Board of Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
2014-2015 Annual Report
ANNUAL REPORT TO MEMBERS 2014-2015 AND ANNUAL BUSINESS MEETING Friday, May 8, 2015 Greater Sudbury, Ontario FONOM ANNUAL BUSINESS MEETING A G E N D A Friday, May 8, 2015, 8:00 am Main Ballroom, Holiday Inn Hotel 1696 Regent Street Greater Sudbury, ON 1. Approval of / Additions to Agenda 2. Introduction of Executive 3. President’s Report 4. Financial Report (resolution required) 5. Approval of Minutes of Meeting Friday, May 9, 2014 (resolution required) 6. Resolutions 7. Adjourn 2 FONOM BOARD OF DIRECTORS PRESIDENT TELEPHONE (705) REPRESENTING Mayor Alan Spacek Mun Tel 337-4250 District of Town of Kapuskasing Mun Fax 335-5103 Cochrane 88 Riverside Drive Kapuskasing, ON P5N 1B3 Email: [email protected] PAST PRESIDENT Councillor S. Mac Bain Mun Tel 474-0400 City of North Bay City of North Bay Mun Fax 495-4353 PO Box 360 200 McIntyre St. E. North Bay, ON P1B 8H8 Email: [email protected] FIRST VICE PRESIDENT Councillor Danny Whalen Mun Tel 672-3363 District of City of Temiskaming Shores Mun Fax 672-3200 Timiskaming 325 Farr Drive, Box 2050 Haileybury, ON P0J 1C0 Email : [email protected] SECOND VICE PRESIDENT Mayor Brian Bigger Mun Tel 674-4455 City of Greater City of Greater Sudbury Ext. 2514 Sudbury PO Box 5000, Stn A Mun Fax 673-3096 200 Brady Street Sudbury, ON P3A 5P3 Email: [email protected] DIRECTORS (in alphabetical order by surname) Mayor Steven Black Mun Tel 360-2611 City of Timmins City of Timmins Mun Fax 360-2690 220 Algonquin Blvd. East Timmins, ON P1B 8H8 Email: [email protected] Reeve Austin -

AMO Secretary Treasurer's Report on Nominations
Report of the Secretary-Treasurer On Nominations to the 2016 – 2018 AMO Board of Directors June 30, 2016 June 30, 2016 To: Member Municipalities It is my pleasure to submit a copy of my report on the candidates standing for election for the 2016 – 2018 AMO Board of Directors, as confirmed by the Returning Officer. The Returning Officer has confirmed candidates against the nomination requirements and processes. Elections will be held on: Monday, August 15, 2016, 12:00 – 5:00 p.m., and Tuesday, August 16, 2016, 8:30 a.m. – 12:30 p.m. Location: Augustus Ballroom Foyer, Caesars Hotel Windsor All elected officials from member municipalities in good standing with the Association are eligible to vote. Please note that voting delegates have until 4:00 p.m. Friday, July 15, 2016 to identify or change their caucus, if they have already registered for the conference. After this date, absolutely no changes are permitted to the voting delegates list. This rule is strictly enforced. Please note that the Heads of the following municipal groups are automatically appointed to the appropriate Caucus of the AMO Board: • L’Association française des municipalités de l’Ontario (AFMO) • Eastern Ontario Wardens’ Caucus (EOWC) • Federation of Northern Ontario Municipalities (FONOM) • Northern Ontario Municipal Association (NOMA) • Large Urban Mayors’ Caucus of Ontario (LUMCO) • Mayors & Regional Chairs of Ontario of Single Cities and Regions (MARCO) • Ontario Small Urban Municipalities (OSUM) • Rural Ontario Municipal Association (ROMA) • Western Ontario Wardens -

