CAMEROON Country Operational Plan COP 2017 Strategic Direction Summary April 17, 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Review of the Evolution of Insecticide Resistance in Main Malaria Vectors in Cameroon from 1990 to 2017 Christophe Antonio-Nkondjio1,5*, N
Antonio-Nkondjio et al. Parasites & Vectors (2017) 10:472 DOI 10.1186/s13071-017-2417-9 REVIEW Open Access Review of the evolution of insecticide resistance in main malaria vectors in Cameroon from 1990 to 2017 Christophe Antonio-Nkondjio1,5*, N. Sonhafouo-Chiana2, C. S. Ngadjeu3, P. Doumbe-Belisse3, A. Talipouo3, L. Djamouko-Djonkam4, E. Kopya3, R. Bamou4, P. Awono-Ambene1 and Charles S. Wondji5 Abstract Background: Malaria remains a major public health threat in Cameroon and disease prevention is facing strong challenges due to the rapid expansion of insecticide resistance in vector populations. The present review presents an overview of published data on insecticide resistance in the main malaria vectors in Cameroon to assist in the elaboration of future and sustainable resistance management strategies. Methods: A systematic search on mosquito susceptibility to insecticides and insecticide resistance in malaria vectors in Cameroon was conducted using online bibliographic databases including PubMed, Google and Google Scholar. From each peer-reviewed paper, information on the year of the study, mosquito species, susceptibility levels, location, insecticides, data source and resistance mechanisms were extracted and inserted in a Microsoft Excel datasheet. The data collected were then analysed for assessing insecticide resistance evolution. Results: Thirty-three scientific publications were selected for the analysis. The rapid evolution of insecticide resistance across the country was reported from 2000 onward. Insecticide resistance was highly prevalent in both An. gambiae (s.l.) and An. funestus. DDT, permethrin, deltamethrin and bendiocarb appeared as the most affected compounds by resistance. From 2000 to 2017 a steady increase in the prevalence of kdr allele frequency was noted in almost all sites in An. -

MINMAP Région Du Centre SERVICES DECONCENTRES REGIONAUX ET DEPARTEMENTAUX
MINMAP Région du Centre SERVICES DECONCENTRES REGIONAUX ET DEPARTEMENTAUX N° Désignation des MO/MOD Nbre de Marchés Montant des Marchés N° page 1 Services déconcentrés Régionaux 19 2 278 252 000 4 Département de la Haute Sanaga 2 Services déconcentrés départementaux 6 291 434 000 7 3 COMMUNE DE BIBEY 2 77 000 000 8 4 COMMUNE DE LEMBE YEZOUM 8 119 000 000 8 5 COMMUNE DE MBANDJOCK 3 50 000 000 10 6 COMMUNE DE MINTA 5 152 500 000 10 7 COMMUNE DE NANGA-EBOKO 12 139 500 000 11 8 COMMUNE DE NKOTENG 5 76 000 000 13 9 COMMUNE DE NSEM 1 27 000 000 13 TOTAL 42 932 434 000 Département de la Lekié 10 Services déconcentrés départementaux 8 268 357 000 14 11 COMMUNE DE BATCHENGA 2 35 000 000 15 12 COMMUNE DE LOBO 8 247 000 000 15 13 COMMUNE DE MONATELE 11 171 500 000 16 14 COMMUNE DE SA'A 16 384 357 000 18 15 COMMUNE D'ELIG-MFOMO 7 125 000 000 20 16 COMMUNE D'EVODOULA 9 166 250 000 21 17 COMMUNE D'OBALA 14 223 500 000 22 18 COMMUNE D'OKOLA 22 752 956 000 24 19 COMMUNE D’EBEBDA 6 93 000 000 27 TOTAL 103 2 466 920 000 Département du Mbam et Inoubou 20 Services déconcentrés départementaux 4 86 000 000 28 21 COMMUNE DE BAFIA 5 75 500 000 28 22 COMMUNE DE BOKITO 12 213 000 000 29 23 COMMUNE DE KIIKI 4 134 000 000 31 24 COMMUNE DE KONYAMBETA 6 155 000 000 32 25 COMMUNE DE DEUK 2 77 000 000 33 26 COMMUNE DE MAKENENE 3 17 000 000 33 27 COMMUNE DE NDIKINIMEKI 4 84 000 000 34 28 COMMUNE D'OMBESSA 5 91 000 000 34 29 COMMUNE DE NITOUKOU 6 83 000 000 35 TOTAL 51 1 015 500 000 MINMAP/DIVISION DE LA PROGRAMMATION ET DU SUIVI DES MARCHES PUBLICS Page 1 de 88 N° Désignation -

