Physiological Responses and Competitive Performance in Elite Synchronized Swimming
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Swimming As Play Gabor Csepregi
Document generated on 09/24/2021 4:20 p.m. Laval théologique et philosophique Swimming as Play Gabor Csepregi Volume 43, Number 2, juin 1987 URI: https://id.erudit.org/iderudit/400305ar DOI: https://doi.org/10.7202/400305ar See table of contents Publisher(s) Faculté de philosophie, Université Laval ISSN 0023-9054 (print) 1703-8804 (digital) Explore this journal Cite this article Csepregi, G. (1987). Swimming as Play. Laval théologique et philosophique, 43(2), 249–254. https://doi.org/10.7202/400305ar Tous droits réservés © Laval théologique et philosophique, Université Laval, This document is protected by copyright law. Use of the services of Érudit 1987 (including reproduction) is subject to its terms and conditions, which can be viewed online. https://apropos.erudit.org/en/users/policy-on-use/ This article is disseminated and preserved by Érudit. Érudit is a non-profit inter-university consortium of the Université de Montréal, Université Laval, and the Université du Québec à Montréal. Its mission is to promote and disseminate research. https://www.erudit.org/en/ Laval théologique et philosophique, 43, 2 (juin 1987) SWIMMING AS PLAY Gabor CSEPREGI "If there is magic on this planet, it is contained in water." Loren EISELY, The Immense Journey RÉSUMÉ — L'intention de cet essai est de mettre en relief quelques traits de la natation (et d'autres sports connexes) considérée comme une forme de jeu. Le mouvement ludique transforme Veau en un monde différent où le nageur se découvre une nouvelle identité, jouit de liberté et s'affranchit des soucis quotidiens. Ici encore, l'être humain peut trouver moyen, grâce au jeu, de satisfaire son désir constant de transcender le monde ordinaire naturel afin de donner plus de sens à sa vie. -

Synchronized Swimming Record Book Was Years: Second Season Written and Edited by Regina Verlengiere
2014 STANFORD SYNCHRO 2014 STANFORD SCHEDULE Date Event/Opponent Location Time Jan. 24 Lindenwood University St. Charles, Mo. TBD Jan. 25 Lindenwood University St. Charles, Mo. TBD Feb. 8 Incarnate Word Stanford, Calif. 12 p.m. Feb. 9 Incarnate Word Stanford, Calif. 9 a.m. Feb. 15 Florida & Lindenwood Gainesville, Fla. TBD Feb. 16 Florida Gainesville, Fla. TBD Feb. 22 Arizona Stanford, Calif. 3 p.m. Feb. 23 Arizona Stanford, Calif. 10 a.m. March 1 Arizona State Mesa, Ariz. TBD March 2 Western Regionals Mesa, Ariz. All Day March 20-22 U.S. Collegiate Nationals Oxford, Ohio All Day 2014 QUICK FACTS General Information Athletic Communications and Media Relations Location: Stanford, CA 94305-6150 Synchro Contact: Regina Verlengiere Synchro Facility: Avery Aquatics Center Email: [email protected] Enrollment: 15, 870 (6,999 undergraduates) Office Phone: (650)723-0996 Founded: 1891 Media Relations Office: (650) 723-4418 Nickname: Cardinal Athletics Website: www.gostanford.com Colors: Cardinal and White Athletic Director: Bernard Muir Media Information President: John Hennessy Interview requests for players and coaches must be coordinated with Sport Administrator: Brian Talbot the Stanford Athletics Communications office. Visit www.gostanford. com for news releases, player profiles, and updated schedules and Coaching Staff results. Sara Lowe (Stanford, 2008) Head Coach: Credits: The 2014 Stanford synchronized swimming record book was Years: Second Season written and edited by Regina Verlengiere. Past design, layout and pro- Assistant Coach: Megan Azebu (Santa Clara, 2012) duction by Maggie Oren, MB Design. Photoraphy by John Todd, Don Athletic Trainer: Scott Anderson Feria and Richard Ersted. Sports Performance Coach: Rachel Hayes Synchro Office Phone: (650) 724-2395 WWW.GOSTANFORD.COM 2014 SYNCHRONIZED SWIMMING RECORD BOOK 2014 STANFORD ROSTER From left to right: Isabella Park, Leigh Haldeman, Evelyna Wang, Megan Hansley, Mina Shah, Marisa Tashima and Carolyn Morrice. -
Synchronized Skating Teams 2020
