Investigation of an Extensive Outbreak of HIV Infection Among Children in Sindh, Pakistan: Protocol for a Matched Case–Control Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pakistan Multi-Sectoral Action for Nutrition Program
SFG3075 REV Public Disclosure Authorized Pakistan Multi-Sectoral Action for Nutrition Program Public Disclosure Authorized Environmental and Social Management Framework (ESMF) Directorate of Urban Policy & Strategic Planning, Planning & Public Disclosure Authorized Development Department, Government of Sindh Final Report December 2016 Public Disclosure Authorized Environmental and Social Management Framework Final Report Executive Summary Local Government and Housing Town Planning Department, GOS and Agriculture Department GOS with grant assistance from DFID funded multi donor trust fund for Nutrition in Pakistan are planning to undertake Multi-Sectoral Action for Nutrition (MSAN) Project. ESMF Consultant1 has been commissioned by Directorate of Urban Policy & Strategic Planning to fulfil World Bank Operational Policies and to prepare “Environmental and Social Management Framework (ESMF) for MSAN Project” at its inception stage via assessing the project’s environmental and social viability through various environmental components like air, water, noise, land, ecology along with the parameters of human interest and mitigating adverse impacts along with chalking out of guidelines, SOPs, procedure for detailed EA during project execution. The project has two components under Inter Sectoral Nutrition Strategy of Sindh (INSS), i) the sanitation component of the project aligns with the Government of Sindh’s sanitation intervention known as Saaf Suthro Sindh (SSS) in 13 districts in the province and aims to increase the number of ODF villages through certification while ii) the agriculture for nutrition (A4N) component includes pilot targeting beneficiaries for household production and consumption of healthier foods through increased household food production in 20 Union Councils of 4 districts. Saaf Suthro Sindh (SSS) This component of the project will be sponsored by Local Government and Housing Town Planning Department, Sindh and executed by Local Government Department (LGD) through NGOs working for the Inter-sectoral Nutrition Support Program. -

4 Chronology of Disaster in Pakistan 2012 (25Th August-15Th October)
Strengthening Participatory Organization (SPO) SPO is one of the largest rights-based civil society organization in Pakistan. It is pursuing various program components presently being implemented in over 75 districts of the country. SPO seeks to address mainly governance, social and political issues in the country through its programmes focussing on democratic th governance, social justice, peace and harmony, institutional strengthening, conflict resolution, citizens engagement, gender, electoral reforms and political parties development. Parallel to these activities, SPO deals with humanitarian 15August - October) emergencies resulting from both natural and human-induced hazards. In th emergencies, it has been dealing to redress problems of disaster like (25 earthquakes, rain-fed floods, cyclones and rehabilitation of internally displaced communities affected by conflicts. Chronology of Disaster in Pakistan 2012 Protection and promotion of human rights is central to the program philosophy of SPO. Its various citizens voices and accountability initiatives seek to strengthen democratic processes through engagement with and building capacities of civil society and state institutions and harness mutual tolerance, peace and harmony between various political, ethnic and religious groups across rural and urban parts of the country. Various components of SPO's citizens voices and accountability initiatives are currently supported by Australian Agency for International Development (AusAid), British High Commission (BHC), Embassy for the Kingdom of Netherlands (EKN), DFID and USAID. SPO also acknowledges support from other donors for its various program components SPO National Center 30-A, Nazimuddin Road, F-10/4, Islamabad, Pakistan UAN: +92-51-111-357-111 Tel: +92-51-2104677, 2104679 Fax: +92-51-2112787 [email protected] www.spopk.org BALOCHISTAN KHYBER PAKHTUNKHWA PUNJAB SINDH AZAD JAMMU KASHMIR QUETTA PESHAWAR MULTAN HYDERABAD MUZAFFARABAD House 58-A, Near Pak Japan House 15, Street 1, Sector N-4 House 339-340, Block-D Plot 158/2, Behind M. -
