Thalamus.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Role of the Hypothalamic Dorsomedial Nucleus in the Central Regulation of Food Intake
The role of the hypothalamic dorsomedial nucleus in the central regulation of food intake Ph.D. thesis Éva Dobolyiné Renner Semmelweis University Szentágothai János Neuroscience Doctoral School Ph.D. Supervisor: Prof. Miklós Palkovits, member of the HAS Opponents: Prof. Dr. Halasy Katalin, Ph.D., D.Sci. Dr. Oláh Márk, M.D., Ph.D. Examination board: Prof. Dr. Vígh Béla, M.D., Ph.D., D.Sci Dr. Kovács Krisztina Judit, Ph.D., D.Sci. Dr. Lovas Gábor, M.D., Ph.D. Budapest 2013 1. Introduction The central role of the hypothalamus in the regulation of food intake and energy expenditure has long been established. The hypothalamus receives hormonal input such as insulin, leptin, and ghrelin from the periphery. The gate for the most important adiposity signals is the arcuate nucleus, which contains neurons expressing orexigenic and anorexigenic peptides, respectively. These neurons convey peripheral input to the paraventricular and ventromedial nuclei, and the lateral hypothalamic area, which all play critical roles in body weight regulations. The hypothalamic dorsomedial nucleus (DMH) has also been implicated in the regulation of body weight homeostasis along with other hypothalamic nuclei including the arcuate, ventromedial, and paraventricular nuclei as well as the lateral hypothalamus. Lesions of the DMH affected ingestive behavior. Electrophysiological data suggested that neurons in this nucleus integrate hormonal input and ascending brainstem information and, in turn, modulate food intake and energy balance. In response to refeeding of fasted rats, Fos-activated neurons were reported in the DMH. Major projections relay vagus-mediated signals from the gastrointestinal tract, and humoral signals to the hypothalamus from the nucleus of the solitary tract (NTS), a viscerosensory cell group in the dorsomedial medulla. -

Cortex and Thalamus Lecture.Pptx
Cerebral Cortex and Thalamus Hyperbrain Ch 2 Monica Vetter, PhD January 24, 2013 Learning Objectives: • Anatomy of the lobes of the cortex • Relationship of thalamus to cortex • Layers and connectivity of the cortex • Vascular supply to cortex • Understand the location and function of hypothalamus and pituitary • Anatomy of the basal ganglia • Primary functions of the different lobes/ cortical regions – neurological findings 1 Types of Cortex • Sensory (Primary) • Motor (Primary) • Unimodal association • Multimodal association - necessary for language, reason, plan, imagine, create Note: • Gyri • Sulci • Fissures • Lobes 2 The Thalamus is highly interconnected with the cerebral cortex, and handles most information traveling to or from the cortex. “Specific thalamic Ignore nuclei” – have well- names of defined sensory or thalamic nuclei for motor functions now - A few Other nuclei have will more distributed reappear later function 3 Thalamus Midbrain Pons Limbic lobe = cingulate gyrus Structure of Neocortex (6 layers) white matter gray matter Pyramidal cells 4 Connectivity of neurons in different cortical layers Afferents = inputs Efferents = outputs (reciprocal) brainstem etc Eg. Motor – Eg. Sensory – more efferent more afferent output input Cortico- cortical From Thalamus To spinal cord, brainstem etc. To Thalamus Afferent and efferent connections to different ….Depending on whether they have more layers of cortex afferent or efferent connections 5 Different areas of cortex were defined by differences in layer thickness, and size and -