Synchronized Skating Teams For Skaters in Basic 4 and Up! 2020 – 2021 Training Season Info *Please note: Due to the Global Pandemic, the Chicago Red Line is currently planning on hosting a “Training Only Season”. Under this plan, the season will not include competitions or travel, and will focus on skater development. IMPORTANT: 2020 – 2021 Training Season Info Due to the Global Pandemic, the Chicago Red Line is currently planning on hosting a “Training Only Season”. Under this plan, the season will not include competitions or travel, and will focus on skater development. This training season will allow us to: • Work on individual skills and drills, that do not include physical touching • Keep socially distant during practice • Build up the skaters’ individual strengths, which will strengthen the team, when it is able to resume normally. • At a reduced dues cost, will allow families who have been impacted financially by the pandemic, to continue participating in their team sport. • Have the coaches loosely choreograph an ‘unconnected’ performance program, that if restrictions loosen, the skaters will be able to perform in a competition or ice show. • If restrictions / precautions lift enough to allow us to attend a competition, to collect fees at that time. Important Note about age: For our younger team, we are requiring at least an age of 7, as we believe that most 7 year olds will be able to understand the importance of Social Distancing on the ice, to maintain everyone’s safety. If you believe your child will struggle with maintaining physical distance from their teammates, we ask that you wait to join us until next season, when we hope to resume normal team practices. -
TDSSA Appendix 1
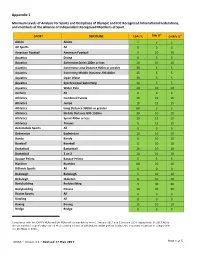
Appendix 1 Minimum Levels of Analysis for Sports and Disciplines of Olympic and IOC Recognized International Federations, and members of the Alliance of Independent Recognized Members of Sport 4 4 SPORT DISCIPLINE ESAs % GHs % GHRFs % Aikido Aikido 5 5 5 Air Sports All 0 0 0 American Football American Football 5 10 10 Aquatics Diving 0 5 5 Aquatics Swimming Sprint 100m or less 10 10 10 Aquatics Swimming Long Distance 800m or greater 30 5 5 Aquatics Swimming Middle Distance 200‐400m 15 5 5 Aquatics Open Water 30 5 5 Aquatics Synchronized Swimming 10 5 5 Aquatics Water Polo 10 10 10 Archery All 0 0 0 Athletics Combined Events 15 15 15 Athletics Jumps 10 15 15 Athletics Long Distance 3000m or greater 60 5 5 Athletics Middle Distance 800‐1500m 30 10 10 Athletics Sprint 400m or less 10 15 15 Athletics Throws 5 15 15 Automobile Sports All 5 0 0 Badminton Badminton 10 10 10 Bandy Bandy 5 10 10 Baseball Baseball 5 10 10 Basketball Basketball 10 10 10 Basketball 3 on 3 10 10 10 Basque Pelota Basque Pelota 5 5 5 Biathlon Biathlon 60 10 10 Billiards Sports All 0 0 0 Bobsleigh Bobsleigh 5 10 10 Bobsleigh Skeleton 0 10 10 Bodybuilding Bodybuilding 5 30 30 Bodybuilding Fitness 10 30 30 Boules Sports All 0 0 0 Bowling All 0 0 0 Boxing Boxing 15 10 10 Bridge Bridge 0 0 0 4 Compliance with the GHRFs MLAs and GH MLAs will be mandatory from 1 January 2017 and 1 January 2018 respectively. -

A History of Synchronized Swimming1
Wir empfehlen Ihnen, auf einem Blatt jeweils zwei Seiten dieses Artikels nebeneinander auszudrucken. We recommend that you print two pages of this article side by side on one sheet. Body Politics 2 (2014), Heft 3, S. 21-38 A History of Synchronized Swimming1 Synthia Sydnor 2 Proem No fish, no fowl, nor other creature whatsoever that hath any living or being, wither in the depth of the sea or superficies of the water, swimmeth 3 upon his back, man only excepted. From articles-fragments-scrounging-primary evidence-sources-refer- ences-facts-propaganda4 (the above quotation dated 1595 is the earliest of my fragments), I assemble here a history of synchronized swimming, or at the least, I compose an essay in which I ponder synchronized swimming at the same time as I tread against the flow5 of the established methodology of “sport history” Historians take unusual pains to erase the elements in their work which reveal their grounding in a particular time and place, their preferences in a controversy – the unavoidable obstacles of their passions. … The genealogist … must be able to recognize the events of history, its jolts, its surprises, its unsteady victories and unpalatable defeats – the basis of all beginnings, atavisms and heredities. … Genealogy does not resemble the evolution of a species and does not map the destiny of a people. [It] identif[ies] the accidents, the minute deviations – or conversely – the complete reversals – the errors, the false appraisals, and the faulty calculations that gave birth to those things that continue to exist and have value for us.6 On genealogy, historical methodology, “items” and “pondering,” I am influenced by Walter Benjamin. -