Copy of Compiled List Phone Nos BISP ALL Regions Dated 21.05
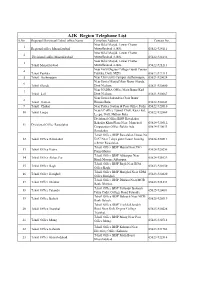
AJK Region Telephone List S.No Regioanl/Divisioanl/Tehsil office Name Complete Address Contact No. Near Bilal Masjid, Lower Chatter 1 Regional office Muzaffarabad Muzaffarabad AJ&K. 05822-924111 Near Bilal Masjid, Lower Chatter 2 Divisional office Muzaffarabad Muzaffarabad AJ&K. 05822-924132 Near Bilal Masjid, Lower Chatter 3 Tehsil Muzaffarabad Muzaffarabad AJ&K. 05822-921213 Near Girls Degree College Gandi Peeran 4 Tehsil Patikka Patikka, Distt. MZD. 05822-922113 5 Tehsil Authmaqam Near University Campus Authamaqam, 05821-920024 Near Jamia Masjid Main Bazar Sharda, 6 Tehsil Sharda Distt Neelum. 05821-920800 Near NADRA Office Main Bazar Kail 7 Tehsil kail Distt Neelum. 05821-920667 Near Jamia Sakandria Chok Bazar 8 Tehsil Hattian Hattian Bala. 05822-922643 9 Tehsil Chakar Near Police Station & Post Office Pothi 05822-922010 NearAC office Tunnel Chok, Kaser kot, 10 Tehsil Leepa 05822-922869 Leepa, Distt. Hattian Bala. Divisional Office BISP Rawalakot Bahadar Khan Plaza Near Muncipal 05824-920512, 11 Divisional Office Rawalakot Corporation Office Baldia Ada 05824-920033 Rawalakot. Tehsil Office BISP Rawalakot House No 12 Tehsil Office Rawalakot D-97 Near 7 days guest house housing 05824-920511 scheme Rawalakot. Tehsil Office BISP Hajira Near PSO 13 Tehsil Office Hajira 05824-920256 Pump Hajira. Tehsil Office BISP Abbaspur Near 14 Tehsil Office Abbas Pur 05824-921029 Hanfi Mosque Abbaspur. Tehsil Office BISP Bagh Near BDA 15 Tehsil Office Bagh 05823-920150 Office Bagh. Tehsil Office BISP Harighel Near SDM 16 Tehsil Office Harighel 05823-920820 Office Harighel. Tehsil Office BISP Dhirkot Near MCB 17 Tehsil Office Dhirkot 05823-921233 Bank Dhirkot. Tehsil Office BISP Pallandri Balouch 18 Tehsil Office Palandri 05825-920081 Palza Cadet College Road Palandri. -

Discrimination Against Religious Minorities in Pakistan: an Analysis of Federal and Provincial Laws
DISCRIMINATION AGAINST RELIGIOUS MINORITIES IN PAKISTAN: AN ANALYSIS OF FEDERAL AND PROVINCIAL LAWS Preface This research paper is part of a large project designed to examine the state of freedom of religion and belief in Pakistan and the problems faced by religious minorities. The project is to be executed by a consortium of six civil society organizations – the Human Rights Commission of Pakistan (HRCP), AGHS Legal Aid Cell, Catholic Commission for Justice and Peace (CCJP), Simorgh, Faiz Foundation Trust, and Centre for Civic Education (CCE). The project’s justification lies in Pakistan’s need to provide institutional guarantees for the fundamental rights of religious minorities including their primary right to enjoy freedom of religion and belief. The fact that for years minority communities have been suffering a decline in the scale of rights available to them lends special urgency to the project. The project is also important because it focuses on an issue which does not only concern the people of Pakistan (those belonging to the majority (Muslim) as well as minority communities), but also affects the future of religious minorities in India and the relations between the two South Asian neighbours. The Lahore Resolution of 1940, which provided the basis for the division of India in 1947 into two independent states of India and Pakistan, had two parts. While the first part demanded the grant of statehood to territories where the Muslims were in majority, the second part dealt with safeguards for the rights of religious minorities which the two authorities succeeding the British administration were supposed to guarantee. -

2013-2014 Development Budget