Dictionnaire Des Villages Du Nyong Et Kellé
OFFICE 3j;E LA RECHERCHE REPUBLIQUE FEDERALE SCIEhTBFIQUE ET TECHNIQUE DU OUTRE-MER CAMEROUN CENTRE ORSTOM DE YAOUNDE DICTIO..NN,AIREDES VILLAGES DU NYONG ET KELLE (2' 6dition) D'après la documentation réuriie par la Sectioiî de Géographie de I'ORSTOM1 REPERTOIRE GEOÇRAPHIQUE DU CAMEROUN FASCICULE No 8 SH. nu 57 Avril 1970 REPERTOIRE GEOGRAPHlQUE DU CAMEROUN Fasc. I Tableau de Io population du Cameroun, 68 p. Fév. 1965 SH. NO 17 Fasc. 2 Dictionnaire des villages du Dia-et-Lobo, 89 p. Juin 1965 SH. NO 22 Fasc. 3 Dictionnaire des villages de la Haute-Sanaga, 44 p. Août 1965 SH. No 50 (2' éd. 1969 1 ' Fasc. 4 Dictionnaire des vtllages du Nyong-et-Mfoumou, 49 p. Oct'obre 1965 SH. NO 24 Fasc. 5 Dictionnaire d,es villages du Nyon;-etspo 45 p. Novembre t965 SH. No 25 Fasc. 6 Dictionneire. des villages du Ntsm 102 p. WC. 1965. SH. NO46 (2' édition Juin 1969 1 d 1% Fasc. 7 ~ictionnair. der village; de la Mefou 100; P. Jahvier 1966 SH. NOk7 1 1 1 , Fasc. 8 Dictionnaire des iillagei du Nyong-et-Ksllé, 5 1 p. Fév: 1b66 SH. 5712' éd. avril 1970 1 1 Fasc. 9 Dictionnsire ;des villages de la Lékié 7 1 p. Merr 1966~~.29. Fasc. 10 ~iction&re des villages de Kr*i 29 p. \ Man- 1965SH. Irp W (2' Bdit. octobre 1969 1 ' 5 ' , Fasc. I I Dictionnaire;diss vlllsg~sdu Mba.r(--60 p. %i 1966 Sç-! W 52 t2' édit. sept. 1969) 1 l Fasc. 12 Dictionnaire de* vfllqgbr de BQU~~~-N~O~O34 p. -

Monitoring of HIV Viral Load, CD4 Cell Count, and Clinical Assessment
Articles Monitoring of HIV viral load, CD4 cell count, and clinical assessment versus clinical monitoring alone for antiretroviral therapy in low-resource settings (Stratall ANRS 12110/ESTHER): a cost-eff ectiveness analysis Sylvie Boyer, Laura March, Charles Kouanfack, Gabrièle Laborde-Balen, Patricia Marino, Avelin Fobang Aghokeng, Eitel Mpoudi-Ngole, Sinata Koulla-Shiro, Eric Delaporte, Maria Patrizia Carrieri, Bruno Spire, Christian Laurent, Jean-Paul Moatti, on behalf of the Stratall ANRS 12110/ESTHER Study Group* Summary Background In low-income countries, the use of laboratory monitoring of patients taking antiretroviral therapy Lancet Infect Dis 2013; (ART) remains controversial in view of persistent resource constraints. The Stratall trial did not show that clinical 13: 577–86 monitoring alone was non-inferior to laboratory and clinical monitoring in terms of immunological recovery. We Published Online aimed to evaluate the costs and cost-eff ectiveness of the ART monitoring approaches assessed in the Stratall trial. April 18, 2013 http://dx.doi.org/10.1016/ S1473-3099(13)70073-2 Methods The randomised, controlled, non-inferiority Stratall trial was done in a decentralised setting in Cameroon. See Comment page 560 Between May 23, 2006, and Jan 31, 2008, ART-naive adults were randomly assigned (1:1) to clinical monitoring *Members listed at end of paper (CLIN) or viral load and CD4 cell count plus clinical monitoring (LAB) and followed up for 24 months. We INSERM, UMR912 (SESSTIM), calculated costs, number of life-years saved (LYS), and incremental cost-eff ectiveness ratios (ICERs) with data Marseille, France (S Boyer PhD, from patients who had been followed up for at least 6 months. -

