Myanmar-Report-On-Situation-Analysis-Of-Population-And-Development-Reproductive
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Birma Na Zakręcie. Zmiany W Kraju Tysiąca Pagód 2007–2014
BIRMA NA ZAKRĘCIE MIĘDZY DYKTATURĄ A DEMOKRACJĄ BIRMA NA ZAKRĘCIE. ZMIANY W KRAJU TYSIĄCA PAGÓD 2007–2014 „Złoty Budda Mahamuni siedzi w głębi głównej nawy. Na wysokości jego pępka widać rusztowanie, a na nim trzech uwijających się mężczyzn, którzy nieustannymi ruchami PRZEMYSŁAW GASZTOLD-SEŃ rąk jak gdyby poprawiają coś w posągu. [...] Zachęceni przez przewodnika, wdrapujemy pracownik Biura Edukacji Publicznej IPN, się na rusztowanie, ale jedna z belek przywiera tak ściśle do posągu, że aby przejść do doktorant na Wydziale Dziennikarstwa i Nauk Politycznych Uniwersytetu przodu i stanąć oko w oko z Buddą, trzeba na zakręcie oprzeć się rękami o jego ramię. Warszawskiego. Autor książki Konces- Czuję obiema dłońmi gorącą lepkość jakiejś mazi i prześlizgnąwszy się szybko na przedni jonowany nacjonalizm. Zjednoczenie pomost rusztowania, odrywam z instynktownym uczuciem wstrętu ręce od posągu: są Patriotyczne „Grunwald” 1980–1990 ubabrane złotem” – zanotował w maju 1952 r. Gustaw Herling-Grudziński w dzienniku (2012, Nagroda Historyczna „Polityki” z podróży do Birmy1. Od czasu jego wizyty w Mandalaj minęło ponad sześćdziesiąt lat2. za debiut, nominacja do Nagrody Przez ten długi czas posąg Buddy znacznie się rozrósł dzięki płatkom złota przylepianym im. Kazimierza Moczarskiego), współautor tomu Syria During the Cold War. The East codziennie przez setki pielgrzymów. Przywiązania do religii nie podminowały ani rządy European Connection (razem z Janem parlamentarne, ani pół wieku krwawej wojskowej dyktatury. Buddyzm wciąż stanowi Adamcem i Massimilianem Trentinem, najważniejszą wartość i punkt odniesienia dla większości Birmańczyków. 2014). We wrześniu 2007 r. i w listopadzie Jaka jest Birma dzisiaj? Czy po wielu latach autorytarnych rządów generałów wejdzie 2013 r. podróżował po Birmie. na drogę ku demokracji? Czy wydarzenia z ostatnich lat są autentycznym krokiem w stronę reformy systemu? Nie na wszystkie pytania znajdzie się jednoznaczną odpowiedź, ale warto pochylić się nad tym najmniej znanym krajem Azji Południowo-Wschodniej. -

New Government's Initiatives for Industrial Development in Myanmar
CHAPTER 2 New Government’s Initiatives for Industrial Development in Myanmar Aung Min and Toshihiro KUDO This chapter should be cited as: Aung Min and Kudo, K., 2012. “New Government’s Initiatives for Industrial Development in Myanmar.” In Economic Reforms in Myanmar: Pathways and Prospects, edited by Hank Lim and Yasuhiro Yamada, BRC Research Report No.10, Bangkok Research Center, IDE-JETRO, Bangkok, Thailand. Chapter 2 New Government’s Initiatives for Industrial Development in Myanmar Aung Min and Toshihiro KUDO Abstract Since 1988, when the State Law and Order Restoration Council (military government) assumed state responsibility, the market has been partially opened to the outside world. Myanmar's industrialization has shown little progress as the previous government’s1 policies and poor international relations hampered FDI inflows. As the new “elected” government took office in 2011, significant changes in policies have taken place and this paper intends to highlight the efforts of the new government in its attempt to enhance industrial development. The paper assesses the performance of related union-level ministries and regional governments towards industrial development through establishing industrial zones in all states and regions, except the Chin and Kayah states. The establishment of seven new industrial zones and extension of 18 existing industrial zones is seen to have a positive effect on industrial development, although improvements in infrastructural facilities need to be realized. Introducing the SME Service Centre in Yangon and SME financing schemes enables the firms to obtain loans from the newly named Small and Medium Industrial Development Bank (SMIDB)2, thus contributing to SME development to some extent. -
