 93 IOM No data . Average water availabilty (# litres/person/day ) ≥ 15l 11 IOM . Hygiene kits distributed to target households in the last 6 months Yes Yes IOM . % of IDP children regularly attending primary school 100% 0% No actor .