Dictionnaire Des Villages Du Mbam P
OFFICE DE LA RECHERCHE REPUBliQUE FEDERALE SCIENTIFIQUE ET TECHNIQUE DU OUT,RE·MER CAMEROUN CENTRE OR5TOM DE YAOUNDE DICTIONNAIRE DES _VILLAGES DU MBAM D'après la documentation réunie par ~la Section de Géographie de l'I.R.CAM.3 REPERTQIRE GEOGRAPHIQUE DU CAMEROUN FASCICULE n° 1 1 rR-GAM 8. P. '9J SH. n° 31 YAOUNDÉ Mai 1966 REPERTOIRE GEOGRAPHIQUE DU CAMEROUN Fasc. Tableau de la population du Cameroun, 68 p. Fév. 1965 SH, N° 17 Fasc. 2 Dictionnaire des villages du Dia et Lobo, 89 p. Juin 1965 SH. N° 22 Fasc. 3 Dictionnaire des villages de la Haute-Sanaga, 53 p. Août 1965 SH. N° 23 Fasc. 4 Dictionnaire des villages du Nyong et Mfoumou, 49 p. Octobre 1965 SH. N° 24 Fasc. 5 Dictionnaire des villages du Nyong et Soo 45 p. Novembre 1965 SH. N° 25 Fasc. 6 Dictionnaire des villages du Ntem 126 p. Décembre 1965 SH. N° 26 Fasc. 7 Dictionnaire- des villages de la Mefou 108 p. Janvier 1966 SH. N° 27 Fasc. 8 Dictionnaire des villages du Nyong et Kellé 51 p. Février 1966 SH. N° 28 Fasc. 9 Dictionnaire des villages de la Lékié 71 p. Mars 1966 SH. N° 29 Fasc. 10 Dictionnaire des villages de Kribi P. Mars 1966 SH. N° 30 Fasc. 11 Dictionnaire des villages du Mbam P. 60 Mai 1966 SH. N° 31 Fasc. 12 Dictionnaire des villages de Boumba Ngoko (en préparation) Fasc. 13 ùictionnaire des villages de Lom-et-Diérem (en préparation! omCE DE LA RECHERCHE SCIENTIFIQUE RERJBLlQUE FEDERALE ET TECHNI~E OUmE-MER ID CAMEROUN _ • _cee- -- - CENTRE ORSTOM DE YAOUNDE DICTIONNAIRE ~ VILLAGES DU ...........M B A M MAI 1!66 S.R. -
Evidence of Iron Mineralization Channels in the Messondo Area (Centre-Cameroon) Using Geoelectrical (DC & IP) Methods: a Case Study
International Journal of Geosciences, 2014, 5, 346-361 Published Online March 2014 in SciRes. http://www.scirp.org/journal/ijg http://dx.doi.org/10.4236/ijg.2014.53034 Evidence of Iron Mineralization Channels in the Messondo Area (Centre-Cameroon) Using Geoelectrical (DC & IP) Methods: A Case Study Ngoumou Paul Claude1, Ndougsa-Mbarga Théophile2*, Assembe Stéphane Patrick1, Kofane Timoleon Crepin1 1Department of Physics, Faculty of Science, University of Yaoundé I, Yaoundé, Cameroon 2Department of Physics Advanced Teachers’ Training College, University of Yaoundé I, Yaoundé, Cameroon Email: *[email protected] Received 1 April 2013; revised 2 May 2013; accepted 4 June 2013 Copyright © 2014 by authors and Scientific Research Publishing Inc. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/ Abstract A geophysical survey was conducted in the Kelle-Bidjocka village, Messondo subdivision, in the Centre Region, Cameroon. The data acquisition was made by combining Schlumberger profiling and electrical soundings along six (06) profiles of 1500 m in length for a total of 64 geoelectrical stations’ survey conducted through a variable mesh 100 m × 200 m, or 100 m × 300 m. The equipment used is the DC resistivimeter Syscal Junior 48 (Iris Instrument). Processing and model- ling of field data are made by using the Res2Dinv, Qwseln and Surfer software. The investigation methods used are electrical resistivity (DC) and induced polarization (IP) methods. The analyses and interpretations have helped to highlight areas of weakness or conductive discontinuities (fractures, faults, shear zones, etc.) in Precambrian gneiss formations, sometimes undergoing weathering processes. -