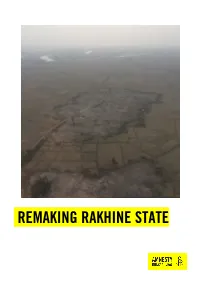
Remaking Rakhine State
REMAKING RAKHINE STATE Amnesty International is a global movement of more than 7 million people who campaign for a world where human rights are enjoyed by all. Our vision is for every person to enjoy all the rights enshrined in the Universal Declaration of Human Rights and other international human rights standards. We are independent of any government, political ideology, economic interest or religion and are funded mainly by our membership and public donations. © Amnesty International 2017 Except where otherwise noted, content in this document is licensed under a Creative Commons Cover photo: Aerial photograph showing the clearance of a burnt village in northern Rakhine State (attribution, non-commercial, no derivatives, international 4.0) licence. © Private https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode For more information please visit the permissions page on our website: www.amnesty.org Where material is attributed to a copyright owner other than Amnesty International this material is not subject to the Creative Commons licence. First published in 2017 by Amnesty International Ltd Peter Benenson House, 1 Easton Street London WC1X 0DW, UK Index: ASA 16/8018/2018 Original language: English amnesty.org INTRODUCTION Six months after the start of a brutal military campaign which forced hundreds of thousands of Rohingya women, men and children from their homes and left hundreds of Rohingya villages burned the ground, Myanmar’s authorities are remaking northern Rakhine State in their absence.1 Since October 2017, but in particular since the start of 2018, Myanmar’s authorities have embarked on a major operation to clear burned villages and to build new homes, security force bases and infrastructure in the region. -

Rakhine State
Myanmar Information Management Unit Township Map - Rakhine State 92° E 93° E 94° E Tilin 95° E Township Myaing Yesagyo Pauk Township Township Bhutan Bangladesh Kyaukhtu !( Matupi Mindat Mindat Township India China Township Pakokku Paletwa Bangladesh Pakokku Taungtha Samee Ü Township Township !( Pauk Township Vietnam Taungpyoletwea Kanpetlet Nyaung-U !( Paletwa Saw Township Saw Township Ngathayouk !( Bagan Laos Maungdaw !( Buthidaung Seikphyu Township CHIN Township Township Nyaung-U Township Kanpetlet 21° N 21° Township MANDALAYThailand N 21° Kyauktaw Seikphyu Chauk Township Buthidaung Kyauktaw KyaukpadaungCambodia Maungdaw Chauk Township Kyaukpadaung Salin Township Mrauk-U Township Township Mrauk-U Salin Rathedaung Ponnagyun Township Township Minbya Rathedaung Sidoktaya Township Township Yenangyaung Yenangyaung Sidoktaya Township Minbya Pwintbyu Pwintbyu Ponnagyun Township Pauktaw MAGWAY Township Saku Sittwe !( Pauktaw Township Minbu Sittwe Magway Magway .! .! Township Ngape Myebon Myebon Township Minbu Township 20° N 20° Minhla N 20° Ngape Township Ann Township Ann Minhla RAKHINE Township Sinbaungwe Township Kyaukpyu Mindon Township Thayet Township Kyaukpyu Ma-Ei Mindon Township !( Bay of Bengal Ramree Kamma Township Kamma Ramree Toungup Township Township 19° N 19° N 19° Munaung Toungup Munaung Township BAGO Padaung Township Thandwe Thandwe Township Kyangin Township Myanaung Township Kyeintali !