Tobacco Settlement Report: FY 2017-18
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2020 SWPONL Conference First Name Middle Last Name Degrees
2020 SWPONL Conference First name Middle Last name Degrees/Credentials Job Title Hospital / Company City, State Tammy Allison MSN, DNP Clinical Director, Education The Uniontown Hospital Uniontown, PA Heather Ambrose DNP, RN, NEA-BC, CPN Director of Nursing UPMC Presbyterian Shadyside Pittsburgh, PA Daniela Angeloni Infermiera CNO UPMC Salvator Mundi Roma, Italy Joe Archer MS, BS, RRT Territory Manager BD/BARD Pittsburgh, PA Amanda Barker Monitoring Sales Specialist Medtronic Pittsburgh, PA Lee Baron MSN, RN Assistant Vice President, Nursing Monongahela Valley Hospital Monongahela, PA Kim Bartolowits RN, MSN, NE-BC Magnet Program Director Allegheny General Hospital/AHN Pittsburgh, PA Deborah Beer DNP, RN-BC,CNE Director, Clinical & Operational UPMC Western Psychiatric Hospital Pittsburgh, PA Informatics Kimberly Belton MSN, RN Nurse Manager Allegheny General Hospital/AHN Pittsburgh, PA Janet Bischof PhD RN NE-BC CNE Director/Associate Professor Wheeling University Wheeling, WV Jodie M Blaha RN, MSN Unit Director UPMC Pittsburgh PA Jeffrey R Bomba MBA, MSN, RN, NE-BC Patient Care Manager AHN Jefferson Hospital Jefferson Hills, PA Karen Bray RN, MSN Vice-President, Patient Care Washington Health System Washington, PA Services Amy Bridgman MSN, RN-BC, CPN Advanced Clinical Education UPMC Children's Hospital of Pittsburgh Aliquippa, PA Specialist Kimberly Brooks DNP, RN Director, Education/Magnet UPMC Magee-Womens Hospital Pittsburgh, PA 2020 SWPONL Conference Angela Brown RN, MSN, CCRN Nurse Manager Allegheny General Hospital/AHN Pittsburgh, PA Kristie Bruner MSN, RN, NE-BC Nurse Manager Allegheny General Hospital/AHN Pittsburgh, PA Lisa M Bryan-Morris MSN, RN, NEA-BC Chief Nursing Officer UPMC Passavant Hospital Pittsburgh, PA Helen Burns PhD, RN, NEA-BC, FAAN Senior Vice President and Chief Excela Health Greensburg, PA Nursing Officer Diane M. -

Chapter Title
Centre County Demographics and Travel Patterns The purpose of this chapter is to describe Centre County in terms of demographics, major and minor trip generators, planning and zoning, and travel patterns. This information, when considered relative to the inventory of available transportation modes in Centre County, helps to identify specific areas that present the greatest need for transportation improvements. The large land area of Centre County (almost 1,100 square miles), and the County’s mountain ridges and valleys impact the physical layout of transportation infrastructure. Demographic indicators must also be considered within the context of these geographic attributes. Within this chapter, socioeconomic data at the census tract level from the 2010 US Census, 2009-13 American Community Survey (ACS), and the information from Chamber of Business and Industry of Centre County (CBICC) is presented relative to the following categories: • Population and Density • Vehicle Availability • Income and Poverty • Labor Force and Unemployment • Public Assistance and SSI Income • Educational Attainment • Distribution of Jobs • Distribution of Age 65 and Older Population and Social Security Income • Distribution of Disabled Population • Housing Figure 2, which is a map of census tracts within Centre County, is presented on the following page. Centre County Long Range Transportation Plan 2044 Page II- 1 Centre County Demographics & Travel Patterns Figure 2 A map of Centre County planning regions is presented on the following page as Figure 3. Planning -