1 SC22051(051) DEVELOPMENT (REVENUE) Rs Charged: ______________ Voted: 33,098,087,000 ______________ Total: 33,098,087,000 ______________ ____________________________________________________________________________________________ AGRICULTURE DEPARTMENT ____________________________________________________________________________________________ AGRICULTURE RESEARCH ____________________________________________________________________________________________ P./ADP DDO Functional-Cum-Object Classification & Budget NO. NO. Particular Of Scheme Estimates 2013 - 2014 ____________________________________________________________________________________________ Rs 04 ECONOMIC AFFAIRS 042 AGRI,FOOD,IRRIGATION,FORESTRY & FISHING 0421 AGRICULTURE 042103 AGRICULTURAL RESEARCH & EXTENSION SERVIC HD9337 DIRECTOR GENERAL AGRICULTURE RESEARCH SINDH. ADP No : 0001 HD09100137 Development and Promotion of Quality Seed through Public 134,896,000 Private Partnership in Sindh A03970 Others 134,896,000 TA9384 DY.DIRECTOR RICE RESEARCH STATION THATTA ADP No : 0002 TA12131410 Rehabilitation of Rice & Cotton Research Station Thatta 34,826,000 A03970 Others 34,826,000 KR9613 SECRETARY AGRICULTURE ADP No : 0003 HD12138010 Establishment of Agriculture Services Complex and Advisory 10,520,000 Centers in Sindh A03970 Others 10,520,000 HD9337 DIRECTOR GENERAL AGRICULTURE RESEARCH SINDH. ADP No : 0004 KA11120007 Development of Bio - Pesticide for mangement of vegetable 9,414,000 pests. A03970 Others 9,414,000 LA9404 DIRECTOR QUAID-E-AWAM ARI LARKANA ADP No : 0005 LA11120008 -
Province Wise Provisional Results of Census - 2017
PROVINCE WISE PROVISIONAL RESULTS OF CENSUS - 2017 ADMINISTRATIVE UNITS POPULATION 2017 POPULATION 1998 PAKISTAN 207,774,520 132,352,279 KHYBER PAKHTUNKHWA 30,523,371 17,743,645 FATA 5,001,676 3,176,331 PUNJAB 110,012,442 73,621,290 SINDH 47,886,051 30,439,893 BALOCHISTAN 12,344,408 6,565,885 ISLAMABAD 2,006,572 805,235 Note:- 1. Total Population includes all persons residing in the country including Afghans & other Aliens residing with the local population 2. Population does not include Afghan Refugees living in Refugee villages 1 PROVISIONAL CENSUS RESULTS -2017 KHYBER PAKHTUNKHWA District Tehsil POPULATION POPULATION ADMN. UNITS / AREA Sr.No Sr.No 2017 1998 KHYBER PAKHTUNKHWA 30,523,371 17,743,645 MALAKAND DIVISION 7,514,694 4,262,700 1 CHITRAL DISTRICT 447,362 318,689 1 Chitral Tehsil 278,122 184,874 2 Mastuj Tehsil 169,240 133,815 2 UPPER DIR DISTRICT 946,421 514,451 3 Dir Tehsil 439,577 235,324 4 *Shringal Tehsil 185,037 104,058 5 Wari Tehsil 321,807 175,069 3 LOWER DIR DISTRICT 1,435,917 779,056 6 Temergara Tehsil 520,738 290,849 7 *Adenzai Tehsil 317,504 168,830 8 *Lal Qilla Tehsil 219,067 129,305 9 *Samarbagh (Barwa) Tehsil 378,608 190,072 4 BUNER DISTRICT 897,319 506,048 10 Daggar/Buner Tehsil 355,692 197,120 11 *Gagra Tehsil 270,467 151,877 12 *Khado Khel Tehsil 118,185 69,812 13 *Mandanr Tehsil 152,975 87,239 5 SWAT DISTRICT 2,309,570 1,257,602 14 *Babuzai Tehsil (Swat) 599,040 321,995 15 *Bari Kot Tehsil 184,000 99,975 16 *Kabal Tehsil 420,374 244,142 17 Matta Tehsil 465,996 251,368 18 *Khawaza Khela Tehsil 265,571 141,193 -

Sindh Community Mobilization Program (CMP) Year III Quarterly Report III: April 1– June 30, 2016 Contract Award No: AID-391-C-13-00006
Sindh Community Mobilization Program (CMP) Year III Quarterly Report III: April 1– June 30, 2016 Contract Award No: AID-391-C-13-00006 SINDH COMMUNITY MOBILIZATION PROGRAM CMP Year III – Quarterly Report III (April 1to June 30, 2016) Photo: Group Picture during Inauguration of Government High School, Kouro Goth, District Khairpur on April 7, 2016 Date: July 29, 2016 CMP is made possible by the support of the American People through the U.S. Agency for International Development (USAID). CMP is implemented by International Relief and Development (IRD) under Contract Award No: AID-391-C-13-00006. This report was produced for review by USAID. 1 Sindh Community Mobilization Program (CMP) Year III Quarterly Report III: April 1– June 30, 2016 Contract Award No: AID-391-C-13-00006 TABLE OF CONTENT A. PROGRAM SUMMARY ............................................................................................................. 5 B. OVERVIEW OF ACHIEVEMENTS THIS REPORTING PERIOD .................................. 6 C. STATUS OF ACTIVITIES AS PER COMPONENT ........................................................... 8 COMPONENT 1: Increase Communities’ Involvement in the GOS Reform of Merging, Consolidating and Upgrading Schools ............................................................................................. 8 COMPONENT 2 – Improve Community and District Government Coordination for Increased Girls’ Enrolment ............................................................................................................................ 12 COMPONENT -

World Bank Document