( 18° N 18° N 18° Legend ^(!_ Capital Ingapu .! State Capital Township Main Town Map ID : MIMU1264v02 Gwa !( Other Town Completion Date : 2 November 2016.A1 Township Projection/Datum : Geographic/WGS84 Major Road Data Sources :MIMU Base Map : MIMU Lemyethna Secondary Road Gwa Township Boundaries : MIMU/WFP Railroad Place Name : Ministry of Home Affairs (GAD) translated by MIMU AYEYARWADY Coast Map produced by the MIMU - [email protected] Township Boundary www.themimu.info Copyright © Myanmar Information Management Unit Yegyi Ngathaingchaung !( State/Region Boundary 2016. -
Profile on Implementation of WHO Framework Convention on Tobacco Control in the South-East Asia Region WHO Library Cataloguing-In-Publication Data
Profile on Implementation of WHO Framework This Profile on the Implementation of the WHO Framework Convention on Tobacco Control in the South-East Asia Region Convention on Tobacco Control provides an overview of the status of the implementation of the convention in the eleven Member States of the SEA Region. in the South-East Asia Region It highlights some major milestones achieved as well as the challenges faced while implementing tobacco control measures in Member countries. Article 4: Every person will be informed of the health consequences, addictive nature and mortal threat posed by tobacco consumption and Article 11: Each Party shall adopt exposure to tobacco smoke …….. and implement effective measures to ensure that tobacco product Article 8: Parties recognize that packaging ad leveling do not promote exposure to tobacco smoke causes Article 14: Each Party shall develop a tobacco product, and each unit death disease and disability and disseminate appropriate, packet and package carry health ………. each party shall comprehensive, and integrated warnings describing harmful effects of implement measures to protect public guidelines and shall take effective tobacco use……………….. from the exposure to tobacco smoke in measures to promote cessation of indoor workplaces, publicArticle 13: Parties tobaccorecognize use that and a adequate treatment comprehensive ban onfor advertizing, tobacco dependence. promotion and sponsorshipArticle 16:wouldEach Party shall adopt reduce the consumptionand ofimplement tobacco effective measures to products……………...prohibit the sales of tobacco products to persons under the age set by domestic law, national law or eighteen. These measures may incude ISBN 978 92 9022 398 6 World Health House Indraprastha Estate, Mahatma Gandhi Marg, New Delhi-110002, India Website: www.searo.who.int 9789290 223986 Profile on Implementation of WHO Framework Convention on Tobacco Control in the South-East Asia Region WHO Library Cataloguing-in-Publication data World Health Organization, Regional Office for South-East Asia. -

Healthcare in Myanmar
REVIEW ARTICLE Nagoya J. Med. Sci. 78. 123 ~ 134, 2016 Healthcare in Myanmar Nyi Nyi Latt1, Su Myat Cho1, Nang Mie Mie Htun1, Yu Mon Saw2, Myat Noe Htin Aung Myint1, Fumiko Aoki1, Joshua A. Reyer1, Eiko Yamamoto1, Yoshitoku Yoshida1 and Nobuyuki Hamajima1 1Department of Healthcare Administration, Nagoya University Graduate School of Medicine, Nagoya, Japan 2Women Leaders Program to Promote Well-being in Asia, School of Health Sciences, Nagoya University Graduate School of Medicine, Nagoya, Japan ABSTRACT Myanmar transitioned to a civilian government in March, 2011. Although the democratic process has accelerated since then, many problems in the field of healthcare still exist. Since there is a limited overview on the healthcare in Myanmar, this article briefly describes the current states surrounding health services in Myanmar. According