March 19, 2015 MEMORANDUM TO: Ontario Works Administrators FROM: Richard Steele Assistant Deputy Minister SUBJECT: Additional Fu
Ministry of Community Ministère des Services and Social Services sociaux et communautaires Assistant Deputy Minister Sous-ministre adjoint Social Assistance Division des opérations Operations Division relatives à l'aide sociale Hepburn Block, 6th floor Édifice Hepburn, 6e étage 80 Grosvenor Street 80, rue Grosvenor Toronto ON M7A 1E9 Toronto (Ontario) M7A 1E9 March 19, 2015 MEMORANDUM TO: Ontario Works Administrators FROM: Richard Steele Assistant Deputy Minister SUBJECT: Additional Funding for SAMS Implementation I am writing to inform you that the ministry will be providing an additional $5 million in one-time funding in this fiscal year to assist Consolidated Municipal Service Managers (CMSMs) and District Social Services Administration Boards (DSSABs) with costs related to the implementation of the Social Assistance Management System (SAMS). The additional funding comes from within the Ministry’s existing social assistance administration budget. This funding is in recognition of the tremendous efforts being made to implement SAMS, and brings the cumulative amount of provincial funding provided to support the operational cost of SAMS implementation to $15 million – $5 million anticipated and provided prior to implementation and an additional $10 million provided post- implementation. The funding is 100 per cent provincial with no cost-sharing requirement for costs incurred up to March 31, 2015. Distribution of the $5 Million in One-Time Funding (100% Provincial): The new funding will be distributed in the same fashion as the previous funding. A base of $50,000 will be provided to all 47 CMSMs and DSAABs, with the balance of the $5 million being distributed based on each delivery agent’s share of the Ontario Works caseload. -

Stand Up, Fight Back!
admin.iatse-intl.org/BulletinRegister.aspx Stand Up, Fight Back! The Stand Up, Fight Back campaign is a way for Help Support Candidates Who Stand With Us! the IATSE to stand up to attacks on our members from For our collective voice to be heard, IATSE’s members anti-worker politicians. The mission of the Stand Up, must become more involved in shaping the federal legisla- Fight Back campaign is to increase IATSE-PAC con- tive and administrative agenda. Our concerns and inter- tributions so that the IATSE can support those politi- ests must be heard and considered by federal lawmakers. cians who fight for working people and stand behind But labor unions (like corporations) cannot contribute the policies important to our membership, while to the campaigns of candidates for federal office. Most fighting politicians and policies that do not benefit our prominent labor organizations have established PAC’s members. which may make voluntary campaign contributions to The IATSE, along with every other union and guild federal candidates and seek contributions to the PAC from across the country, has come under attack. Everywhere from Wisconsin to Washington, DC, anti-worker poli- union members. To give you a voice in Washington, the ticians are trying to silence the voices of American IATSE has its own PAC, the IATSE Political Action Com- workers by taking away their collective bargaining mittee (“IATSE-PAC”), a federal political action commit- rights, stripping their healthcare coverage, and doing tee designed to support candidates for federal office who away with defined pension plans. promote the interests of working men and women. -