Hyderabad Electric Supplv CompanY J4 E* Q-j; Public Disclosure Authorized El 503 1-I VOL. 8 HESCO 6th STG Project Environmental and Social Assessment Volume - of 2- Main Report Public Disclosure Authorized Ref.: FRT07VO3HES July 2007 Public Disclosure Authorized Public Disclosure Authorized LAN tlan Partners (Pvt.) Ltd. Suite 4, 1st Floor, 20-B Blair Center, G-8 Markaz, Islamabad Tel.: +92 (51) 225 3696-97 * Fax: +92 (51) 225 3698 * Email: [email protected] Report disclaimer: Elan Partners has prepared this document in accordance with the instructions of Hyderabad Electric Supply Company (HESCO) for its sole and specific use. Any other persons, companies, or institutions who use any information contained herein do so at their own risk. HESCO 6h STG Project (2006-07) ESA Report Executive Summary The Hyderabad Electric Supply Company (HESCO) is planning to undertake the 6 th Secondary Transmission and Grid (STG) project in various parts of its territory. HESCO is seeking financing from the World Bank (WB) for this 5-year project. In line with the prevailing legislation in the country and WB safeguard policies, an environmental and social assessment (ESA) of the project has been carried out. This document presents the report of this assessment. Study Methodology The present study was conducted using a standard methodology prescribed by national and intemational agencies. Various phases of the study included screening, scoping, data collection and compilation, stakeholder consultation, impact assessment, and report compilation. Legislative Framework The Pakistan Environmental Protection Act, 1997 (PEPA 1997) requires the proponents of every development project in the country to conduct an environmental assessment and submit its report to the relevant environmental protection agency. -

Sindh Community Mobilization Program
SINDH COMMUNITY MOBILIZATION PROGRAM CMP Year II Report (October 1 , 2014 to September 30, 2015) Quarter Four Report (July 1 to September 30, 2015) Photo: Students of Government Boys’ Primary School, Alim Khan Sirohi (Mix or co-education school) received water flasks for participation in World Environment Day event organized in their school in District Sukkur on June 5, 2015. TABLE OF CONTENTS Date: October 30, 2015 CMP is made possible by the support of the American People through the U.S. Agency for International Development (USAID).1 CMP is implemented by International Relief and Development (IRD) under Contract Award No: AID-391-C-13-00006. This report was produced for review by USAID. Sindh Community Mobilization Program (CMP) Year II, Annual/Quarter 4 Report: October 1, 2014 – September 30, 2015 Contract Award No: AID-391-C-13-00006 A. PROGRAM SUMMARY ............................................................................................................... 1 B. OVERVIEW OF ACHIEVEMENTS THIS REPORTING PERIOD ......................................... 2 C. STATUS OF ACTIVITIES AS PER COMPONENT .............................................................. 10 COMPONENT 1: Increase Communities’ Involvement in the GOS Reform of Merging, ........ 10 Consolidating, and Upgrading Schools ............................................................................................ 10 COMPONENT 2 - Improve community and district government coordination for increased girls’ enrollment ................................................................................................................................ -

Pakistan's Epi Directory
PAKISTAN’S EPI DIRECTORY Pakistan EPI Directory 2013-14 Page 1 Pakistan EPI Directory 2013-14 Page 2 ACRONYMS ACD Agricultural College Dispensary AH Army Hospital AHQ Agency Head Quarter AMS Additional Medical Superintendent ASV Assistant Superintendent Vaccination BHU Basic Health Unit CD Civil Dispensary CDC Communicable Disease Control Supervisor CH Civil Hospital CHC Community Health Centre CMC City Medical Centre CMH Child and Mother Health CRMO Chief Resident Medical Officer DCD District Council Dispensary DEO District Executive Officer DHQ District Head Quarter Hospital DMS Deputy Medical Superintendent DSV District Superintendent Vaccination EDO Executive District Officer FPC Family Planning Centre FSMO Field Supervisor Medical Officer GD Government Dispensary GH Government Hospital GRD Government Rural Dispensary Pakistan EPI Directory 2013-14 Page i GV GAVI