to the Census 2014, the population in the Republic of the Union of Myanmar was 51,410,000. The crude birth rate in the previous one year was estimated to be 18.9 per 1,000, giving the annual population growth rate of 0.89% between 2003 and 2014. The Ministry of Health reorganized into six departments. National non-governmental organizations and community-based organizations support healthcare, as well as international non-governmental organizations. Since hospital statistics by the govern- ment cover only public facilities, the information on private facilities is limited. Although there were not enough medical doctors (61 per 100,000 population), the number of medical students was reduced from 2,400 to 1,200 in 2012 to ensure the quality of medical education. The information on causes of death in the general population could not be retrieved, but some data was available from hospital statistics. -

Village Tracts of Mrauk - U Township Rakhine State
Myanmar Information Management Unit Village Tracts of Mrauk - U Township Rakhine State 93°0’E 93°10’E 93°20’E Kyauk Kyat Taung U Pyi Lone Gyi Ei Vi Ti Kar Kyi 20°48’N 20°48’N Yar Pyin Hteik Wa Pyin Pauk Pin Kwin Sin Ke Shar Yay Kan Sauk Pyin Oe Htein Pyaing Cha Tha Pyay Ma Kyar Se Kan Ta u n g M y in t Shwe Kyin Cheik Chaung Pyin Oke Kan Bu Ywet Gwa Son Ma Nyoe Hpa Yar Gyi Tein Nyo Byoke Chaung Maw Taung Taik Wet Hla Lay Hnyin Kone Baung Taung Tin Htein Kan 20°40’N Way Thar Li Gone Kyun 20°40’N Sin Oe Pya Hla Than Thin Pan Kaing Chaung Ywar Haung Taw MRAUK - U Kin Chaung Ah Yet Thay Ma Htan Ma Rit Na Kan Pu Zun Hpe Mrauk-U Myet Yaik Kyun Bar Nyo Kin Seik Urban Pu Rein Cha Yar Shauk Ta w Bwe i Ku Lar Ka Pon Kyun Baung Dut Paung Htoke Ka Da Wa Tan Tin Pi Pin Yin Than Ta Yar Ku Toe Nan Kya 20°32’N Naung Min 20°32’N Ma Har Kon Baung Su Yit Chaung Kyay Htee Oke Kar Kyaw Pin Lel Lay Hnyin Thar Pyar Te Yin Thei Myaung Than Shin Pyin Bway Maung Hna Ma Let Pan Taw Bu Ta Lone Zee Zar Kywe Te Koke Ka Rit Htaunt Ah Kyee Kant Tha Ri Set Thar Ta w M a Let Kyein Than Chi Nga Me Pyin Ye Hpyar Chaung Pyaung Paw Nyaung Pin Lel Nan Tet Ah Lel Chaung Kyar Kan Chin Shin Yae Zee Pin Gyi Hpa Yar Myar Tha Baw Mandalay Magway Nyaung 20°24’N Pin Lel (Ku Thar Yar Kone 20°24’N Lar Pone) K Thu Nge Taw Bay of Bengal Rakhine Bago Nat Chaung Minbya Kilometers Ayeyarwady 0482 Yangon 93°0’E 93°10’E 93°20’E Map ID: MIMU575v01 Legend Data Sources : GLIDE Number: TC-2010-000211-MMR Road Village Tract Boundaries Cyclone BASE MAP - MIMU Creation Date: 15 November 2010. -

Golden Mrauk-U, The: an Ancient Capital of Rakhine by U Shwe
A GUIDE TO MRAUK - U An Ancient City of Rakhine, Myanmar By Tun Shwe Khine (M.A) First Edition 1992 Historical Sites in Mrauk-U Aerial view of Mrauk-U I <i H Published by U Tun Shwe, Registrar (1) Sittway Degree College, Sittway. Registration No. 450/92 (10) 1992 Nov. 13. Art Adviser and Make-up U Kyaw Hla, Editor, University Translation & Publications Dept., Yangon. Photographs by Ko Tun Shaung, University Translation & Publications Dept., Yangon. Typeset by Shwe Min-Tha-Mee Computer, No. 9 (E), Thalawady Road, 7th mile, Yangon. Printed by U Tha Tun (03333), Nine Nines Press, 25, Razadirat Road, Botahtaung, Yangon. Tha Tun (03333) Cover Registration No. (413/92) (12), printed by U First Edition Jan: 1993, 2000 Copies. Cover - Dukkhanthein Shrine at Sun'set THE GOLDEN CITY OF MRAUK-U The Author Tun Shwe Khine was born in Rambyae, Rakhine State in 1949; graduated from Yangon University in 1972 and obtained master degree in Geography in 1976. He has served as a tutor in Yangon Worker's College; assistant lecturer and registrar (2) in Sittway Degree College. Now he is