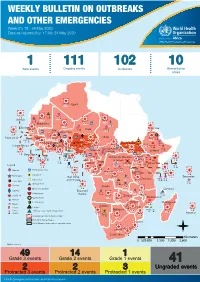
WEEKLY BULLETIN on OUTBREAKS and OTHER EMERGENCIES Week 21: 18 - 24 May 2020 Data As Reported By: 17:00; 24 May 2020
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 21: 18 - 24 May 2020 Data as reported by: 17:00; 24 May 2020 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 1 111 102 10 New events Ongoing events Outbreaks Humanitarian crises 8 306 600 Algeria 25 1 1 0 485 0 237 6 Gambia 7 0 675 60 945 61 Mauritania 13 0 1 030 65 Senegal 304 1 39 0Eritrea 3 047 35 Niger 7 635 37 Mali 380 3 Burkina Faso 95 4 0 3 7 0 Cabo Verdé Guinea 832 52 22 0 Chad 582 5 4 690 18 4 1 7 839 226 29 0 Nigeria 3 275 20Côte d’Ivoire South Sudan 1 873 895 15 604 1 274 3 32 0 Guinea-Bissau Ghana 987 202 4 400 159 7 551 92 381 12 139 0 2 0 4 0 Central African 25 0 Liberia 2 376 30 22 0 655 8 Benin Cameroon 4 732 26 Ethiopia 1 173 6 6 683 32 Republic 1 618 5 21 219 83 Sierra léone Togo 352 14 1 449 71 Uganda 120 18 Democratic Republic 812 3 339 3 14 0 401 3 1 214 51 of Congo 8 4 202 0 505 32 1 1 Congo 304 0 Gabon 3 463 2 280 Kenya 149 3 555 13 Legend 265 26 9 0 95 4 37 0 1 934 12 58 112 748 Rwanda Measles Humanitarian crisis 327 0 487 16 9 018 112 Burundi 299 9 11 0 Hepatitis E Monkeypox 42 1 2 305 66 Seychelles Sao Tome 5 0 Yellow fever Tanzania 857 0 70 0 Lassa fever and Principe 509 21 20 7 79 0 Dengue fever Cholera 1 441 37 1 043 12 Angola Ebola virus disease Comoros cVDPV2 Equatorial 83 4 2 0 Chikungunya Guinea 121 0 696 0 COVID-19 Malawi 69 4 Zambia Mozambique Guinea Worm 920 7 Anthrax Leishmaniasis Zimbabwe 2 305 18 Madagascar Malaria Namibia Floods Plague 286 1 Botswana 56 4 334 10 Cases Crimean-Congo haemorrhagic fever 236 865 226 527 2 Deaths 21 -

GE84/275 BR IFIC Nº 2893 Section Spéciale Special Section
Section spéciale Index BR IFIC Nº 2893 Special Section GE84/275 Sección especial Indice International Frequency Information Circular (Terrestrial Services) ITU - Radiocommunication Bureau Circular Internacional de Información sobre Frecuencias (Servicios Terrenales) UIT - Oficina de Radiocomunicaciones Circulaire Internationale d'Information sur les Fréquences (Services de Terre) UIT - Bureau des Radiocommunications Date/Fecha : 16.04.2019 Expiry date for comments / Fecha limite para comentarios / Date limite pour les commentaires : 25.07.2019 Description of Columns / Descripción de columnas / Description des colonnes Intent Purpose of the notification Propósito de la notificación Objet de la notification 1a Assigned frequency Frecuencia asignada Fréquence assignée 4a Name of the location of Tx station Nombre del emplazamiento de estación Tx Nom de l'emplacement de la station Tx B Administration Administración Administration 4b Geographical area Zona geográfica Zone géographique 4c Geographical coordinates Coordenadas geográficas Coordonnées géographiques 6a Class of station Clase de estación Classe de station 1b Vision / sound frequency Frecuencia de portadora imagen/sonido Fréquence image / son 1ea Frequency stability Estabilidad de frecuencia Stabilité de fréquence 1e carrier frequency offset Desplazamiento de la portadora Décalage de la porteuse 7c System and colour system Sistema de transmisión / color Système et système de couleur 9d Polarization Polarización Polarisation 13c Remarks Observaciones Remarques 9 Directivity Directividad -

Programmation De La Passation Et De L'exécution Des Marchés Publics