Nittany Valley Fact Sheet.Pub
NITTANY VALLEY REGION UNEMPLOYMENT RATES 7.8% LABOR FORCE DATA 6.2% 5.9% 5.7% 5.5% The majority of residents from the Nittany Valley work 30 4.3% 3.6% minutes or less from their residence and drive to work. 3.8% Nittany Valley has a strong workforce with low unemployment rates. The employees are highly educated with higher percent- ages of high school graduates than the State and Nation. Bellefonte Benner Marion Spring Walker Centre PA U.S. County COMMUTING TO WORK NITTANY VALLEY EDUCATIONAL Drove to Public Worked at ATTAINMENT COMPARISON Work Carpooled Transportation Walked Other Home Bellefonte 73.3% 13.5% 2.7% 8.3% 0.5% 1.6% % Bachelor's % High School Benner 87.5% 8.7% 0.0% 0.0% 0.0% 3.8% Degree or Graduate or Marion 78.8% 11.8% 0.0% 2.1% 0.0% 7.3% Higher Higher Spring 84.1% 9.2% 0.1% 2.8% 0.8% 3.0% Walker 83.0% 11.0% 0.2% 1.7% 1.1% 3.0% U.S. 24.4% 80.4% Nittany Valley 81.1% 10.8% 0.8% 3.7% 0.6% 3.0% Pennsylvania 22.4% 81.9% Nittany Valley 18.3% 82.2% TRAVEL TIME TO WORK 30.0 LABOR FORCE POPULATION 25.0 Not in In Labor Labor 20.0 Force s Force e t u 15.0 Bellefonte 3,240 1,932 n i M Benner 1,850 2,754 10.0 Marion 512 188 Spring 3,356 1,454 5.0 Walker 1,769 767 0.0 Nittany Valley 10,727 7,095 Bellefonte Benner Marion Spring Walker Centre County Prepared by the Centre County Planning & Community Development Office, 2008 Source: U.S. -

2005 Most Wired Survey and Benchmarking Study
2012 Most Wired Survey Winners by State Alabama Cullman Regional Medical Center: Innovator Award winner Evergreen Medical Center: Most Wired–Small and Rural St. Vincent’s Hospital–Birmingham: Most Wired University of Alabama at Birmingham (UAB) Hospital: Most Wired Washington County Hospital, Chatom: Most Wired–Small and Rural Arizona Banner Health, Phoenix: Most Wired Tucson Medical Center: Most Wired Arkansas Stone County Medical Center, Mountain View: Most Wired–Small and Rural California Eisenhower Medical Center, Rancho Mirage: Most Wired Kaiser Permanente, Oakland: Most Improved Naval Hospital Lemoore: Most Wired–Small and Rural Rady Children's Hospital–San Diego: Most Wired San Francisco VA Medical Center: Most Wired Sharp HealthCare, San Diego: Most Wired Stanford Hospital and Clinics: Most Wired University of California Davis Health System, Sacramento: Most Wired University of California, San Diego Health System: Most Wired VA Palo Alto Health Care System: Most Wired VA Sierra Pacific Network, Mare Island: Most Wired Colorado Denver Health and Hospital Authority: Most Wired Poudre Valley Health System, Fort Collins: Most Wired Connecticut Hartford Hospital: Most Wired Middlesex Health System, Middletown: Most Wired MidState Medical Center, Meriden: Most Wired Saint Francis Care, Hartford: Most Wired William W. Backus Hospital, Norwich: Most Wired Yale New Haven Health System: Most Wired Delaware Alfred I. duPont Hospital for Children, Wilmington: Most Wired District of Columbia Washington, D.C. VA Medical Center: Most Wired Florida -

