The Humanitarian Operation Adamawa State Nigeria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Politics of History in Northern Nigeria
The Politics of History in Northern Nigeria Niels Kastfelt Centre of African Studies University of Copenhagen Paper presented to the Research Seminar of the African Studies Centre, Leiden, 27 April 2006 The Politics of History in Contemporary Africa In recent years there has been a growing interest in the political uses of history in Africa. It is difficult to tell whether there is today a greater or more explicit political use of history than before, but it is clear that the past as a political resource does attract a strong interest from politicians and others, and that this interest takes new and highly visible forms. In this paper I shall discuss the politics of history in northern Nigeria. The discussion is based on a local case from the Nigerian Middle Belt which will be interpreted in the light of two wider contexts, that of the African continent in general and that of the specific Nigerian context. The aim of the paper is therefore double, aiming both at throwing light on the continental debate on history and on contemporary Nigerian politics. The political use of history in contemporary Africa takes many forms and so does the scholarly study of it. Without pretending to cover the entire field some main forms may be identified: “Patriotic history”: In a series of fascinating studies Terence Ranger and others have called attention to the emergence of “patriotic history” in contemporary Zimbabwe1. Zimbabwean “patriotic history” is part of the so-called “Mugabeism” launched in recent years by the regime of Robert Mugabe. The core of Mugabeism is the special version of the past called patriotic history which is promoted systematically through television, radio, newspapers and in the schools. -
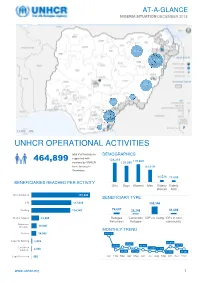
Unhcr Operational Activities 464,899
AT-A-GLANCE NIGERIA SITUATION DECEMBER 2018 28,280 388,208 20,163 1,770 4,985 18.212 177 Bénéficiaires Reached UNHCR OPERATIONAL ACTIVITIES total # of individuals DEMOGRAPHICS supported with 464,899 128,318 119,669 services by UNHCR 109,080 from January to 81,619 December; 34,825 of them from Mar-Apr 14,526 11,688 2018 BENEFICIARIES REACHED PER ACTIVITY Girls Boys Women Men Elderly Elderly Women Men Documentation 172,800 BENEFICIARY TYPE CRI 117,838 308,346 Profiling 114,747 76,607 28,248 51,698 Shelter Support 22,905 Refugee Cameroon IDPs in Camp IDPs in host Returnees Refugee community Awareness Raising 16,000 MONTHLY TREND Referral 14,956 140,116 Capacity Building 2,939 49,819 39,694 24,760 25,441 34,711 Livelihood 11,490 11,158 Support 2,048 46,139 37,118 13,770 30,683 Legal Protection 666 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec www.unhcr.org 1 NIGERIA SITUATION AT-A-GLANCE / DEC 2018 CORE UNHCR INTERVENTIONS IN NIGERIA UNHCR Nigeria strategy is based on the premise that the government of Nigeria assumes the primary responsibility to provide protection and assistance to persons of concern. By building and reinforcing self-protection mechanisms, UNHCR empowers persons of concern to claim their rights and to participate in decision-making, including with national and local authorities, and with humanitarian actors. The overall aim of UNHCR Nigeria interventions is to prioritize and address the most serious human rights violations, including the right to life and security of persons. -
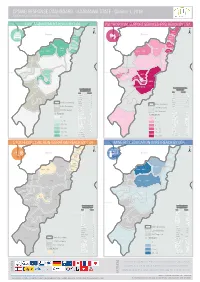
CPSWG RESPONSE DASHBOARD - ADAMAWA STATE - Quarter 1, 2019 Child Protection Sub Working Group, Nigeria
CPSWG RESPONSE DASHBOARD - ADAMAWA STATE - Quarter 1, 2019 Child Protection Sub Working Group, Nigeria YobeCASE MANAGEMENT REACH BY LGA PSYCHOSOCIALYobe SUPPORT SERVICES (PSS) REACH BY LGA 78% 14% Madagali ± Madagali ± Borno Borno Michika Michika 86% 10% 82% 16% Mubi North Mubi North Hong 100% Mubi South 5% Hong Gombi 100% 100% Gombi 10% 27% Mubi South Shelleng Shelleng Guyuk Song 0% Guyuk Song 0% 0% Maiha 0% Maiha Chad Chad Lamurde 0% Lamurde 0% Nigeria Girei Nigeria Girei 36% 81% 11% 96% Numan 0% Numan 0% Yola North Demsa 100% Demsa 26% Yola North 100% 0% Adamawa Fufore Yola South 0% Yola South 100% Fufore Mayo-Belwa Mayo-Belwa Adamawa Local Government Area Local Government (LGA) Target Area (LGA) Target LGA TARGET LGA TARGET Demsa 1,170 DEMSA 78 Fufore 370 Jada FUFORE 41 Jada Ganye 0 GANYE 0 Girei 933 GIREI 16 Gombi 4,085 State Boundary GOMBI 33 State Boundary Guyuk 0 GUYUK 0 LGA Boundary Hong 16,941 HONG 6 Ganye Ganye LGA Boundary Jada 0 JADA 0 Not Targeted Lamurde 839 LAMURDE 6 Not Targeted Madagali 6,321 MADAGALI 119 % Reach Maiha 2,800 MAIHA 12 % REACH Mayo-Belwa 0 0 MAYO - BELWA 0 0 Michika 27,946 Toungo 0% MICHIKA 232 Toungo 0% 1 - 36 Mubi North 11,576 MUBI NORTH 154 1 - 5 Mubi South 11,821 MUBI SOUTH 139 37 - 78 Numan 2,250 NUMAN 14 6 - 11 Shelleng 0 SHELLENG 0 79 - 82 12 - 16 Song 1,437 SONG 21 Teungo 25 83 - 86 TOUNGO 6 17 - 27 Yola North 1,189 YOLA NORTH 14 Yola South 2,824 87 - 100 YOLA SOUTH 47 28 - 100 SOCIO-ECONOMICYobe REINTEGRATION REACH BY LGA MINEYobe RISK EDUCATION (MRE) REACH BY LGA Madagali Madagali R 0% I 0% ± -

Rainfall and the Length of the Growing Season in Nigeria
INTERNATIONAL JOURNAL OF CLIMATOLOGY Int. J. Climatol. 24: 467–479 (2004) Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/joc.1012 RAINFALL AND THE LENGTH OF THE GROWING SEASON IN NIGERIA T. O. ODEKUNLE* Department of Geography, Obafemi Awolowo University, Ile-Ife, Nigeria Received 15 May 2003 Revised 8 December 2003 Accepted 16 December 2003 ABSTRACT This study examines the length of the growing season in Nigeria using the daily rainfall data of Ikeja, Ondo, Ilorin, Kaduna and Kano. The data were collected from the archives of the Nigerian Meteorological Services, Oshodi, Lagos. The length of the growing season was determined using the cumulative percentage mean rainfall and daily rainfall probability methods. Although rainfall in Ikeja, Ondo, Ilorin, Kaduna, and Kano appears to commence around the end of the second dekad of March, middle of the third dekad of March, mid April, end of the first dekad of May, and early June respectively, its distribution characteristics at the respective stations remain inadequate for crop germination, establishment, and development till the end of the second dekad of May, early third dekad of May, mid third dekad of May, end of May, and end of the first dekad of July respectively. Also, rainfall at the various stations appears to retreat starting from the early third dekad of October, early third dekad of October, end of the first dekad of October, end of September, and early second dekad of September respectively, but its distribution characteristics only remain adequate for crop development at the respective stations till around the end of the second dekad of October, end of the second dekad of October, middle of the first dekad of October, early October, and middle of the first dekad of September respectively. -

Nigeria Update to the IMB Nigeria
Progress in Polio Eradication Initiative in Nigeria: Challenges and Mitigation Strategies 16th Independent Monitoring Board Meeting 1 November 2017 London 0 Outline 1. Epidemiology 2. Challenges and Mitigation strategies SIAs Surveillance Routine Immunization 3. Summary and way forward 1 Epidemiology 2 Polio Viruses in Nigeria, 2015-2017 Past 24 months Past 12 months 3 Nigeria has gone 13 months without Wild Polio Virus and 11 months without cVDPV2 13 months without WPV 11 months – cVDPV2 4 Challenges and Mitigation strategies 5 SIAs 6 Before the onset of the Wild Polio Virus Outbreak in July 2016, there were several unreached settlements in Borno Borno Accessibility Status by Ward, March 2016 # of Wards in % Partially LGAs % Fully Accessible % Inaccessible LGA Accessible Abadam 10 0% 0% 100% Askira-Uba 13 100% 0% 0% Bama 14 14% 0% 86% Bayo 10 100% 0% 0% Biu 11 91% 9% 0% Chibok 11 100% 0% 0% Damboa 10 20% 0% 80% Dikwa 10 10% 0% 90% Gubio 10 50% 10% 40% Guzamala 10 0% 0% 100% Gwoza 13 8% 8% 85% Hawul 12 83% 17% 0% Jere 12 50% 50% 0% Kaga 15 0% 7% 93% Kala-Balge 10 0% 0% 100% Konduga 11 0% 64% 36% Kukawa 10 20% 0% 80% Kwaya Kusar 10 100% 0% 0% Mafa 12 8% 0% 92% Magumeri 13 100% 0% 0% Maiduguri 15 100% 0% 0% Marte 13 0% 0% 100% Mobbar 10 0% 0% 100% Monguno 12 8% 0% 92% Ngala 11 0% 0% 100% Nganzai 12 17% 0% 83% Shani 11 100% 0% 0% State 311 41% 6% 53% 7 Source: Borno EOC Data team analysis Four Strategies were deployed to expand polio vaccination reach and increase population immunity in Borno state SIAs RES2 RIC4 Special interventions 12 -
