George Mason Cheerleading
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
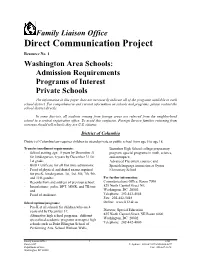
Washington Area Schools: Admission Requirements Programs of Interest Private Schools
Family Liaison Office Direct Communication Project _____________________________________________________________________________________________________________________ Resource No. 1 Washington Area Schools: Admission Requirements Programs of Interest Private Schools The information in this paper does not necessarily indicate all of the programs available in each school district. For comprehensive and current information on schools and programs, please contact the school district directly. In some districts, all students coming from foreign areas are referred from the neighborhood school to a central registration office. To avoid this confusion, Foreign Service families returning from overseas should tell schools they are U.S. citizens. District of Columbia District of Columbia law requires children to attend private or public school from age 5 to age 18. Transfer/enrollment requirements: Banneker High School college preparatory · School starting age: 5 years by December 31 program, special programs in math, science, for kindergarten, 6 years by December 31 for and aerospace; 1st grade; · Advanced Placement courses; and · Birth Certificate for all first time admissions; · Spanish language immersion at Oyster · Proof of physical and dental exams required Elementary School. for pre-K, kindergarten, 1st, 3rd, 5th, 7th, 9th, and 11th grades; For further information: · Records from and address of previous school; Communications Office, Room 7096 · Inoculations: polio, DPT, MMR, and TB test; 825 North Capitol Street NE and Washington, DC 20002 -

Body Found After Search for Missing Man KKK Flyers Delivered to Fork
FLUVANNAREVIEW.COM JAN. 31 – FEB. 6, 2019 | VOLUME 39, ISSUE 5 | ONE COPY FREE Supervisors Discuss New Tax PAGE 23 Lake Board Votes for Phased-In Dues Increase PAGE 6 Carysbrook Announces Honor Roll PAGE 14 Body Found After Search for Missing Man PAGE 4 KKK Flyers Delivered to Fork Union Area PAGE 12 Guilty Plea in Arson, Flucos Rally for Attempted Murder Overtime Win PAGE 12 PAGE 22 THIS WEEK’S PET Dear Fluvanna Friends, My team, Gunnels Group, has been Hello I’m Two! honored to service our Fluvanna f I am a very sweet 6 Years old. community since 2001, and it will be a I love to be petted on the head. When I first got here, privilege to service your real estate I was a little scared, but I am coming around. When new people come around, I will hide in the back needs in 2019. of my cage, but if you keep talking to me softly, I will come to the front of the cage wanting attention. Gunnels Group helps achieve our buyer clients’ dream of I am current on all shots, micro-chipped & Neutered. I am located at PetSmart - homeownership, and our seller clients transition into their next phase 425 Merchant walk square Charlottesville, VA 22902 of life. We are dedicated to offering our clients thoughtful advice, Fluvanna SPCA | 5239 Union Mills Rd., Troy, VA (434) 591-0123 | www.fspca.org thorough guidance and attentive customer service. Contact us today and we will work together to achieve your real estate goals. SPONSORED BY John, Pat & Rascal Your Local Realtor, Maggie Gunnels Whether you need help to Owner, Gunnels Group rentAd Proof a home#1 or manageFluvanna Review your -01-31-19 property, Issue Associate Broker, Long & Foster we have the solution. -
George Mason University
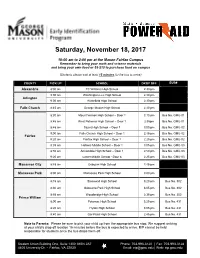
Saturday, November 18, 2017 10:00 am to 2:00 pm at the Mason Fairfax Campus Remember to bring your math and science materials and bring your own food or $8-$10 to purchase food on campus (Students please wait at least 15 minutes for the bus to arrive) COUNTY PICK UP SCHOOL DROP OFF BUS# Alexandria 8:30 am TC Williams High School 2:30 pm 9:00 am Washington-Lee High School 2:30 pm Arlington 9:00 am Wakefield High School 2:30 pm Falls Church 8:45 am George Mason High School 2:30 pm 8:30 am Mount Vernon High School – Door 1 3:10 pm Bus No. GMU-01 8:45 am West Potomac High School – Door 1 2:55pm Bus No. GMU-01 8:45 am Stuart High School – Door 1 3:00 pm Bus No. GMU-02 9:00 am Falls Church High School – Door 1 2:45 pm Bus No. GMU-02 Fairfax 9:20 am Fairfax High School – Door 1 2:25 pm Bus No. GMU-02 8:35 am Holmes Middle School – Door 1 3:05 pm Bus No. GMU-03 8:50 am Annandale High School – Door 1 2:50 pm Bus No. GMU-03 9:20 am Lanier Middle School - Door 8 2:25 pm Bus No. GMU-03 Manassas City 8:45 am Osbourn High School 2:45 pm Manassas Park 8:30 am Manassas Park High School 3:00 pm 8:15 am Stonewall High School 3:20 pm Bus No. 302 8:30 am Osbourne Park High School 3:05 pm Bus No. -