the Registrar (1) of Sittway Degree College. He has written several research articles and books, and edited some books, magazines and journals. "*,r. Some of his works excluding articles are as follows: (1) Rakhine State Regional Geography (in Myanmar), (2) Ancient Cities ofRakhine (in Myanmar), (3) The History of Rakhine Dynasty (in Myanmar), (4) The Thet Tribe in Northern Rakhine (in Myanmar), (5) Rakhine Buddhist Art in Vesali Period (in Myanmar), (6) Rakhine Folk-Tales (in Myan- mar), (7) Earlier Writers in Rakhine (in Myanmar), (8).4 Study ofRakhine Minthami Aye-gyin (in Myanmar), (9)The History of Rakhine Mahamuni (in Myanmar and English) and (10) Historical Sites in Rakhine (in English). -

The Protection of Human Rights of Rohingya in Myanmar: the Role of the International Community
Department of Political Science Master in International Relations Chair of: International Organization and Human Rights The Protection of Human Rights of Rohingya in Myanmar: The Role of The International Community CANDIDATE: SUPERVISOR: Riccardo Marzoli Professor Roberto Virzo No. 623322 CO-SUPERVISOR: Professor Francesco Cherubini Academic year: 2014/2015 TABLE OF CONTENTS INTRODUCTION ………………………………………………………………………...p.5 1.THE PAST: THE HISTORICAL PRESENCE OF ROHINGYA IN RAKHINE STATE. SINCE THE ORIGINS TO 1978…………………………………………………………. 9 1.1.REWRITING HISTORY: CONFLICTING VERSIONS OF BURMESE AND INTERNATIONAL SCHOLARS ………………………………………………………. 10 1.1.1 ETIMOLOGY OF THE TERMS…………………………………………………………………. 13 1.2. ANCIENT HISTORY OF ARAKAN AND FIRST ISLAMIC CONTACTS……… 14 1.3 CHANDRAS DINASTY AND THE ORIGINS OF THE MAGHS…………………16 1.4. MIN SAW MUN AND THE ARAKANESE KINGS WITH MUSLIM TITLES: THE SIGN OF A WIDESPREAD ISLAMIC INFLUENCE……………………………………...17 1.4.1 DIFFERENT VISIONS: WHICH ROLE FOR ROHINGYA IN MYANMAR?...................19 1.5 A NEW INFLUX: FRATRICIDAL WARS BETWEEN THE HEIRS OF THE MUGHALS’ THRONE AND THE ROLE OF THE KAMANS……………………………20 1.6 DIFFERENT WAVES OF MUSLIM ENTRANCES TO ARAKAN………………...21 1.7 1781 THE ADVENT OF THE BURMANS. THE OCCUPATION BY BODAW PAYA AND THE PREMISES OF THE BRITISH DOMINANCE ………………………………..24 1.7.1 KING SANDA WIZAYA AND THE KAMANS IN RAMREE………………………………...24 1.7.2 THE END OF THE KINGDOM OF MRAUK-U AND THE ARRIVAL OF THE AVA ARMY……………………………………………………………………………………………………………….25 1.7.3 KING BERING’S SAGA AND THE ARAKANESE -

MYANMAR/BURMA Breaking Barriers: Advocating Sexual and Reproductive Health and Rights
MYANMAR/BURMA BREAKING BarrIERS: Advocating Sexual and Reproductive Health and Rights ARROW COUNTRY STUDIES ISBN 978-967-0339-23-8 2016 This work is licensed under the Creative Commons Attribution-Non-Commercial 4.0 International License. To view a copy of this license, visit http://creativecommons.org/ licenses/by-nc/4.0/. Any part of the text of the publication may be photocopied, reproduced, stored in a retrieval system, or transmitted in any form by any means, or adapted and translated to meet local needs, for non-commercial and non-profit purposes. However, the copyright for images used remains with respective copyright holders. All forms of copies, reproductions, adaptations, and translations through mechanical, electrical, or electronic means should acknowledge ARROW as the source. A copy of the reproduction, adaptation, and/or translation should be sent to ARROW. In cases of commercial usage, ARROW must be contacted for permission at [email protected] Asian-Pacific Resource and Research Centre for Women (ARROW) 1 & 2 Jalan Scott, Brickfields, Kuala Lumpur, Malaysia 50470 Telephone (603) 2273 9913/9914 Fax (603) 2273 9916 E-mail [email protected] Web www.arrow.org.my Facebook The Asian-Pacific Resource & Research Centre for Women (ARROW) Twitter @ARROW_Women Youtube youtube.com/user/ARROWomen Pinterest arrowomen Production Team Researchers: Rachael McGuin & Nang Lao Liang Won Research Coordinator: Nalini Singh Publication Coordinator/Editor: Maria Melinda Ando Overall Oversight: Sivananthi Thanenthiran & Tabinda Sarosh Copy Editor/Researcher -