Vaccinator IV Inspector Vaccination LHV Lady Health Vaccinator MC Medical Complex MCD Medical Complex Dispensary MCH Mother and Child Health Centre MD Modal Dispensary MO Medical Officer MS Medical Superintendent MT Medical Technician OR Outreach PC Private Clinic PH Private Hospital PPHI People's Primary Healthcare Initiative Priv. Private RD Rural Dispensary RHC Rural Health Centre RHD Rural Health Dispensary SC Senior Clerk SH&NH School, Health and Nutrition Supervisor SHC Sub Health Centre SI Sanitary Inspector SMO Senior Medical Officer SSC Social Security Centre SSD Social Security Dispensary SSH Social Security Hospital THO Taluka Health Officer Pakistan EPI Directory 2013-14 Page ii THQ Tehsil Head Quarter Hospital TSI Tehsil Sanitary Inspector UCMO Union Council Medical Officer UHU Urban Health Unit WMO Women Medical Officer Pakistan EPI Directory 2013-14 Page iii Table of Contents ACRONYMS ................................................................................................... -
Larkana Blockwise
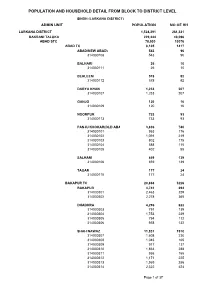
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL SINDH (LARKANA DISTRICT) ADMIN UNIT POPULATION NO OF HH LARKANA DISTRICT 1,524,391 261,331 BAKRANI TALUKA 229,444 40,096 ABAD STC 78,530 13076 ABAD TC 8,105 1417 ABAD(NEW ABAD) 543 96 314030108 543 96 BALHARI 26 10 314030111 26 10 BEHLEEM 578 92 314030112 578 92 DARYA KHAN 1,233 207 314030107 1,233 207 GANJO 120 16 314030109 120 16 NOORPUR 733 93 314030113 733 93 PANJU KHOKAR(OLD ABAD) 3,836 740 314030101 953 176 314030102 1,091 219 314030103 802 175 314030104 588 115 314030105 402 55 SALHANI 859 139 314030106 859 139 TAGAR 177 24 314030110 177 24 BAKAPUR TC 20,868 3226 BAKAPUR 4,741 694 314030301 2,463 329 314030302 2,278 365 DHADHRA 4,296 622 314030303 791 139 314030304 1,753 239 314030305 794 112 314030306 958 132 SHAH NAWAZ 11,831 1910 314030307 1,608 230 314030308 1,045 165 314030309 917 137 314030310 1,863 288 314030311 936 155 314030312 1,171 225 314030313 1,969 286 314030314 2,322 424 Page 1 of 37 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL SINDH (LARKANA DISTRICT) ADMIN UNIT POPULATION NO OF HH MAD BAHU TC 22,760 3808 FARIDABAD 11,967 1855 314030401 2,355 319 314030402 988 194 314030403 439 66 314030404 1,444 236 314030405 798 153 314030406 921 182 314030407 1,351 204 314030408 1,873 341 314030409 1,798 160 MAD BAHU 10,793 1953 314030410 1,280 222 314030411 593 106 314030412 514 63 314030413 954 167 314030414 631 116 314030415 249 43 314030416 879 179 314030417 588 114 314030418 524 85 314030419 481 74 314030420 628 107 314030421 722 123 314030422 636 -

Identification of Shift in Sowing and Harvesting Dates of Rice Crop
sustainability Article Identification of Shift in Sowing and Harvesting Dates of Rice Crop (L. Oryza sativa) through Remote Sensing Techniques: A Case Study of Larkana District Vipin Kumar Oad 1,2, Xiaohua Dong 3,4,* , Muhammad Arfan 2 , Vicky Kumar 1, Muhammad Salman Mohsin 2, Syed Saad 1, Haishen Lü 5, Muhammad Imran Azam 3 and Muhammad Tayyab 3,* 1 Department of Civil & Environmental Engineering, University Technology Petronas, Persiaran UTP, Seri Iskandar, Perak 32610, Malaysia; [email protected] (V.K.O.); [email protected] (V.K.); [email protected] (S.S.) 2 U.S.-Pakistan Center for Advanced Studies in Water (USPCAS-W), Mehran University of Engineering & Technology, Jamshoro, Sindh 76062, Pakistan; [email protected] (M.A.); [email protected] (M.S.M.) 3 College of Hydraulic and Environmental Engineering, China Three Gorges University, Yichang 443002, China; [email protected] 4 Hubei Provincial Collaborative Innovation Center for Water Security, Wuhan 430070, China 5 State Key Laboratory of Hydrology-Water Resources and Hydraulic Engineering, College of Hydrology and Water Resources, Hohai University, Nanjing 210098, China; [email protected] * Correspondence: [email protected] (X.D.); [email protected] (M.T.) Received: 25 March 2020; Accepted: 24 April 2020; Published: 28 April 2020 Abstract: The present study aimed to determine the impact of climate variability on rice crops in terms of sowing and harvesting dates and crop period. The identification of sowing and harvesting dates were spotted by mask identification, variations in land surface temperature (LST) on a temporal scale in the respective months, and a field-level social inquiry.