Residency Match List 2021
PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE 2021 Residency List – Philadelphia Campus Anesthesiology (8) Family Medicine (con’t) Cook County Health and Hosp Sys, IL Jefferson Health - Northeast, PA (2) Hospital of the Univ of Pennsylvania, PA Lankenau Medical Center, PA Indiana University SOM, IN McLaren Health Care, MI Penn State Hershey Medical Center, PA Mike O'Callaghan Federal Hospital, Tower Health/Reading Hospital, PA (2) Nellis Air Force Base/Univ of Nevada UCLA Medical Center, CA School of Medicine, NV (2)* UPMC Pinnacle Hospitals, PA Naval Hospital Jacksonville, FL* NCC - Fort Belvoir Community Hosp, VA* Emergency Medicine (28) Northwestern McGaw Lake Forest, IL Albert Einstein Medical Center, PA (2) OhioHealth-Doctors Hospital, OH Capital Health Regional Medical Center, NJ OhioHealth-Grant Medical Center, OH Christiana Care, DE Penn Medicine-Lancaster General Hosp, PA CMSRU/Cooper University Hospital, NJ Penn State Hershey Medical Center, PA Crozer-Chester Medical Center, PA (3) Puyallup Tribal Health Authority, WA Florida Atlantic University Rowan University SOM, NJ (2) -Charles E. Schmidt COM, FL Rutgers-RWJUH Somerset, NJ Geisinger Health System, PA St. Lukes Hospital, PA Harbor-UCLA Medical Center, CA St. Lukes Hospital-Anderson, PA (2) HCA Healthcare/USF Morsani GME Suburban Community Hospital, PA -Oak Hill, FL Univ of Massachusetts Med School, MA Inspira Health Network, NJ (2) UPMC McKeesport, PA Jefferson Health - Northeast, PA (2) UPMC Presbyterian Shadyside, PA Jefferson Health NJ - Rowan SOM, NJ (2) UPMC Williamsport, -
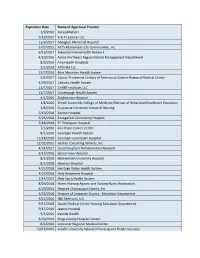
Expiration Date Name of Approved Provider 1/9/2016 Accessmatters 5
Expiration Date Name of Approved Provider 1/9/2016 AccessMatters 5/19/2017 A & T Lectures LLC 11/6/2017 Abington Memorial Hospital 5/27/2015 ACTS Retirement-Life Communities, Inc. 6/15/2017 Adventist HomeHealth Network 4/19/2016 Aetna Northeast Region Patient Management Department 8/9/2016 Aria Health Hospitals 1/1/2018 ATECAM LLC 11/7/2016 Blue Mountain Health System 5/5/2017 Cancer Treatment Centers of America at Eastern Regional Medical Center 4/29/2017 Catholic Health System 11/7/2017 CHART Institute, LLC 11/7/2017 Conemaugh Health System 4/1/2016 Doylestown Hospital 1/8/2016 Drexel University College of Medicine/Division of Behavioral Healthcare Education 1/8/2016 Duquesne University School of Nursing 5/10/2018 Easton Hospital 6/26/2018 Evangelical Community Hosptial 5/18/2018 FF Thompson Hospital 7/1/2016 Fox Chase Cancer Center 8/1/2016 Geisinger Health System 11/18/2016 Geisinger-Lewistown Hospital 12/31/2015 Gerber Consulting Services, Inc 4/24/2017 Good Shepherd Rehabilitation Network 6/15/2016 Grand View Hospital 8/2/2018 Hahnemann University Hospital 8/2/2018 Hanover Hospital 4/27/2018 Heritage Valley Health System 4/27/2018 Holy Redeemer Hospital 2/14/2017 Holy Spirit Health System 8/26/2018 Home Nursing Agency and Visiting Nurse Association 4/29/2016 Hospice Chautauqua County, Inc 6/25/2018 Hospice of Lancaster County - Education Department 9/12/2016 J&K Seminars, LLC 9/13/2018 Jacobi Medical Center Nursing Education Department 9/12/2016 Jeanes Hospital 9/3/2015 Kaleida Health 6/30/2016 Kings County Hospital Center 8/9/2016 -

The Central Pennsylvania Conference (EV) 1850-1871 Compiled from the Conference Archives
The Central Pennsylvania Conference (EV) 1850-1871 compiled from the Conference Archives I. Annual Conference Records Because of denominational unions and boundary adjustments, the Central Pennsylvania Conference of the United Methodist Church includes congregations with roots in more than a dozen distinct predecessor conferences. In order to service its constituency, the Conference Archives seeks to acquire and maintain as complete a collection as possible of the journals of these various conferences. Congregations with roots in one of the three primary Methodist Episcopal, United Brethren or Evangelical Association conferences that served central Pennsyl- vania have access to virtually complete conference records and statistics. Even in these instances, however, conference journals can be incomplete. Early journals of all the predecessor denominations list only charge statistics. While they clearly identify the pastor assigned to each charge, they do not provide information about individual churches -- nor do they even identify which churches are on which charges. Hidden within the minutes, however, are specific reports that provide valuable primary source information at the congregational level. Missionary Reports : When conferences began printing their journals, they tried to contain expenses by producing a product that many people would be willing to purchase. Including a detailed report of missionary giving proved to be the key, for people like to see their name in print -- especially when connected with noble causes. Accordingly, many conferences listed the people at each appointment on each charge who contributed to missions -- and often listed the amounts of the individual contributions. These reports not only identify what churches were on what charges, but they also identify which families attended which churches. -