Basal Ganglia & Cerebellum
1/2/2019 This power point is made available as an educational resource or study aid for your use only. This presentation may not be duplicated for others and should not be redistributed or posted anywhere on the internet or on any personal websites. Your use of this resource is with the acknowledgment and acceptance of those restrictions. Basal Ganglia & Cerebellum – a quick overview MHD-Neuroanatomy – Neuroscience Block Gregory Gruener, MD, MBA, MHPE Vice Dean for Education, SSOM Professor, Department of Neurology LUHS a member of Trinity Health Outcomes you want to accomplish Basal ganglia review Define and identify the major divisions of the basal ganglia List the major basal ganglia functional loops and roles List the components of the basal ganglia functional “circuitry” and associated neurotransmitters Describe the direct and indirect motor pathways and relevance/role of the substantia nigra compacta 1 1/2/2019 Basal Ganglia Terminology Striatum Caudate nucleus Nucleus accumbens Putamen Globus pallidus (pallidum) internal segment (GPi) external segment (GPe) Subthalamic nucleus Substantia nigra compact part (SNc) reticular part (SNr) Basal ganglia “circuitry” • BG have no major outputs to LMNs – Influence LMNs via the cerebral cortex • Input to striatum from cortex is excitatory – Glutamate is the neurotransmitter • Principal output from BG is via GPi + SNr – Output to thalamus, GABA is the neurotransmitter • Thalamocortical projections are excitatory – Concerned with motor “intention” • Balance of excitatory & inhibitory inputs to striatum, determine whether thalamus is suppressed BG circuits are parallel loops • Motor loop – Concerned with learned movements • Cognitive loop – Concerned with motor “intention” • Limbic loop – Emotional aspects of movements • Oculomotor loop – Concerned with voluntary saccades (fast eye-movements) 2 1/2/2019 Basal ganglia “circuitry” Cortex Striatum Thalamus GPi + SNr Nolte. -
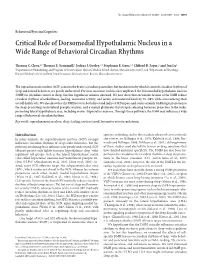
Critical Role of Dorsomedial Hypothalamic Nucleus in a Wide Range of Behavioral Circadian Rhythms
The Journal of Neuroscience, November 19, 2003 • 23(33):10691–10702 • 10691 Behavioral/Systems/Cognitive Critical Role of Dorsomedial Hypothalamic Nucleus in a Wide Range of Behavioral Circadian Rhythms Thomas C. Chou,1,2 Thomas E. Scammell,2 Joshua J. Gooley,1,2 Stephanie E. Gaus,1,2 Clifford B. Saper,2 and Jun Lu2 1Department of Neurobiology and Program in Neuroscience, Harvard Medical School, Boston, Massachusetts 02115, and 2Department of Neurology, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston, Massachusetts 02215 The suprachiasmatic nucleus (SCN) contains the brain’s circadian pacemaker, but mechanisms by which it controls circadian rhythms of sleep and related behaviors are poorly understood. Previous anatomic evidence has implicated the dorsomedial hypothalamic nucleus (DMH) in circadian control of sleep, but this hypothesis remains untested. We now show that excitotoxic lesions of the DMH reduce circadian rhythms of wakefulness, feeding, locomotor activity, and serum corticosteroid levels by 78–89% while also reducing their overall daily levels. We also show that the DMH receives both direct and indirect SCN inputs and sends a mainly GABAergic projection to the sleep-promoting ventrolateral preoptic nucleus, and a mainly glutamate–thyrotropin-releasing hormone projection to the wake- promoting lateral hypothalamic area, including orexin (hypocretin) neurons. Through these pathways, the DMH may influence a wide range of behavioral circadian rhythms. Key words: suprachiasmatic nucleus; sleep; feeding; corticosteroid; locomotor activity; melatonin Introduction sponses, in feeding, and in the circadian release of corticosteroids In many animals, the suprachiasmatic nucleus (SCN) strongly (for review, see Bellinger et al., 1976; Kalsbeek et al., 1996; Ber- influences circadian rhythms of sleep–wake behaviors, but the nardis and Bellinger, 1998; DiMicco et al., 2002), although many pathways mediating these influences are poorly understood. -