City Council Agenda
CITY COUNCIL AGENDA City Council Meeting Tuesday, September 27, 2016 Council Chamber, Tom Davies Square 6:00 p.m. OPEN SESSION, COUNCIL CHAMBER Council and Committee Meetings are accessible. For more information regarding accessibility, please call 3-1-1 or email [email protected]. MOMENT OF SILENT REFLECTION ROLL CALL DECLARATIONS OF PECUNIARY INTEREST AND THE GENERAL NATURE THEREOF 1 of 106 CITY COUNCIL (2016-09-27) MATTERS ARISING FROM THE PLANNING COMMITTEE SEPTEMBER 12, 2016 Council will consider, by way of one resolution, resolutions PL2016-137 to PL2016-139 and PL2016-141 to PL2016-143 inclusive, all of which are found at http://agendasonline.greatersudbury.ca/?pg=agenda&action=navigator&id=991&itemid=rec. Any questions regarding the resolutions should be directed to Councillor Cormier, Chair, Planning Committee. (RESOLUTION PREPARED) ADOPTING, APPROVING OR RECEIVING ITEMS IN THE CONSENT AGENDA (RESOLUTION PREPARED FOR ITEMS C-1 TO C-5) CONSENT AGENDA (For the purpose of convenience and for expediting meetings, matters of business of repetitive or routine nature are included in the Consent Agenda, and all such matters of business contained in the Consent Agenda are voted on collectively. A particular matter of business may be singled out from the Consent Agenda for debate or for a separate vote upon the request of any Councillor. In the case of a separate vote, the excluded matter of business is severed from the Consent Agenda, and only the remaining matters of business contained in the Consent Agenda are voted on collectively. Each and every matter of business contained in the Consent Agenda is recorded separately in the minutes of the meeting.) TENDERS AND REQUESTS FOR PROPOSALS C-1. -
2015 Year End Council Expense Report
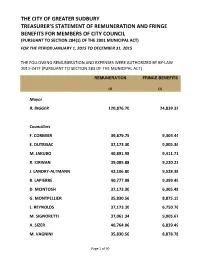
THE CITY OF GREATER SUDBURY TREASURER'S STATEMENT OF REMUNERATION AND FRINGE BENEFITS FOR MEMBERS OF CITY COUNCIL (PURSUANT TO SECTION 284(1) OF THE 2001 MUNICIPAL ACT) FOR THE PERIOD JANUARY 1, 2015 TO DECEMBER 31, 2015 THE FOLLOWING REMUNERATION AND EXPENSES WERE AUTHORIZED BY BY-LAW 2011-247F (PURSUANT TO SECTION 283 OF THE MUNICIPAL ACT) REMUNERATION FRINGE BENEFITS (1) (2) Mayor B. BIGGER 120,876.70 24,839.32 Councillors F. CORMIER 39,879.75 9,304.44 E. DUTRISAC 37,173.30 9,005.36 M. JAKUBO 40,891.98 9,411.71 R. KIRWAN 39,085.88 9,220.23 J. LANDRY-ALTMANN 42,106.80 9,528.38 R. LAPIERRE 40,777.08 9,399.49 D. MCINTOSH 37,173.30 6,305.48 G. MONTPELLIER 35,830.56 8,875.15 L. REYNOLDS 37,173.30 6,750.76 M. SIGNORETTI 37,061.34 9,005.67 A. SIZER 40,764.06 6,839.49 M. VAGNINI 35,830.56 8,878.78 Page 1 of 50 THE CITY OF GREATER SUDBURY TREASURER'S STATEMENT OF REMUNERATION AND FRINGE BENEFITS FOR MEMBERS OF CITY COUNCIL (PURSUANT TO SECTION 284(1) OF THE 2001 MUNICIPAL ACT) FOR THE PERIOD JANUARY 1, 2015 TO DECEMBER 31, 2015 THE FOLLOWING REMUNERATION AND EXPENSES WERE AUTHORIZED BY BY-LAW 2011-247F (PURSUANT TO SECTION 283 OF THE MUNICIPAL ACT) REMUNERATION FRINGE BENEFITS (1) (2) (1) The amounts include remuneration as members of Council as well as for any additional roles as Chair or member of the following committees or Boards: Deputy Mayor, Finance and Administration Committee, Audit Committee, Operations Committee, Planning Committee, Community Services Committee and Sudbury and District Health Unit. -

Making Mid-Sized the Right Size: Re-Envisioning Success in Ontario's Mid-Sized Cities
DISCUSSION PAPER Making Mid-Sized the Right Size: Re-envisioning Success in Ontario’s Mid-Sized Cities Acknowledgements 2 ACKNOWLEDGEMENTS his paper was prepared by Jo Flatt, Kris Longston, Acting Manager of Community & Senior Program Manager, Evergreen Strategic Planning, City of Greater Sudbury, Greater T Sudbury and Luisa Sotomayor. Deb McIntosh, Councilor, Ward 9, Greater Sudbury We would like to thank all of the interview participants for their time and effort in Sarah Meritt, Manager, Old East Village Business contributing to the development of this report, Association (OEVBIA), London as well as Ian Bromley for reviewing the paper. Debbi Nicholson, CEO, Greater Sudbury Chamber of This report is funded by the Ministry of Municipal Commerce, Greater Sudbury Affairs and House within the Province of Ontario. Acknowledgements Liz Palmieri, Executive Director, Niagara Community Foundation, St. Catharines Interview Participants: Judy Pihach, Manager, Planning and Development Services, City of St. Catharines, St. Catharines Michelle Baldwin, Executive Director, David Robinson, Director of the Institute for Northern Pillar Non-Profit Network, London Ontario Research and Development, Laurentian Mayor Brian Bigger, Greater Sudbury University, Greater Sudbury Ken Doherty, Director, Community Services, Brianna Salmon, Manager, Transportation and Urban City of Peterborough, Peterborough Design Programmes, Peterborough Sandra Dueck, Policy Analyst, Greater Peterborough Mayor Walter Sendzik, St. Catharines Chamber of Commerce, Peterborough Carmen -
$1.1 Billion Available to Address
Winter 2017 UnderONTARIO SEWER AND WATERMAINgrounder CONSTRUCTION ASSOCIATION $1.1 BILLION AVAILABLE TO ADDRESS Technology ONTARIO’S Use of Drones in Sewer and WATER AND WASTEWATER Watermain Industry Member Profile: INFRASTRUCTURE DEFICIT Enterprise Fleet Management The pipe that will revolutionize the landscape of infrastructure systems is here, and it’s PERFECT. PERFECT PIPE, a concrete pipe product manufactured with a high density polyethylene (HDPE) liner and thermoplastic internal connectors with dual elastomeric rubber gaskets for the ultimate in joint integrity and durability. It’s the future of waste water systems and it’s only available in Canada through Con Cast Pipe. Contact us to learn more or for a plant tour to view the production of the PERFECT Pipe. concastpipe.com | 1 800 668 PIPE | [email protected] 831213_ConCast.indd 1 12/10/16 8:10 pm 3D Machine Control + Sitelink 3D = A GAME CHANGER! SITELINK3D IN THE OFFICE IN THE FIELD IN THE CAB Sitelink3D - Advanced Communication System for 3D-MC Products Sitelink3D brings you that connectivity and control. Sitelink3D gives tabular views of project crews, their exact position, activities, files in use, plus a myriad of other functions. A simple key stroke allows the user to interact with any specific machine connected to the system. Topcon 3D Machine Control Systems: Sitelink3D • Increase Speeds up to 200% • Remote Support • Smoothness & Grading Accuracy • RTK Distribution • Easy-to-use Interface • Remote File Transfers • Text Messaging • Visibility & Tracking Find out about -