PROGRAMMATION DE LA PASSATION ET DE L’EXÉCUTION DES MARCHÉS PUBLICS EXERCICE 2021 JOURNAUX DE PROGRAMMATION DES MARCHÉS DES SERVICES DÉCONCENTRÉS ET DES COLLECTIVITÉS TERRITORIALES DÉCENTRALISÉES RÉGION DU CENTRE EXERCICE 2021 SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES N° Désignation des MO/MOD Nbre de Marchés Montant des Marchés N°Page 1 Services déconcentrés Régionaux 17 736 645 000 3 2 Communauté Urbaine de Yaoundé 62 10 459 000 000 5 Département de la Haute Sanaga 3 Services déconcentrés départementaux 2 24 000 000 10 4 Commune de Bibey 12 389 810 000 10 5 Commune de Lembe Yezoum 17 397 610 000 11 6 Commune de Mbandjock 12 214 000 000 12 7 Commune de Minta 8 184 500 000 12 8 Commune de Nanga Ebogo 21 372 860 000 13 9 Commune de Nkoteng 12 281 550 000 14 10 Commune de Nsem 5 158 050 000 15 TOTAL 89 2 022 380 000 Département de la Lekié 11 Services déconcentrés départementaux 9 427 000 000 16 12 Commune de Batchenga 8 194 000 000 17 13 Commune d'Ebebda 10 218 150 000 18 14 Commune d'Elig-Mfomo 8 174 000 000 19 15 Commune d'Evodoula 10 242 531 952 20 16 Commune de Lobo 11 512 809 000 21 17 Commune de Monatélé 12 288 500 000 22 18 commune d'Obala 11 147 000 000 23 19 commune d'Okola 14 363 657 000 24 20 commune de Sa'a 17 319 500 000 25 TOTAL 110 2 887 147 952 Département du Mbam et Inoubou 21 Services déconcentrés départementaux 6 144 385 000 27 22 Commune Bafia 13 213 500 000 27 23 Commune de Bokito 9 167 500 000 28 24 Commune de DEUK 17 379 500 000 29 25 Commune Kiiki 10 285 000 000 30 26 Commune Konyambeta 12 295 -

Cholera Outbreak
Emergency appeal final report Cameroon: Cholera outbreak Emergency appeal n° MDRCM011 GLIDE n° EP-2011-000034-CMR 31 October 2012 Period covered by this Final Report: 04 April 2011 to 30 June 2012 Appeal target (current): CHF 1,361,331. Appeal coverage: 21%; <click here to go directly to the final financial report, or here to view the contact details> Appeal history: This Emergency Appeal was initially launched on 04 April 2011 for CHF 1,249,847 for 12 months to assist 87,500 beneficiaries. CHF 150,000 was initially allocated from the Federation’s Disaster Relief Emergency Fund (DREF) to support the national society in responding by delivering assistance. Operations update No 1 was issued on 30 May 2011 to revise the objectives and budget of the operation. Operations update No 2 was issued on 31st May 2011 to provide financial statement against revised budget. Operations update No 3 was issued on 12 October 2011 to summarize the achievements 6 months into the operation. Operations update No 4 was issued on 29 February 2012 to extend the timeframe of the operation from 31st March to 30 June 2012 to cover the funding agreement with the American Embassy in Cameroon. PBR No M1111087 was submitted as final report of this operation to the American Embassy in Cameroon on 03 August 2012. Throughout the operation, Cameroon Red Cross volunteers sensitized the populations on PBR No M1111127 was submitted as final report of this how to avoid cholera. Photo/IFRC operation to the British Red Cross on 14 August 2012. Summary: A serious cholera epidemic affected Cameroon since 2010. -
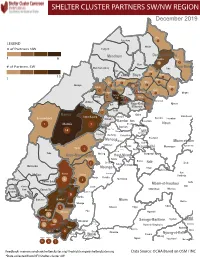
NW SW Presence Map Complete Copy