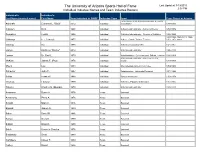
The University of Arizona Sports Hall of Fame Last Updated: 3/19/2015 2:58 PM Individual Inductee Names and Team Inductee Rosters
The University of Arizona Sports Hall of Fame Last Updated: 3/19/2015 2:58 PM Individual Inductee Names and Team Inductee Rosters Individual's Individual's Last Name (married name) First Name Year Inducted in SHOF Inductee Type Sport Years Played at Arizona Letterwinner & UA Athletics Facilities & Events Ashcraft Clarence L. "Stub" 2012 Individual Coordinator 1947-1982 Clausen Dick 1998 Individual Athletics Administrator - Athletics Director 1958-1972 Dempsey Cedric 1994 Individual Athletics Administrator - Director of Athletics 1982-1883 1924-1926, 1926-1941, 1926- Gibbings F.T. (Limey) 1977 Individual Athlete, Coach, Trainer, Teacher 1951, 1951-1969 Gittings Ina 1976 Individual Athletics Association (W) 1921-1951 Larose Kathleen "Rocky" 2014 Individual Athletics Administrator 1980-2013 Larson Dr. Emil L. 1979 Individual Administration - Commissioner, Official, Teacher 1926-1968 Athletics Administrator - Athletics Director, McKale James F. (Pop) 1976 Individual Coach 1914-1957 Myers Lou 1984 Individual Intercollegiate Athletic Committee 1959-1980 Schaefer John P. 1997 Individual Administraion - University President 1971-1982 Soltys Frank W. 1988 Individual Sports Information 1959-1979 Thomas Edward 1990 Individual Athletics - Equipment Manager 1951-1985 Tribolet Charles S. (Bumps) 1978 Individual Athletics Administrator 1928-1978 Anderson Burce H. 1976 Team Baseball Armstrong Perry A. 1976 Team Baseball Arnold Mark C. 1976 Team Baseball Bagnall James A. 1980 Team Baseball Baker David M. 1986 Team Baseball Bargar Greg R. 1980 Team Baseball Billard Brian R. 1980 Team Baseball Bolek Kenneth Charles 1976 Team Baseball Bradshaw Scott 1980 Team Baseball Candaele Casey T. 1980 Team Baseball Carley David 1986 Team Baseball The University of Arizona Sports Hall of Fame Last Updated: 3/19/2015 2:58 PM Individual Inductee Names and Team Inductee Rosters Individual's Individual's Last Name (married name) First Name Year Inducted in SHOF Inductee Type Sport Years Played at Arizona Carlsen Robin A. -

Sport Development Awards : Award Recipients 1987-2019
Sport Development Awards Award Recipients 1987-2019 Don Watts Coach Developer Award Coach Developer Award - Sport 2013 Don McGavern – Multi Sport 2013 Phyllis Sadoway – Ringette 2015 Leigh Gouldie – Multi Sport 2015 Beth Veale – Ringette 2017 Jim Loughlin – Multi Sport 2017 Kelly Wills – Artistic Gymnastics 2019 Susan Yackulic – Multi Sport 2019 Jacqueline Cool - Swimming Coaching Recognition Award 1987 1988 Dave Johnson – Swimming John Cannon - Athletics Ian Paton – Squash George Kingston - Hockey Perry Pearn – Hockey Glenn Purych - Wrestling Deryk Snelling – Swimming Yosh Senda - Judo Cathy Walsh – Wheelchair Stuart Brown - Soccer 1989 1990 Peter Connellan – Football Herb Flewwelling - Diving Michael Jiranek - Figure Skating Max Gartner - Alpine Skiing Carole Larsen – Curling Les Gramantik - Athletics Leslie Sproule - Synchronized Swimming Paul Hortie* - Boxing Milan Uremovic – Rowing Donna Rudakas - Basketball 1991 1992 Greg Folk - Figure Skating Ritch Braun - Athletics Bruce Rimmer - Alpine Skiing Bert Goldberger - Soccer Garry Smith - Wheelchair Basketball Dru Marshall - Field Hockey Sandy Teel - Synchronized Swimming Jan Ullmark - Figure Skating Sharon Trenaman - Squash April 2021 Classification: Public Coaching Recognition Award 1995 1997 Michelle Callkins - Synchronized Swimming Lynne Koper - Figure Skating Ewan Ferrier - Bowhunting and Archery Krysztof Machnowski - Sailing Patricia Foster – Rollerskating Jules Owchar - Colleges Winnifred Silverthorne - Figure Skating Channarong Ratanseangsuang - Badminton Jack Walters - Speed -