The Connexions of the Amygdala
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.28.2.137 on 1 April 1965. Downloaded from J. Neurol. Neurosurg. Psychiat., 1965, 28, 137 The connexions of the amygdala W. M. COWAN, G. RAISMAN, AND T. P. S. POWELL From the Department of Human Anatomy, University of Oxford The amygdaloid nuclei have been the subject of con- to what is known of the efferent connexions of the siderable interest in recent years and have been amygdala. studied with a variety of experimental techniques (cf. Gloor, 1960). From the anatomical point of view MATERIAL AND METHODS attention has been paid mainly to the efferent connexions of these nuclei (Adey and Meyer, 1952; The brains of 26 rats in which a variety of stereotactic or Lammers and Lohman, 1957; Hall, 1960; Nauta, surgical lesions had been placed in the diencephalon and and it is now that there basal forebrain areas were used in this study. Following 1961), generally accepted survival periods of five to seven days the animals were are two main efferent pathways from the amygdala, perfused with 10 % formol-saline and after further the well-known stria terminalis and a more diffuse fixation the brains were either embedded in paraffin wax ventral pathway, a component of the longitudinal or sectioned on a freezing microtome. All the brains were association bundle of the amygdala. It has not cut in the coronal plane, and from each a regularly spaced generally been recognized, however, that in studying series was stained, the paraffin sections according to the Protected by copyright. the efferent connexions of the amygdala it is essential original Nauta and Gygax (1951) technique and the frozen first to exclude a contribution to these pathways sections with the conventional Nauta (1957) method. -

The Human Thalamus Is an Integrative Hub for Functional Brain Networks
5594 • The Journal of Neuroscience, June 7, 2017 • 37(23):5594–5607 Behavioral/Cognitive The Human Thalamus Is an Integrative Hub for Functional Brain Networks X Kai Hwang, Maxwell A. Bertolero, XWilliam B. Liu, and XMark D’Esposito Helen Wills Neuroscience Institute and Department of Psychology, University of California, Berkeley, Berkeley, California 94720 The thalamus is globally connected with distributed cortical regions, yet the functional significance of this extensive thalamocortical connectivityremainslargelyunknown.Byperforminggraph-theoreticanalysesonthalamocorticalfunctionalconnectivitydatacollected from human participants, we found that most thalamic subdivisions display network properties that are capable of integrating multi- modal information across diverse cortical functional networks. From a meta-analysis of a large dataset of functional brain-imaging experiments, we further found that the thalamus is involved in multiple cognitive functions. Finally, we found that focal thalamic lesions in humans have widespread distal effects, disrupting the modular organization of cortical functional networks. This converging evidence suggests that the human thalamus is a critical hub region that could integrate diverse information being processed throughout the cerebral cortex as well as maintain the modular structure of cortical functional networks. Key words: brain networks; diaschisis; functional connectivity; graph theory; thalamus Significance Statement The thalamus is traditionally viewed as a passive relay station of information from sensory organs or subcortical structures to the cortex. However, the thalamus has extensive connections with the entire cerebral cortex, which can also serve to integrate infor- mation processing between cortical regions. In this study, we demonstrate that multiple thalamic subdivisions display network properties that are capable of integrating information across multiple functional brain networks. Moreover, the thalamus is engaged by tasks requiring multiple cognitive functions. -
Basal Ganglia Anatomy, Physiology, and Function Ns201c
Basal Ganglia Anatomy, Physiology, and Function NS201c Human Basal Ganglia Anatomy Basal Ganglia Circuits: The ‘Classical’ Model of Direct and Indirect Pathway Function Motor Cortex Premotor Cortex + Glutamate Striatum GPe GPi/SNr Dopamine + - GABA - Motor Thalamus SNc STN Analagous rodent basal ganglia nuclei Gross anatomy of the striatum: gateway to the basal ganglia rodent Dorsomedial striatum: -Inputs predominantly from mPFC, thalamus, VTA Dorsolateral striatum: -Inputs from sensorimotor cortex, thalamus, SNc Ventral striatum: Striatal subregions: Dorsomedial (caudate) -Inputs from vPFC, hippocampus, amygdala, Dorsolateral (putamen) thalamus, VTA Ventral (nucleus accumbens) Gross anatomy of the striatum: patch and matrix compartments Patch/Striosome: -substance P -mu-opioid receptor Matrix: -ChAT and AChE -somatostatin Microanatomy of the striatum: cell types Projection neurons: MSN: medium spiny neuron (GABA) •striatonigral projecting – ‘direct pathway’ •striatopallidal projecting – ‘indirect pathway’ Interneurons: FS: fast-spiking interneuron (GABA) LTS: low-threshold spiking interneuron (GABA) LA: large aspiny neuron (ACh) 30 um Cellular properties of striatal neurons Microanatomy of the striatum: striatal microcircuits • Feedforward inhibition (mediated by fast-spiking interneurons) • Lateral feedback inhibition (mediated by MSN collaterals) Basal Ganglia Circuits: The ‘Classical’ Model of Direct and Indirect Pathway Function Motor Cortex Premotor Cortex + Glutamate Striatum GPe GPi/SNr Dopamine + - GABA - Motor Thalamus SNc STN The simplified ‘classical’ model of basal ganglia circuit function • Information encoded as firing rate • Basal ganglia circuit is linear and unidirectional • Dopamine exerts opposing effects on direct and indirect pathway MSNs Basal ganglia motor circuit: direct pathway Motor Cortex Premotor Cortex Glutamate Striatum GPe GPi/SNr Dopamine + GABA Motor Thalamus SNc STN Direct pathway MSNs express: D1, M4 receptors, Sub. -