SHELTER CLUSTER PARTNERS SW/NWMap creation da tREGIONe: 06/12/2018 December 2019 Ako Furu-Awa 1 LEGEND Misaje # of Partners NW Fungom Menchum Donga-Mantung 1 6 Nkambe Nwa 3 1 Bum # of Partners SW Menchum-Valley Ndu Mayo-Banyo Wum Noni 1 Fundong Nkum 15 Boyo 1 1 Njinikom Kumbo Oku 1 Bafut 1 Belo Akwaya 1 3 1 Njikwa Bui Mbven 1 2 Mezam 2 Jakiri Mbengwi Babessi 1 Magba Bamenda Tubah 2 2 Bamenda Ndop Momo 6b 3 4 2 3 Bangourain Widikum Ngie Bamenda Bali 1 Ngo-Ketunjia Njimom Balikumbat Batibo Santa 2 Manyu Galim Upper Bayang Babadjou Malentouen Eyumodjock Wabane Koutaba Foumban Bambo7 tos Kouoptamo 1 Mamfe 7 Lebialem M ouda Noun Batcham Bafoussam Alou Fongo-Tongo 2e 14 Nkong-Ni BafouMssamif 1eir Fontem Dschang Penka-Michel Bamendjou Poumougne Foumbot MenouaFokoué Mbam-et-Kim Baham Djebem Santchou Bandja Batié Massangam Ngambé-Tikar Nguti Koung-Khi 1 Banka Bangou Kekem Toko Kupe-Manenguba Melong Haut-Nkam Bangangté Bafang Bana Bangem Banwa Bazou Baré-Bakem Ndé 1 Bakou Deuk Mundemba Nord-Makombé Moungo Tonga Makénéné Konye Nkongsamba 1er Kon Ndian Tombel Yambetta Manjo Nlonako Isangele 5 1 Nkondjock Dikome Balue Bafia Kumba Mbam-et-Inoubou Kombo Loum Kiiki Kombo Itindi Ekondo Titi Ndikiniméki Nitoukou Abedimo Meme Njombé-Penja 9 Mombo Idabato Bamusso Kumba 1 Nkam Bokito Kumba Mbanga 1 Yabassi Yingui Ndom Mbonge Muyuka Fiko Ngambé 6 Nyanon Lekié West-Coast Sanaga-Maritime Monatélé 5 Fako Dibombari Douala 55 Buea 5e Massock-Songloulou Evodoula Tiko Nguibassal Limbe1 Douala 4e Edéa 2e Okola Limbe 2 6 Douala Dibamba Limbe 3 Douala 6e Wou3rei Pouma Nyong-et-Kellé Douala 6e Dibang Limbe 1 Limbe 2 Limbe 3 Dizangué Ngwei Ngog-Mapubi Matomb Lobo 13 54 1 Feedback: [email protected]/ [email protected] Data Source: OCHA Based on OSM / INC *Data collected from NFI/Shelter cluster 4W. -

Land Use and Land Cover Changes in the Centre Region of Cameroon
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 18 February 2020 Land Use and Land Cover changes in the Centre Region of Cameroon Tchindjang Mesmin; Saha Frédéric, Voundi Eric, Mbevo Fendoung Philippes, Ngo Makak Rose, Issan Ismaël and Tchoumbou Frédéric Sédric * Correspondence: Tchindjang Mesmin, Lecturer, University of Yaoundé 1 and scientific Coordinator of Global Mapping and Environmental Monitoring [email protected] Saha Frédéric, PhD student of the University of Yaoundé 1 and project manager of Global Mapping and Environmental Monitoring [email protected] Voundi Eric, PhD student of the University of Yaoundé 1 and technical manager of Global Mapping and Environmental Monitoring [email protected] Mbevo Fendoung Philippes PhD student of the University of Yaoundé 1 and internship at University of Liège Belgium; [email protected] Ngo Makak Rose, MSC, GIS and remote sensing specialist at Global Mapping and Environmental Monitoring; [email protected] Issan Ismaël, MSC and GIS specialist, [email protected] Tchoumbou Kemeni Frédéric Sédric MSC, database specialist, [email protected] Abstract: Cameroon territory is experiencing significant land use and land cover (LULC) changes since its independence in 1960. But the main relevant impacts are recorded since 1990 due to intensification of agricultural activities and urbanization. LULC effects and dynamics vary from one region to another according to the type of vegetation cover and activities. Using remote sensing, GIS and subsidiary data, this paper attempted to model the land use and land cover (LULC) change in the Centre Region of Cameroon that host Yaoundé metropolis. The rapid expansion of the city of Yaoundé drives to the land conversion with farmland intensification and forest depletion accelerating the rate at which land use and land cover (LULC) transformations take place.