Libraries, Technology, and the Route to Relevance Facilities Master
Volume 5, Issue 2 Get the latest industry news and trends: Libraries, Technology, And The Route To Relevance By better aligning their services to community needs, they can target inequities and support economic opportunity Cameron Chavira Like the footings beneath the shelves they line, books have traditionally formed the foundation of the services that public libraries offer their communities. However, with the shift from print to digital publishing, libraries face a battle in maintaining their status as bastions for learning, community engagement, workforce development and citizenship. This challenge has not gone unnoticed by local-government budget-writers, who are increasingly likely to cut funding for libraries in favor of more "necessary" departments and programs. Nevertheless, library professionals remain hopeful that technology will help moderate inequities in areas such as access to information, educational achievement and economic opportunity. But to successfully leverage technology to this effect, we must make sure that those who make funding decisions see libraries not as stuffy stacks of yellowing pages but as modern community learning centers. This can be achieved through thoughtful assessment and partnership. Here's how: First, libraries need to identify service gaps by evaluating the needs of their users against the services they provide. Technology can be a great help here, given the variety of data-driven mapping tools now available to help shape precise community profiles. These tools, typically employed for purposes of planning and zoning, offer libraries a detailed dissection of a neighborhood's demographics, including education level, family composition and transit information. Once libraries have this profile defined, they can assess how their services align with the community's needs. -

George Mason High School
George Mason High School State of the Schools Report October 14, 2008 1 GMHS State of the Schools Report October 14, 2008 Introduction Department Profiles Challenge Statement (1) Horizontal Meetings (41-42) Staff Demographics (2) English (43-44) Student Demographics (3-4) Fine and Performing Arts (45-46) Foreign Language (47-48) School Plan Physical Education/Health/Drivers ED (49-50) Student Achievement (6) Career and Tech Ed (51-53) MYP (7-8) Social Studies (54-55) IB 5-Year Review (9-11) Mathematics (56-57) School Schedule (12) Science (58-59) Student Activities (13) Special Education (60-61) Professional Development (14) Counseling (62-68) Family and Community (15-16) Alternative Education (69) Data Use (17) IB/Gifted and Talented (70–74) Library (75) School Day Daily Schedule (19) Program Reports TA (19) Summer School (77-78) Activities (19) Class of 2008 Statistics (79-80) Technology (20-22) Attendance Initiatives (81-82) Athletics (23) Academic/Career/Fitness/School Climate Evaluation Tools SRI (25) STAMP (26) Math Evaluation (26) Naviance and Kudor (27) Impact Protocol (29) FitnessGram (30) Pride Survey (30) Support Programs House (32-33) Student Services (33) Gateway (34) EIP (34) Writing Lab (35) Math Lab (35-36) Eighth Grade Transition (37-39) Challenge Statement At George Mason we are an exciting and collaborative community of learners who strive toward excellence. We care for each other and take pride in and responsibility for our individual and mutual growth and accomplishments. We celebrate our diversity and seek to foster respect for all in the community through global awareness and appreciation of our individual and cultural differences. -