Aversive Stimuli Drive Hypothalamus-To-Habenula
Aversive stimuli drive hypothalamus-to-habenula excitation to promote escape behavior Salvatore Lecca, Frank Meye, Massimo Trusel, Anna Tchenio, Julia Harris, Martin Karl Schwarz, Denis Burdakov, F Georges, Manuel Mameli To cite this version: Salvatore Lecca, Frank Meye, Massimo Trusel, Anna Tchenio, Julia Harris, et al.. Aversive stimuli drive hypothalamus-to-habenula excitation to promote escape behavior. eLife, eLife Sciences Publication, 2017, 6, pp.e30697. 10.7554/eLife.30697. hal-03129952 HAL Id: hal-03129952 https://hal.archives-ouvertes.fr/hal-03129952 Submitted on 3 Feb 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. SHORT REPORT Aversive stimuli drive hypothalamus-to- habenula excitation to promote escape behavior Salvatore Lecca1,2, Frank Julius Meye1,3, Massimo Trusel1,2, Anna Tchenio1,2, Julia Harris4, Martin Karl Schwarz5, Denis Burdakov4, Francois Georges6,7, Manuel Mameli1,2* 1Institut du Fer a` Moulin, Inserm UMR-S 839, Paris, France; 2Department of Fundamental Neuroscience, The University of Lausanne, Lausanne, Switzerland; -

The Thalamus: Gateway to the Mind Lawrence M
Overview The thalamus: gateway to the mind Lawrence M. Ward∗ The thalamus of the brain is far more than the simple sensory relay it was long thought to be. From its location at the top of the brain stem it interacts directly with nearly every part of the brain. Its dense loops into and out of cortex render it functionally a seventh cortical layer. Moreover, it receives and sends connections to most subcortical areas as well. Of course it does function as a very sophisticated sensory relay and thus is of vital importance to perception. But also it functions critically in all mental operations, including attention, memory, and consciousness, likely in different ways for different processes, as indicated by the consequences of damage to its various nuclei as well as by invasive studies in nonhuman animals. It plays a critical role also in the arousal system of the brain, in emotion, in movement, and in coordinating cortical computations. Given these important functional roles, and the dearth of knowledge about the details of its nonsensory nuclei, it is an attractive target for intensive study in the future, particularly in regard to its role in healthy and impaired cognitive functioning. © 2013 John Wiley & Sons, Ltd. How to cite this article: WIREs Cogn Sci 2013. doi: 10.1002/wcs.1256 INTRODUCTION and other animals can do quite well without major chunks of cortex. Indeed, decorticate rats behave very pen nearly any textbook of neuroscience or similarly to normal rats in many ways,2 whereas sensation and perception and you will find the O de-thalamate rats die. -