BEST Synkrolovers Camp 2020
BEST Synkrolovers Camp 2020 Colònia Sant Jordi - Mallorca OLYMPIC EDITION www.bestcentresports.com · [email protected] INDEX 1) INTRODUCTION .................................................... 3 WELCOME! 2) FAMILY v RESIDENTIAL OPTION ........................... 4 3) GENERAL INFORMATION ...................................5 After over a decade of running highly successful Family Swim Holidays and • Camp dates ........................................................ 5 our residential swimming program, CAMP Mallorca, we have collaborated • Location ............................................................... 5 with Synkrolovers to create something just as special for synchro swimmers. • Travel .................................................................... 5 We are very proud to present our third edition of our BEST Synkrolovers Camp. 4) The BEST Centre .................................................. 6 • BEST Synkrolovers Camp Staff .................... 6 For one week this August, young synchro swimmers from across the globe will • The Pool ............................................................... 7 have the unmissable opportunity to train in one of the worlds best swimming • Gym ...................................................................... 7 facilities, with Olympic Synchro star and head coach of the U.S. senior national team - Andrea Fuentes. • Address .................................................................7 5) ACCOMMODATION ............................................ 8 • Hotel Romántica ........................................... -

Destination Reiseziel Gourmet Ona Carbonell
The Spanish Lifestyle Magazine for the International Clients of Banco Sabadell Das Spanische Lifestyle Magazin für Internationale Kunden von Banco Sabadell Spring / Frühling 2015 Number / Heft 62. 2€ Destination Reiseziel Trends Tendenzen Gourmet Menorca, a Paradise of Tranquility Spanish cinematographic locations Becoming flexitarian Menorca, ein Paradies der Ruhe Die bekanntesten Filmorte Spaniens Flexitarier werden p.18 p.24 p.32 Ona Carbonell A world champion and Olympic medalist in synchronized swimming Eine Weltmeisterin und Olympiasiegerin im Synchronschwimmen p.12 62 Spring/Frühling 2015 Spring/Frühling INDEX 06 08 12 TRENDY GADGETS PEOPLE INTERVIEW A glance at the Four outstanding An interview with the synchronized latest gadgets Spanish personalities swimmer Ona Carbonell Ein Blick in die Vier herausragende Ein Gespräch mit die synchronisiert neuesten Gadgets spanische Persönlichkeiten Schwimmer Ona Carbonell Club Prestige Magazine publisher herausgeber www.factoriaprisma.com print druck Monterreina Área Empresarial Andalucía C/ Cabo de Gata, 1-3 Sector 2 28320 Pinto MADRID TEL: +34 916 213 060 FAX: +34 916 213 031 MOVIL: +34 627 47 30 45 www.monterreina.com Club Prestige Magazine is published quarterly and is distributed free to Banco Sabadell customers. The views and opinions expressed in this magazine are not necessarily those of Banco Sabadell or Club Prestige Magazine, nor does the inclusion of any advertisement mean that the publisher endorses the company concerned or its products. No part of this magazine including texts, photographs and graphics may be reproduced in any way without prior written consent of Banco Sabadell. SabadellSolbank is a registered Trade Mark of Banco de Sabadell S.A Das Club Prestige Magazine erscheint vierteljährlich und wird kostenlos an Kunden der Banco Sabadell verteilt. -

Len European Championships Aquatic Finalists