Fccps High School Renaming Committee Final Report
FCCPS HIGH SCHOOL RENAMING COMMITTEE FINAL REPORT Submitted by: The FCCPS High School Renaming Committee Jamie Argento Rodriguez, Chair April 9, 2021 INTRODUCTION The FCCPS High School Renaming Committee firmly holds that the renaming of the high school must be considered as a starting point along the necessary path for change in the City of Falls Church. If accomplished in isolation, changing the name of the high school is an empty gesture. As the School Board considers the names that the committee recommends in this report, we urge and request that the School Board, FCCPS, and the Fall Church City community build on the momentum forged by the renaming effort to create positive outcomes for the students, faculty, residents, and visitors for whom the school is built to serve. The high school name change, and the corresponding elementary school name change, present an opportunity to educate us about the history of Falls Church City, to shine a light on its African-American community and heritage, and to steer us on a course towards inclusion and equity. The committee respectfully submits this report in furtherance of these goals. PROCESS OVERVIEW Committee membership The FCCPS High School Renaming Committee was selected by Superintendent Dr. Peter Noonan in January 2021. The committee’s membership includes 26 members representing a diverse set of experiences. The committee consists of high school students, FCCPS faculty in multiple roles, FCCPS alumni, parents, and community members. The committee’s members are diverse in gender, race, ethnicity, sexual orientation, and other important factors that represent the broader Falls Church City community. -

George Mason 2019 Quick Facts
GEORGE MASON 2019 QUICK FACTS George Mason University 2019 Men’s Soccer GENERAL INFORMATION Top Returning Players (2018 Stats) Location Fairfax, Va. Enrollment 39,904 (23,812 Undergraduate) Tunde Akinlosotu (Sr.) 5G, 5A, 15 PTS. Founded 1957 (University Status, 1972) Ryan Mingachos (Sr.) 4G, 4A, 12 PTS. Nickname Patriots Grant Robinson (Sr.) 5G, 2A, 12 PTS. Colors Green and Gold Pablo Pertusa (Sr.) 2G, 4A, 8 PTS. Stadium (Capacity) George Mason Stadium (5,000) Affiliation NCAA Division I Conference Atlantic 10 Conference Newcomers President Anne Holton Name P Yr Hometown Previous School Athletic Director Brad Edwards Asker Damgaard M Fr. Copenhagen, Denmark Gefion Gymnasium Athletic Website GoMason.com Sukrija Dudic M Sr. Srebrenica, Bosnia i Hercegovina New Haven SOCCER STAFF VanDyke Gyau D Jr. Alexandria, Va. Richard Bland College Head Coach Greg Andrulis (Eastern Connecticut State, ‘80) Brendan Hogan F Fr. Haymarket, Va. Battlefield Overall Record 254-174-65 (27th season) Keaton Jennings GK R-Fr. Cranberry Township, Pa. Robert Morris Record at Mason 120-102-37 (15th season) Brison Moorhead GK So. Clearwater, Fla. Presbytarian College Assistant Coach Billy Chiles (Towson, ‘08) Léon Reilhac M Fr. Esslingen, Germany JFK Wirtschaftsgymnasium Assistant Coach Eduardo de Souza (Trevecca Nazarene, ‘03) Tillman Theurich GK Fr. Berlin, Germany Flatowe Oberschule Athletic Trainer Ray Yamrus Mads Tranberg D Jr. Copenhagen, Denmark Cincinnati Strength and Conditioning Coach John Delgado Soccer Office Number (703) 993-3288 ATHLETIC COMMUNICATIONS -

Summer Camps
The Falls Church Recreation and Parks Department summer camp offerings operate as a program exempt from licensure with basic health and safety requirements but has no direct oversight by the Virginia Department of Social Services. Children 6 & up are limited to five weeks of contracted camps (pages 6-21) per location. Staff will monitor to ensure campers are within these parameters. If you have questions, please contact the Recreation and Parks Department at 703-248-5027 or [email protected] Campers will need to bring a lunch with drink and an afternoon snack daily. There is no refrigeration. If a child needs medication during camp, visit www.fallschurchva.gov/camps for information/paperwork. REGISTRATION INFORMATION: REFUND POLICY: Payment in full is required at the time of registration. The Recreation and Parks Department will provide a full credit Families can register: or refund for a camp if the camp is cancelled by the Online at www.fallschurchva.gov/Register Department, or upon request when schedule or location By calling 703-248-5027. Phone-in registrations will changes made by the Department prohibit or limit an not be accepted on March 8 or 15 before 10:00am. individual's ability to attend a camp. For any reason other than those noted above, a “Request for Refund/Household Credit” In-person registration is not available at this time. form must be completed and submitted at least two weeks FALLS CHURCH COMMUNITY CENTER HOURS: before the start of camp. Monday-Friday 9am - 8pm Requests for a refund made at least 14 calendar days before Saturday 8:30am – 12pm the start of camp will be granted, less a 20% processing fee. -