Assessment of Dispute Resolution Structures and Hlp Issues in Borno and Adamawa States, North-East Nigeria
ASSESSMENT OF DISPUTE RESOLUTION STRUCTURES AND HLP ISSUES IN BORNO AND ADAMAWA STATES, NORTH-EAST NIGERIA March 2018 1 The Norwegian Refugee Council is an independent humanitarian organisation helping people forced to flee. Prinsensgate 2, 0152 Oslo, Norway Authors Majida Rasul and Simon Robins for the Norwegian Refugee Council, September 2017 Graphic design Vidar Glette and Sara Sundin, Ramboll Cover photo Credit NRC. Aerial view of the city of Maiduguri. Published March 2018. Queries should be directed to [email protected] The production team expresses their gratitude to the NRC staff who contributed to this report. This project was funded with UK aid from the UK government. The contents of the document are the sole responsibility of the Norwegian Refugee Council and can under no circumstances be regarded as reflecting the position or policies of the UK Government. AN ASSESSMENT OF DISPUTE RESOLUTION STRUCTURES AND HLP ISSUES IN BORNO AND ADAMAWA STATES 2 Contents Executive summary ..........................................................................................5 Methodology ....................................................................................................................................................................8 Recommendations ......................................................................................................................................................9 1. Introduction ...............................................................................................10 1.1 Purpose of -

Ibadan, Nigeria by Laurent Fourchard
The case of Ibadan, Nigeria by Laurent Fourchard Contact: Source: CIA factbook Laurent Fourchard Institut Francais de Recherche en Afrique (IFRA), University of Ibadan Po Box 21540, Oyo State, Nigeria E-mail: [email protected] [email protected] INTRODUCTION: THE CITY A. URBAN CONTEXT 1. Overview of Nigeria: Economic and Social Trends in the 20th Century During the colonial period (end of the 19th century – agricultural sectors. The contribution of agriculture to 1960), the Nigerian economy depended mainly on agri- the Gross Domestic Product (GDP) fell from 60 percent cultural exports and on proceeds from the mining indus- in the 1960s to 31 percent by the early 1980s. try. Small-holder peasant farmers were responsible for Agricultural production declined because of inexpen- the production of cocoa, coffee, rubber and timber in the sive imports and heavy demand for construction labour Western Region, palm produce in the Eastern Region encouraged the migration of farm workers to towns and and cotton, groundnut, hides and skins in the Northern cities. Region. The major minerals were tin and columbite from From being a major agricultural net exporter in the the central plateau and from the Eastern Highlands. In 1960s and largely self-sufficient in food, Nigeria the decade after independence, Nigeria pursued a became a net importer of agricultural commodities. deliberate policy of import-substitution industrialisation, When oil revenues fell in 1982, the economy was left which led to the establishment of many light industries, with an unsustainable import and capital-intensive such as food processing, textiles and fabrication of production structure; and the national budget was dras- metal and plastic wares. -

Nigeria: Adamawa State Weekly Situation Report No
Nigeria: Adamawa State Weekly Situation Report No. 11 20 August 2021 This report is compiled by OCHA Nigeria in collaboration with humanitarian partners. HIGHLIGHTS • Some 297 people convicted for sexual and gender-based violence out of 774 reported cases between 2020 and the first half of 2021. • UNICEF is working with humanitarian partners to improve the quality of education and motivate teachers in Adamawa State SITUATION OVERVIEW 774 cases of sexual and gender-based violence reported between 2020 and the first half of 2021 Some 297 people were convicted for sexual and gender-based violence (SGBV) from 2020 to 2021 in Adamawa State out of about 774 cases reported. Due to the rising cases of GBV, the state Primary Healthcare Development Agency trained 50 participants across