Imaging of the Confused Patient: Toxic Metabolic Disorders Dara G
Imaging of the Confused Patient: Toxic Metabolic Disorders Dara G. Jamieson, M.D. Weill Cornell Medicine, New York, NY The patient who presents with either acute or subacute confusion, in the absence of a clearly defined speech disorder and focality on neurological examination that would indicate an underlying mass lesion, needs to be evaluated for a multitude of neurological conditions. Many of the conditions that produce the recent onset of alteration in mental status, that ranges from mild confusion to florid delirium, may be due to infectious or inflammatory conditions that warrant acute intervention such as antimicrobial drugs, steroids or plasma exchange. However, some patients with recent onset of confusion have an underlying toxic-metabolic disorders indicating a specific diagnosis with need for appropriate treatment. The clinical presentations of some patients may indicate the diagnosis (e.g. hypoglycemia, chronic alcoholism) while the imaging patterns must be recognized to make the diagnosis in other patients. Toxic-metabolic disorders constitute a group of diseases and syndromes with diverse causes and clinical presentations. Many toxic-metabolic disorders have no specific neuroimaging correlates, either at early clinical stages or when florid symptoms develop. However, some toxic-metabolic disorders have characteristic abnormalities on neuroimaging, as certain areas of the central nervous system appear particularly vulnerable to specific toxins and metabolic perturbations. Areas of particular vulnerability in the brain include: 1) areas of high-oxygen demand (e.g. basal ganglia, cerebellum, hippocampus), 2) the cerebral white matter and 3) the mid-brain. Brain areas of high-oxygen demand are particularly vulnerable to toxins that interfere with cellular respiratory metabolism. -

Neuron Numbers Increase in the Human Amygdala from Birth to Adulthood, but Not in Autism
Neuron numbers increase in the human amygdala from birth to adulthood, but not in autism Thomas A. Avinoa, Nicole Bargera, Martha V. Vargasa, Erin L. Carlsona, David G. Amarala,b,c, Melissa D. Baumana,b, and Cynthia M. Schumanna,1 aDepartment of Psychiatry and Behavioral Sciences, UC Davis MIND Institute, School of Medicine, University of California, Davis, Sacramento, CA 95817; bCalifornia National Primate Research Center, University of California, Davis, CA 95616; and cCenter for Neuroscience, University of California, Davis, CA 95618 Edited by Joseph E. LeDoux, New York University, New York, NY, and approved March 1, 2018 (received for review February 12, 2018) Remarkably little is known about the postnatal cellular develop- process, however, may also make the amygdala more susceptible ment of the human amygdala. It plays a central role in mediating to developmental or environmental insults. emotional behavior and has an unusually protracted development ASD is characterized by impairments in social communication well into adulthood, increasing in size by 40% from youth to combined with restricted interests and behaviors. Alterations in adulthood. Variation from this typical neurodevelopmental trajec- amygdala growth can be detected as early as 2 y of age (23–26) tory could have profound implications on normal emotional devel- and persist into late childhood (5, 27). The severity of the indi- vidual’s social and communicative symptoms positively correlates opment. We report the results of a stereological analysis of the – number of neurons in amygdala nuclei of 52 human brains ranging with amygdala enlargement, suggesting a potential structure from 2 to 48 years of age [24 neurotypical and 28 autism spectrum function relationship (23). -

Tonic Activity in Lateral Habenula Neurons Promotes Disengagement from Reward-Seeking Behavior
bioRxiv preprint doi: https://doi.org/10.1101/2021.01.15.426914; this version posted January 16, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Tonic activity in lateral habenula neurons promotes disengagement from reward-seeking behavior 5 Brianna J. Sleezer1,3, Ryan J. Post1,2,3, David A. Bulkin1,2,3, R. Becket Ebitz4, Vladlena Lee1, Kasey Han1, Melissa R. Warden1,2,5,* 1Department of Neurobiology and Behavior, Cornell University, Ithaca, NY 14853, USA 2Cornell Neurotech, Cornell University, Ithaca, NY 14853 USA 10 3These authors contributed equally 4Department oF Neuroscience, Université de Montréal, Montréal, QC H3T 1J4, Canada 5Lead Contact *Correspondence: [email protected] 15 Sleezer*, Post*, Bulkin* et al. 1 of 38 bioRxiv preprint doi: https://doi.org/10.1101/2021.01.15.426914; this version posted January 16, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. SUMMARY Survival requires both the ability to persistently pursue goals and the ability to determine when it is time to stop, an adaptive balance of perseverance and disengagement. Neural activity in the 5 lateral habenula (LHb) has been linked to aversion and negative valence, but its role in regulating the balance between reward-seeking and disengaged behavioral states remains unclear.