Virginia Operation Prom/ Graduation
1 VIRGINIA OPERATION PROM/ fundraising ideas, and decorations with as much hands- on as possible. Reservations must be made in advance. GRADUATION • Provides presentations and consultations for Virginia high In accordance with the position of the U.S. and Virginia schools who request them. Departments of Education that illicit drug and alcohol use • Provides presentations at state and national conferences. is wrong and harmful, Virginia Operation Prom/Graduation These have included the U.S. Department of Education, (OP/G) advocates a “no use” policy for youth. Virginia National Association of Secondary School Principals, OP/G does not accept donations from any alcohol or tobacco National Association of School Boards, Virginia manufacturers or distributors to facilitate or promote the Governor’s Alcohol and Other Drug Conference, Greater state program. Washington Council of Governments, Texas State School Board Association, Eastern Kentucky Alcohol/Drug-Free WHAT IS OP/G? Celebration Seminar, Maryland Prevention Council, and Virginia Operation Prom/Graduation is a project of the the Baltimore Private School Council. Virginia Department of Education in cooperation with the Virginia State Police Association. • On request produces all-night celebration simulations for state conferences. Any school is welcome to send In response to a 1987 request from the Virginia representatives to observe or obtain hands-on experience. Department of Motor Vehicles, the Virginia Department of Education developed the Virginia Operation Prom/Graduation • Visits prom and graduation celebrations to (OP/G) project. The purpose of OP/G is to address the serious photographically record and find new ideas that can be issues of youth drinking, drug use, and driving behavior during shared via workshops and the planning guide. -

City of Falls Church GEORGE MASON HIGH SCHOOL FEASIBILITY STUDY
Attachment A RFP 03-07-17-GMHSFS City of Falls Church GEORGE MASON HIGH SCHOOL FEASIBILITY STUDY BACKGROUND & PURPOSE The City of Falls Church (“City”) is a high-density, urban jurisdiction with a population of 14,000 people located six (6) miles outside of Washington, D.C. The City and Falls Church City Public Schools (“FCCPS”) seek an experienced and qualified Architect to create a Feasibility Study (“Study”) for: • a new George Mason High School; • space to accommodate a future addition to the existing Mary Ellen Henderson Middle School; • sports facilities; and • parking facilities to support the new development. The development site is located at 7124 & 7130 Leesburg Pike, Falls Church VA 22043. The Study should maximize any unused portion of the school development site for commercial development, to be located at the Haycock Road end of the site. The unused portion of the site may be as large as ten (10) acres. The City and FCCPS anticipate six (6) two ‐hour meetings to discuss the Program. SCOPE OF WORK The proposed Study will provide analysis and verification of the current George Mason High School Program (“Program”), including accommodations / academic classroom spaces for 1,200 students, and common spaces capable of accommodating 1,500 students. The Study will provide two (2) alternatives for each of two (2) scenarios to build a new George Mason High School: a. Scenario 1 – Construct a new High School with space reserved for a Mary Ellen Henderson Middle School expansion. The entire existing High School will be demolished. b. Scenario 2 – Construct a new High School with renovations to a portion of existing High School space (see attached drawing for anticipated existing spaces to remain). -