the 21 Local Government Areas (LGA) to prevent a further spike in cases. The capacity-building effort is expected to increase awareness of SGBV, detection of victims and suspects, reporting of suspects, and the management of victims undergoing trauma related to SGBV in communities across the state. Concern over the root cause of poor service delivery in the education sector UNICEF has raised concern over the challenges teachers face in the course of delivering quality education in Adamawa State. During the inauguration of a technical and vocational education program organised for teachers in Hong LGA the agency observed that low morale, poor welfare packages, and inequitable distribution of teachers are largely responsible for issues with education quality in the state. UNICEF plans to construct and rehabilitate 55 schools in Hong, Mubi North, Mubi South, Michika, Fufore, and Guyuk LGAs in Adamawa State to address some of the challenges. -

Patterns of Migration and Population Mobility in Sudanic West Africa: Evidence from Ancient Kano, C
Afrika Zamani, No. 24, 2016, pp. 11-30 © Council for the Development of Social Science Research in Africa & Association of African Historians 2017 (ISSN 0850-3079) Patterns of Migration and Population Mobility in Sudanic West Africa: Evidence from Ancient Kano, c. 800–1800 AD Akachi Odoemene* Abstract In the last three decades historians of migration in Europe and the Americas have increasingly criticised the idea of a ‘mobility transition’, which assumed that pre- modern societies were geographically fairly immobile, and that people only started to move in unprecedented ways from the nineteenth century onwards. This paper takes this perspective as a point of departure, and further presents evidence of remarkable population mobility from ancient Kano, taking a longue durée viewpoint. It reconstructs the nature and transformative roles of constant and consistent migration and population mobility in Kano, which ensured enormous social interactions within and between culturally distinct communities and led to socio-cultural changes. This earned Kano a reputation as an important, formidable and large medieval urban metropolis in Western Sudan. Thus, ancient Kano, like elsewhere in Sudanic Africa, had a rich history of massive and systematic migration and population mobility since the ninth century AD. Résumé Au cours des trois dernières décennies, les historiens de la migration en Europe et dans les Amériques ont de plus en plus critiqué l’idée d’une « transition de la mobilité », qui supposait que les sociétés prémodernes étaient géographiquement assez immobiles et que les populations n’ont commencé à se déplacer de manière inédite qu’à partir du dix-neuvième siècle. Partant de ce point de vue, le présent article présente des éléments attestant de la remarquable mobilité démographique dans l’ancienne Kano, sous une perspective de longue durée. -

Boko Haram Threatens to Cut Borno State from Nigeria
AFRICA Boko Haram Threatens to Cut Borno State from Nigeria OE Watch Commentary: The excerpted article from a Nigerian source discusses how Boko Haram’s current strategy risks cutting off northeastern Nigeria’s Borno State from the rest of the country. For several weeks in January, the group attacked the crucial Kano-Maiduguri highway connecting northern Nigeria’s largest city, Kano, with Borno’s capital, Maiduguri. The article points out that this is similar to the group’s strategy during the height of its territorial conquests in 2013-2014 in Borno, when it sought to render that highway and other roads inaccessible by bombing major bridges and occupying roadside villages. In terms of tactics, the article observes that Boko Haram often dresses in military attire, which makes drivers mistakenly believe the militants are the army. This enables the group to set Civilian Joint Force members patrol in Maiduguri. up fake checkpoints and capture or kill passengers and disrupt Source: C. Oduah (VOA) via Wikimedia, https://commons.wikimedia.org/wiki/File:Civilian_Joint_Force_members_patrol_in_Maiduguri.jpg, Public Domain traffic. In particular, the article states that Boko Haram has recently begun to target aid workers and Christians on the highways and released their execution videos through media channels affiliated with the Islamic State of Iraq and Syria (ISIS). In a worst case scenario, the article argues that the Kano-Maiduguri highway would have to be closed down, which would severely affect trade in northern Nigeria. This is why, apparently, Borno governor Babagana Zulum has urged the military to take all measures to secure that highway. -