LEN EUROPEAN CHAMPIONSHIPS AQUATIC FINALISTS 1926-2016 2 EUROPEAN CHAMPIONSHIPS GLASGOW 2ND-12TH AUGUST 2018 SWIMMING AT TOLLCROSS INTERNATIONAL SWIMMING CENTRE DIVING AT ROYAL COMMONWEALTH POOL, EDINBURGH ARTISTIC (SYNCHRONISED) SWIMMING AT SCOTSTOUN SPORTS CAMPUS, GLASGOW OPEN WATER SWIMMING IN LAKE LOMOND 2 Contents Event Page Event Page European Championship Venues 5 4x100m Freestyle Team- Mixed 123 4x100m Medley Team – Mixed 123 50m Freestyle – Men 7 100m Freestyle – Men 9 Open Water Swimming – Medals Table 124 200m Freestyle – Men 13 400m Freestyle – Men 16 5km Open Water Swimming – Men 125 800m Freestyle – Men 20 10km Open Water Swimming – Men 126 1500m Freestyle – Men 21 25km Open Water Swimming – Men 127 50m Backstroke – Men 25 5km Open Water Swimming – Women 129 100m Backstroke – Men 26 10km Open Water Swimming – Women 132 200m Backstroke – Men 30 25km Open Water Swimming – Women 133 50m Breaststroke – Men 34 Open Water Swimming – Team 5km Race 136 100m Breaststroke – Men 35 200m Breaststroke – Men 38 Diving – Medals Table 137 50m Butterfly – Men 43 1m Springboard – Men 138 100m Butterfly – Men 44 3m Springboard – Men 140 200m Butterfly – Men 47 3m Springboard Synchro - Men 143 10m Platform – Men 145 200m Individual Medley – Men 50 10m Platform Synchro – Men 148 400m Individual Medley – Men 54 1m Springboard – Women 150 4x100m Freestyle Team – Men 58 3m Springboard – Women 152 4x200m Freestyle Team – Men 61 3m Springboard Synchro – Women 155 4x100m Medley Team – Men 65 10m Platform – Women 158 10m Platform Synchro – Women 161 -

Swimming Swimming
SYNCHRONIZED SWIMMING SWIMMING www.bestswimcentre.com [email protected] Mallorca 2016 INDEX CAMP MALLORCA PRESENTATION • Presentation ............................................. p. 2 • Focus ......................................................... p. 2 1) STAFF............................................................ p. 3 After over a decade of running highly successful Family 2) GENERAL INFORMATION ............................. p. 4 Swim Holidays in Mallorca, the BEST Centre is proud • Accommodation ....................................... p. 5 to launch its CAMP MALLORCA elite sports camps. • Meals ........................................................ p. 5 • Food Allergies ........................................... p. 5 • Multiple Camps ........................................ p. 5 CAMP Mallorca is designed to allow young 3) SPORTS FACILITIES swimmers and synchronized swimmers to stay • BEST Centre .............................................p. 6 in a safe and healthy environment and practice • Blau Colonia Sant Jordi H.R. ...................p. 6 the sport they love. 4) BLUEWATER HOTEL .....................................p. 7 5) THE TOWN ..................................................p. 8 • Transportation ..........................................p. 8 • Addresses ................................................p. 8 6) SURROUNDING AREA .................................p. 9 • National Park of Cabrera .........................p. 9 7) ITINERARIES & PRICES • Swimming Camp ....................................p. 10 • Synchronized -

Marga Crespí
• MARGA CRESPÍ • OBJETIVOS • PROGRAMACIÓN • INFORMACIÓN TÉCNICA INSTALACIONES • SELECCIÓN ESPAÑOLA RFEN DE NATACIÓN SINCRONIZADA • RESUMEN FOTOGRÁFICO MARGA CRESPÍ • Margalida Crespí nació en Palma de Mallorca, el 15 de agosto de 1990. • A los 6 años de edad, empezó a practicar la natación sincronizada en el PM Son Moix con el Club Mediterránea, en el que se fue formando y comenzó a competir y cosechar un éxito tras otro con tan solo 9 años. • Un día en un campeonato se fijó en ella la seleccionadora nacional Anna Tarrés y comenzó su andadura en Barcelona junto con el resto del equipo nacional. Ha tenido el privilegio de entrenar junto a Gemma Mengual, uno de sus referentes a seguir. • Miembro de la selección nacional de natación sincronizada, entre sus grandes éxitos cabe destacar las dos medallas de plata del campeonato de Europa celebrado en Budapest en el 2010 y la medalla de bronce de los campeonatos del Mundo celebrados en julio de 2011 en Shangai. OBJETIVOS • Dedicar la nueva instalación municipal a Marga Crespí en reconocimiento por su carrera deportiva, y que esto sirva como motivo de impulso y ánimo de cara al futuro, dada la gran exigencia y sacrificio que requiere la natación sincronizada. • Poder dar un nuevo impulso al deporte y favorecer la práctica deportiva de todos los vecinos y vecinas de Son Ferriol, así como del conjunto de los ciudadanos y ciudadanas de Palma. • Fomentar la práctica de la natación y en especial de la natación sincronizada en Baleares. • Transmitir e inculcar valores como el trabajo en equipo, respeto, exigencia y esfuerzo, compañerismo, responsabilidad y compromiso, e integridad.