George Mason University, Fairfax Campus 4400 University Drive, Fairfax, VA 22030 (Students Please Wait for at Least 15 Minutes for the Bus to Arrive)
m July 08, 2019 - July 26, 2019 8:30 a.m.- 2:30 p.m. George Mason University, Fairfax Campus 4400 University Drive, Fairfax, VA 22030 (Students please wait for at least 15 minutes for the bus to arrive) COUNTY PICK UP SCHOOL DROP OFF In the morning, Alexandria City In the afternoon, the bus students will be taking summer school T.C. WILLIAMS will drop students at the Alexandria buses to T.C. Williams. High School designated stops. Bus will depart T.C. Williams at 7:30am 3330 KING ST Please See Afternoon Bus going to GMU. Roster Schedule. COUNTY PICK UP SCHOOL/LOCATION DROP OFF BUS# 6:40 AM S ABINGDON ST & 29TH ST S 3:19 PM GMU 416 6:46 AM DREW SCHOOL 3:07 PM GMU 416 6:56 AM RANDOLPH ELEMENTARY SCHOOL 3:02 PM GMU 416 7:00 AM S HIGHLAND ST & 7TH ST S 2:56 PM GMU 416 7:06 AM 5TH ST N & N OXFORD ST 2:51 PM GMU 416 7:08 AM N THOMAS ST & 4TH ST N 2:48 PM GMU 416 7:15 AM 8TH RD N & N MANCHESTER ST 2:43 PM GMU 416 6:30 AM WAKEFIELD HIGH SCHOOL 3:52 PM GMU 623 6:40 AM 28TH ST S & S MEADE ST 3:42 PM GMU 623 Arlington 6:47 AM 2111 JEFFERSON DAVIS HWY 3:36 PM GMU 623 6:50 AM 15TH ST S & S FERN ST 3:33 PM GMU 623 6:57 AM 13TH RD S & S QUEEN ST 3:25 PM GMU 623 7:05 AM 16TH ST N & N QUINN ST 3:17 PM GMU 623 7:09 AM LEE HWY & N CLEVELAND ST 3:14 PM GMU 623 7:15 AM GLEBE ELEMENTARY SCHOOL 3:09 PM GMU 623 Note to Parents: Please be sure to pick your child up from the appropriate bus stop. -

Falls Church 11.13.15 Clean Copy.Indd
Mason Greens Joint Venture CONCEPTUAL PROPOSAL PURSUANT TO THE PUBLIC-PRIVATE EDUCATION FACILITIES AND INFRASTRUCTURE ACT TO INCLUDE A NEW OR RENOVATED GEORGE MASON HIGH SCHOOL, EXPANSION OF THE EXISTING MARY ELLEN HENDERSON MIDDLE SCHOOL AND COMMERCIAL DEVELOPMENT RFP NO. 0730-15GMHS-PPEA DUE: OCTOBER 30, 2015 Table of Contents Cover Letter Letter of Submittal Executive Summary 1. Qualifications and Experience A. Structure - Partially Redacted, See Confidential Binder B. Experience of Entities C. Firm and Major Subcontractor Experience D. Persons Directly Involved with Mason Greens Development - Partially Redacted, See Confidential Binder E. Financial Statements F. Disqualified Persons G. Plans for Obtaining Qualified Workers H. VA DGS Form 30-168 I. SWaM Business Participation 2. Project Characteristics A. Project Vision - See Confidential Binder B. School Board, City and Public Entity Involvement C. Permits and Approvals D. Anticipated Adverse Impacts - Partially Redacted, See Confidential Binder E. Schedule - See Confidential Binder F. Contingency Plans for Addressing Public NeedsSee Confidential Binder G. Risk and Liability - Partially Redacted, See Confidential Binder H. Ownership and Management - See Confidential Binder I. Phasing - See Confidential Binder J. Architectural, Building and Engineering Standards H. Involvement of Adjacent Owner and Tenants 3. Project Financing - See Confidential Binder 4. Project Benefits & Compatibility A. Economic Impact on Local Community - Partially Redacted, See Confidential Binder B. Community Engagement Strategy - Partially Redacted, See Confidential Binder C. Unique Benefits D. Compatibility with Existing Plans Appendices Partially Redacted, See Confidential Binder This Proposal contains appropriately marked proprietary and/or confidential information. __No __Yes9 The City of Falls Church and its Public Schools are committed to the letter and spirit of the Americans with Disabilities Act.