Linguistics Diversity and Nigerian Languages Dynamism
Education & Science Journal of Policy Review and Curriculum Development | ESJPRCD Vol. 7, No. 1 ISSN Print: 2315-8425 | ISSN Online: 2354-1660 September, 2017 Linguistics Diversity and Nigerian Languages Dynamism 1Abubakar Tukur Liman & 2Bashiru Usman 1&2Department of English Language Education, College of Continuing Education, Adamawa State Polytechnic Yola- Adamawa State A b s t r a c t igeria seats about 450 languages on a land mass of less than 7percent of the total area of the African continent. This linguistic diversity explores the Ndynamism of language to adapt to situational constraints occasioned by regional/geographical, social, educational, and occupational domains, among others. This paper sets to examine the concept of linguistic diversity as it relates to the Nigerian experience. To achieve this, secondary data on the concept were reviewed. The study found that linguistic diversity is indeed a blessing which should be harnessed in Nigeria. Consequently, the paper recommends an aggressive use of mother tongues amongst Nigerian family members, school administrators, curriculum developers and teachers can also help the children in retaining and developing their mother tongues by initiating and implementing policies that encourage communication with the learners in such languages, government agencies like the National Orientation Agency, can also vigorously pursue projects aimed at communicating strong affirmative messages about the value of acquiring additional languages and emphasizing the fact that multilingualism is indeed a blessing and an important linguistic accomplishment. Keywords: Linguistic diversity, Language, Mother tongue, Multilingualism, Communication Corresponding Author: Abubakar Tukur Liman http://internationalpolicybrief.org/journals/international-scientific-research-consortium-journals/edu-and-sci-jrnl-of-policy-review-and-curriculum-dev-vol7-no1-september-2017 ESJPRCD | Page 66 Background to the Study Nigeria is a country with extreme linguistic fragmentation. -

Measuring Landcover Indicies of Adamawa State Using Remote Sensing and Geographic Information System (Gis) Techniques
FUTY Journal of the Environment, Vol. 4, No. 1, 2009 1 © School of Environmental Sciences, Federal University of Technology, Yola-Nigeria. ISSN 1597-8826 ((©© School of Environmental Sciences, Federal University of Technology, Yola-Nigeria. ISSN 1597-8826 MEASURING LANDCOVER INDICIES OF ADAMAWA STATE USING REMOTE SENSING AND GEOGRAPHIC INFORMATION SYSTEM (GIS) TECHNIQUES A. A. Musa1 and A. L. Tukur2 1Department of Surveying and Geoinformatics, Federal University of Technology, Yola 2Department of Geography, Federal University of Technology, Yola ABSTRACT Areas covered by marshlands, highlands and plains were needed in each local government area (LGA) as the bases for allocating funds to the LGAs. In recognition of the fact that ground survey techniques are very labor intensive, consumes a lot of time and generally inconveniencing, a GIS technique was adopted. Satellite images of the state were sub divided along the LGA boundaries. Highlands were located visually and digitized into vector polygons, and then by using the polygon tool of the GIS, areas covered by the polygons were determined. The image classification routine was used to isolate marshlands. By going to the ‘Raster Tools…’ menu and specifying the ‘Display/Edit Raster Attributes’ tool, the areas covered by the marshlands were also determined. Areas covered by plains on the other hand were determined indirectly. The area covered by highlands (already computed) was subtracted from the total area of the LGA by using manual qualitative deduction. Since highlands and plains are mutually exclusive, the result of the subtraction is the area covered by plains. It was observed that LGAs with the highest percentage of marshlands are those which R.Benue pass through.