Day of Mourning Ceremonies 2017
Day of Mourning Ceremonies 2017 Ontario Region South Central Ontario REGION and ADDRESS EVENT DATE and TIME CONTACT Brantford & District Labour Speaker: Jeff Van Wyk, BDLC Friday, April 28 at 5:00 pm Roxanne Bond: 519-209-2154 or Council (BDLC) President; Mayor Chris Friel; [email protected] Fordview Park, Brantford Pastor Kevin Weeks Guelph & District Labour Council Guest Speakers: From Labour Friday, April 28 at 5:00 pm Terry O’Connor: 519-994-2474 5:00 pm - Meet at City Hall and the Community March to Goldie Mill Park 5:30 pm - Service at Goldie Mill Park Hamilton and District Labour Guest Speaker: Erin Harrison, Friday, April 28 at 5:30 pm Tom Atterton: 905-547-2944 or Council City Hall Chambers CLC [email protected] Niagara Regional Labour Council Friday, April 28 at 8:00 am Guylaine Tremblay: [email protected] St. Catharines Monument dedicated to four fallen workers – under the St. Catharines Skyway, located on the Welland Canal Parkway, west side of the canal under the bridge Niagara Regional Labour Council – Friday, April 28 at 9:00 am Guylaine Tremblay: [email protected] Niagara-on-the-Lake Monument located at the Centennial Arena, 1557 Four Mile Creek Road in Virgil Page 1 Niagara Regional Labour Council - Friday, April 28 at 10:00 am Guylaine Tremblay: [email protected] Niagara Falls Monument located at Niagara Falls City Hall, 4310 Queen Street Niagara Regional Labour Council – Friday, April 28 at 11:00 am Guylaine Tremblay: [email protected] Fort Erie Monument located at Fort Erie City Hall, 1 Municipal Centre Drive, along Hwy #3 Niagara Regional Labour Council – Friday, April 28 at 12:30 pm Guylaine Tremblay: [email protected] Port Colborne Monument located in HH Knoll Park on Sugarloaf Street beside the hospital Niagara Regional Labour Council – Friday, April 28 at 1:30 pm Guylaine Tremblay: [email protected] Welland Monument located beside the canal in Merritt Park, 151 King Street Niagara Regional Labour Council – Friday, April 28 at 2:30 pm Guylaine Tremblay: [email protected] Port Robinson In memory of Robyn Lafleur. -