Fatal Silence ?
FATAL SILENCE ? Freedom of Expression and the Right to Health in Burma ARTICLE 19 July 1996 ACKNOWLEDGEMENTS This report was written by Martin Smith, a journalist and specialist writer on Burma and South East Asia. ARTICLE 19 gratefully acknowledges the support of the Open Society Institute for this publication. ARTICLE 19 would also like to acknowledge the considerable information, advice and constructive criticism supplied by very many different individuals and organisations working in the health and humanitarian fields on Burma. Such information was willingly supplied in the hope that it would increase both domestic and international understanding of the serious health problems in Burma. Under current political conditions, however, many aid workers have asked not to be identified. ©ARTICLE 19 ISBN 1 870798139 All rights reserved. No part of this publication may be photocopied, recorded or otherwise reproduced, stored in a retrieval system or transmitted in any form by any electronic or technical means without prior permission of the copyright owner and publisher. Note by the editor of this Internet version This version is a conversion to html of a Word document - in the Library at http://www.ibiblio.org/obl/docs/FATAL- SILENCE.doc - derived from a scan of the 1996 hard copy. The footnotes, which in the original were numbered from 1 to __ at the end of each chapter, are now placed at the end of the document, and number 1-207. The footnote references to earlier footnotes have been changed accordingly. In addition, where online versions exist of the documents referred to in the notes and bibliography, the web addresses are given, which was not the case in the original. -

Revitalizing Agriculture in Myanmar
Revitalizing Agriculture in Myanmar: Breaking Down Barriers, Building a Framework for Growth Prepared for International Development Enterprises | Myanmar DISTRIBUTION, CITATION, OR QUOTATION NOT PERMITTED WITHOUT PERMISSION July 21, 2010 This paper was written by David O. Dapice ([email protected]), Thomas J. Vallely ([email protected]), and Ben Wilkinson ([email protected]) of the Ash Center for Democratic Governance and Innovation at the Harvard Kennedy School and Michael J. Montesano ([email protected]) of the Institute of Southeast Asian Studies in Singapore. The views expressed herein are the authors’ alone and do not necessarily reflect those of IDE, the government of the Union of Myanmar, the Harvard Kennedy School, Harvard University, or the Institute of Southeast Asian Studies. We wish to extend our sincere thanks to our colleagues at IDE/Myanmar and the Ministry of Agriculture and Irrigation for their contributions to the research and for organizing the complex logistics the assessment demanded. Partial funding for the study was provided by the Royal Norwegian Government. Revitalizing Agriculture in Myanmar July 2010 Page 3 of 64 Distribution, Citation, or Quotation Not Permitted Without Permission of IDE TABLE OF CONTENTS MAP | Union of Myanmar ........................................................................................................................... 4 INTRODUCTION ........................................................................................................................................