Acute-Care-Hospitals-Alphabetic.Pdf
Acute Care Hospitals Facility Name Facility # Facility Name Facility # Abington Health Center - Warminster 1410-09 Barnabas Health Jersey City Medical Center 2312-70 Campus(Warminster Hospital) Barnes-Kasson Hospital 1241-58 Abington Health-Lansdale Hospital 1432-46 Barnesville Hospital - Barnesville 1012-72 Abington Memorial Hospital 1001-46 Bath VA Medical Center 1062-71 Acuity Specialty Hospital of New Jersey (LTAC) 2310-70 (within Atlanticare Reg. Med.Ctr. Atlantic City Bayhealth Hospital, Sussex Campus 1012-68 Campu Bayshore Community Hospital 1039-70 AHN Harmar Neighborhood Hospital 1465-02 Beebe Medical Center - Lewes, DE 1003-68 AHN Hempfield Neighborhood Hospital 1130-65 Bellevue Hospital Center- New York, NY 1012-71 AHN McCandless Neighborhood Hospital 1464-02 Belmont Community Hospital (The Bellaire City 1002-72 AHN Neighborhood Hospital - Brentwood 1463-02 Hospital) Akron General Medical Center 1033-72 Belmont Hospital Bel Air 1026-72 Albany Medical Center Hospital - Albany, NY 1043-71 Benedictine Hospital 1001-71 Aliquippa Community Hospital (UPMC Beaver 1002-04 Berwick Hospital Center 1013-19 Valley Hospital) Beth Israel Hospital - Newark 1035-70 Allegheny General Hospital 1184-02 Beth Israel Med Ctr-Petrie Division (Manhattan) 1057-71 Allegheny Valley Hospital (Alle-Kiski Medical 1124-02 Center) Bloomsburg Hospital 1016-19 Anne Arundel Medical Center 1035-69 Bluefield Regional Medical Center 1029-73 Ardern Hill Hospital - Goshen 1017-71 Blythedale Children's Hospital 1063-71 Aria Health - Bucks County (formerly Delaware -

And Family-Centered Care Through Learning, Engagement and Discovery
geisinger.org Symposium on Enhancing patient- and family-centered care through learning, engagement and discovery Tue., June 14, and Wed., June 15, 2016 The Henry Hood Center for Health Research Geisinger Medical Center campus This conference is supported through a Eugene Washington Engagement Patient- Centered Outcomes Research Initiative (PCORI) Award (EAIN-3012) and the Geisinger Scientific Research Committee (SRC-S-52). Symposium on Enhancing patient- and family-centered care through learning, engagement and discovery All across the United States, healthcare professionals are tackling the challenges of enhancing the quality of patient- and family- centered care. To meet those challenges, they have to form true partnerships with their colleagues, their patients and family caregivers. At Geisinger, we’re embracing these challenges. We’re working with our healthcare professionals to help them partner with their colleagues, patients and patient families, all with the aim of improving the quality and the experience of care. And we’re asking patients and their families to collaborate with Geisinger as co-improvers, co-investigators and co-innovators in our drive to realize this overarching aim. Today, we are excited to welcome you to this symposium: Enhancing Patient- and Family-Centered Care through Learning, Discovery, and Engagement. Over the next two days, we invite you to join us in exploring effective strategies for fulfilling Geisinger’s commitment to putting — and keeping — patients at the center of all we do. Our goal is to make this symposium a stunning success, and without your participation, we will not be able to attain this goal. Please accept our sincere thanks for your participation and for your past, present and future contributions to making Geisinger the best. -