Office of the Mayor Corporation of the City of Sault Ste. Marie
OFFICE OF THE MAYOR CORPORATION OF THE CITY OF SAULT STE. MARIE April 24, 2018 SENT VIA EMAIL The Honourable Ahmed D. Hussen Minister of Immigration, Refugees and Citizenship House of Commons Ottawa, Ontario K1A 0A6 The Honourable Laura Albanese Minister of Citizenship and Immigration Toronto, Ontario 6th Floor, 400 University Avenue M5G 1S5 Dear Minister Hussen and Minister Albanese, RE: Remedial measures to address immigration imbalance We, the members of Northern Ontario Large Urban Mayors (NOLUM), are reaching out to both of you, the Provincial and Federal Ministers responsible for immigration, regarding the implementation of remedial measures to address Ontario’s immigration imbalance. NOLUM members are calling for the Government of Ontario to partner with the Government of Canada to implement a program similar to the Atlantic Immigration Pilot. Northern Ontario faces challenges very similar to those in Atlantic Canada and even more precarious demographic issues. For instance, according to a report from the Government of Ontario, Ontario Population Projections Update, 2016-2041, the number of children aged 0 to 14 is projected to increase in Ontario, but decline in Northern Ontario and the majority of rural areas are expected to have significantly fewer children by 2041. Meanwhile, Northern Ontario’s share of seniors in the population is expected to increase to over 25% percent in most areas and the general aging of Northern Ontario’s population will result in a projected overall negative natural increase. Additionally, Northern Ontario is experiencing net out-migration, mostly among young adults, which reduces both current and future population growth. These challenges are significant factors in the projected decline of Northern Ontario’s population. -

Mark Signoretti
Presented To: City Council For Information Only Presented: Tuesday, Sep 27, 2016 Report Date Thursday, Aug 25, 2016 2016 Second Quarter Statement of Council Expenses Type: Correspondence for Information Only Resolution Signed By For Information Only Report Prepared By Christina Dempsey BACKGROUND Co-ordinator of Accounting Digitally Signed Aug 25, 16 Attached is second quarter Statement of Council Division Review Expenses for the period January 1, 2016 to June 30, 2016. Lorraine Laplante Manager of Accounting In accordance with the City's by-law on Transparency and Digitally Signed Aug 26, 16 Accountability and the Payment of Expenses for Members of Recommended by the Department Council and Municipal Employees by-law, the City of Greater Ed Stankiewicz Acting Chief Financial Officer/City Sudbury discloses an itemized statement of Council expenses on Treasurer a quarterly and annual basis. Digitally Signed Sep 13, 16 Recommended by the C.A.O. Each Councillor has an Office expense budget of $10,489 to pay Ed Archer for expenses that are eligible under Schedule B of the Payment Chief Administrative Officer of Expenses for Members of Council and Municipal Employees Digitally Signed Sep 13, 16 by-law. The Mayor has an annual operating budget. Also disclosed are Council Memberships and Travel expenses as well as Council expenses. Expenses disclosed relate to non-salary expenditures from these budgets. The Statement of Council Expenses discloses the total transactions by Members of Council. The appendices disclose the details of each transaction -

Canada's Largest Lgbtq2s Health Conference La Plus Importante Conférence Sur La Santé Lgbtq2s Au Canada
MARCH 21-24, 2018 DU 21 AU 24 MARS 2018 CANADA’S LARGEST LGBTQ2S HEALTH CONFERENCE LA PLUS IMPORTANTE CONFÉRENCE SUR LA SANTÉ LGBTQ2S AU CANADA RAINBOW HEALTH ONTARIO 2018 CONFERENCE Rainbow Health Ontario C’est avec une grande reconnaissance gratefully acknowledges que Santé arc-en-ciel Ontario remercie our generous sponsors nos généreux commanditaires. CHAMPIONS LEADERS / CHEF DE FILES Co-sponsors: Access Alliance & Women’s Health in Women’s Hands INNOVATORS / INNOVATEURS regarding the influence of sex and gender ways to develop the role and approach of on health throughout life, and to apply our union. At the Ontario Centre of Excellence www.unifor.org these research findings to identify and for Child and Youth Mental Health, we work with agencies to strengthen mental address pressing health challenges facing health services and build an accessible men, women, boys, girls and gender- The Association of Ontario Health system of care for children, youth and their diverse people. http://bit.ly/CIHR-IGH Centres is the voice of a vibrant network families and caregivers. We offer a diverse of community-governed primary health collection of tools, services, products and care organizations that share commitment training to help professionals find, use and Health Quality Ontario is the provincial to advancing health equity through the share evidence that improve outcomes. advisor on the quality of health care. delivery of comprehensive primary health Three strategic directions guide us in With the goal of excellent care for care. www.aohc.org doing this work. all Ontarians, Health Quality Ontario 1. Strengthening skills and knowledge reports to the public on how the system at the service area level is performing, develops standards for If you haven’t been to Sudbury lately, you 2.