1992 Comprehensive Plan
1992 SPRING TOWNSHIP COMPREHENSIVE PLAN Spring Township 6309 Blanckd Street Bellefonte 16823 Centre County, PA Prepared By: George L. Stallman, III, A.I.C.P. stallman & Stahlman. Inc. Engineering and Planning Y ork, Pennsylvania i SPRING TOWNSHIP OFFICIALS Township Supervisors John H. Auman. ............................... Chairman Melvin J. Zimmerman...................... Vice Chairman Samuel E. Markle ..................Secretary/Treasurer Township Staff Stellard T. Beightol, Jr ..... Code Enforcement Officer Miller, Kistler, & Campbell .................Solicitor Sweetland Engineering ........................ Engineer Glace Associates...... ..............Alternate Engineer Korena DeFurio ......................... Township Clerk Molly Patton ........................... Township Clerk Planning Commission Rodney Musser..... ........................... Chairman James I. Smith........ ..................Vice Chairman Linda Lowe .................................. Secretary Michael Bonchack William MacMath William H. Weaver, I11 NITTANY VALLEY JOINT COMPREHENSIVE PLANNING INITIATIVE Under the guidance of Attorney Ben Novak, seven Centre County Municipalities joined together in 1988 with the goal of updating their Comprehensive Plans and Zoning Ordinances. They were: J Bellefonte Borough J Benner Township J Centre Hall Borough J Marion Township J Port Matilda Borough J Spring Township J Walker Township Huston Township was originally part of the group, but subsequent- ly resigned and was replaced by Port Matilda Borough. Nittany Valley was selected -

A Year Ofgrowth
A Year of Growth 2013 Annual Report Sharing the wealth. Shaping the future. 1 From the Executive Director’s Desk Dear Friends, Here at Centre Foundation, we are truly “Building for the Future” and 2013 was a year that embodied that vision. We welcomed growth and transformation in our staff, our funds, our board, and our community! In December, I was honored to be named Executive Director upon the retirement of Al Jones. Earlier, we welcomed a new staff member, Irene Miller, in August. Jodi Pringle ended her very successful two- year term as board chair and has passed the gavel on to Amos Goodall. To see a complete list of our current staff – including Carrie Ryan, our new Deputy Director that joined us in March of 2014 – and Molly Kunkel board members, please see page 31. Executive Director Our assets grew 17.9% due to a dynamic combination of increased donations to existing funds, generous estate gifts through our Campbell Society, an increase in new funds established, and very strong investment returns. The full 2013 Financial Report and corresponding infographics can be found beginning on page 28. The Foundation’s ongoing support of community organizations kept growing, totaling over $10.7 million! A complete list of gifts to our funds starts on page 9, while a list of our lifetime grants to organizations begins on page 21. Sharing the wealth. Shaping the future. Centre Gives, our new granting program, completed its second year in May of 2013 and raised over half a million dollars for the participating organizations. More details can be found on page 12. -

HERITAGE DRIVING TOUR an Ironworks That Provided Half of the Iron Used in America in the 1850S
Overlooking Penns Valley in 1764, James Potter exclaimed to his traveling companion,“My Heavens, Happy Valley Agriculture Thompson, I have discovered an empire.” He soon began carving one out, which ultimately led to HERITAGE DRIVING TOUR an ironworks that provided half of the iron used in America in the 1850s. As ironmaking moved on, the deforested land used for charcoal was transformed into farmland, making Pennsylvania the breadbasket of America. As the transition occurred, Centre County community leaders In some places in Happy Valley, it appears as if time has stopped. started the Farmers’ High School in 1855 to improve the quality of Family farms still spread gently over the serene landscape as far as farming. Today, Centre County has more than 1,000 farms and boasts the eye can see, dotted with historical communities founded nearly agricultural history dating back to the state’s earliest years. The 250 years ago. The Happy Valley Agriculture Heritage Driving Tour Farmers’ High School became the Pennsylvania State University, takes you on the area’s most beautiful roads, lined with working which remains a place where agricultural innovations and farming farms, Amish homesteads and family restaurants sourcing their improvements are made every day — and the ice cream produced menus from the bountiful local harvests. Along the way, you can there is still the best you can taste. explore our rich agricultural history while taking a well-deserved Accommodations time out from the hectic pace of life. To complement your agricultural experience, Happy Valley offers a number of cozy bed and breakfast options, both in rural settings where wildlife abounds and in our historical towns.