Task Shifting in Uganda: Case Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Ethiopia's Kechene Jewish Community
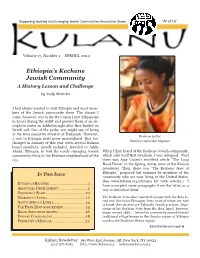
Supporting Isolated and Emerging Jewish Communities Around the Globe “All of Us” Volume 17, Number 1 SPRING, 2010 Ethiopia’s Kechene Jewish Community A History Lesson and Challenge by Judy Manelis I had always wanted to visit Ethiopia and meet mem- bers of the Jewish community there. The closest I came, however, was in the 80’s when I met Ethiopians in Israel during the airlift and greeted them at an ab- sorption center in Ashkelon right after they landed on Israeli soil. One of the perks, you might say, of being at the time executive director of Hadassah. However, Kechene potter a visit to Ethiopia itself never materialized. That fact Photo by Laura Alter Klapman changed in January of this year when several Kulanu board members, myself included, traveled to Addis Ababa, Ethiopia, to visit the newly emerging Jewish When I first heard of the Kechene Jewish community, community living in the Kechene neighborhood of the which calls itself Beit Avraham, I was intrigued. First city. there was Amy Cohen’s excellent article “The Long Road Home” in the Spring, 2009, issue of the Kulanu newsletter. Then, there was “The Kechene Jews of Ethiopia,” prepared last summer by members of the IN THIS ISSUE community who are now living in the United States. (See www.kulanu.org/ethiopia for both articles.) I ETHIOPIA ’S K E CH E N E .....................................1 have excerpted some paragraphs from the latter as a ABAYUDAYA DE V E LOPM E NT ............................2 way to introduce them: SURINAM E ’S RABBI ......................................10 ZIMBABW E ’S L E MBA .....................................12 The Kechene Jews share ancestral origins with the Beta Is- rael and, like those Ethiopian Jews, most of whom are now SOUTH AFRICA ’S LE MBA ...............................14 in Israel, they observe pre-Talmudic Jewish practices. -

LCSH Section J
J (Computer program language) J. I. Case tractors Thurmond Dam (S.C.) BT Object-oriented programming languages USE Case tractors BT Dams—South Carolina J (Locomotive) (Not Subd Geog) J.J. Glessner House (Chicago, Ill.) J. Strom Thurmond Lake (Ga. and S.C.) BT Locomotives USE Glessner House (Chicago, Ill.) UF Clark Hill Lake (Ga. and S.C.) [Former J & R Landfill (Ill.) J.J. "Jake" Pickle Federal Building (Austin, Tex.) heading] UF J and R Landfill (Ill.) UF "Jake" Pickle Federal Building (Austin, Tex.) Clark Hill Reservoir (Ga. and S.C.) J&R Landfill (Ill.) Pickle Federal Building (Austin, Tex.) Clarks Hill Reservoir (Ga. and S.C.) BT Sanitary landfills—Illinois BT Public buildings—Texas Strom Thurmond Lake (Ga. and S.C.) J. & W. Seligman and Company Building (New York, J. James Exon Federal Bureau of Investigation Building Thurmond Lake (Ga. and S.C.) N.Y.) (Omaha, Neb.) BT Lakes—Georgia USE Banca Commerciale Italiana Building (New UF Exon Federal Bureau of Investigation Building Lakes—South Carolina York, N.Y.) (Omaha, Neb.) Reservoirs—Georgia J 29 (Jet fighter plane) BT Public buildings—Nebraska Reservoirs—South Carolina USE Saab 29 (Jet fighter plane) J. Kenneth Robinson Postal Building (Winchester, Va.) J.T. Berry Site (Mass.) J.A. Ranch (Tex.) UF Robinson Postal Building (Winchester, Va.) UF Berry Site (Mass.) BT Ranches—Texas BT Post office buildings—Virginia BT Massachusetts—Antiquities J. Alfred Prufrock (Fictitious character) J.L. Dawkins Post Office Building (Fayetteville, N.C.) J.T. Nickel Family Nature and Wildlife Preserve (Okla.) USE Prufrock, J. Alfred (Fictitious character) UF Dawkins Post Office Building (Fayetteville, UF J.T. -

Minneapolis Jewish Federation Hands-On Global Experience: Uganda
Minneapolis Jewish Federation Hands-On Global Experience: Uganda November 10 - 20, 2019 Minneapolis Jewish Federation Uganda Travel to Uganda with the Minneapolis Jewish Federation and Global Village Connect to meet the Jewish Community in Uganda! The Minneapolis Jewish Federation and Global Village Connect invite you to join us in Uganda to spend time with the Abayudaya, the Jews of Uganda, as part of The David Tychman Global Experiences Program! Meet the community, help the Tikkun Olam Primary School build a kitchen and an organic school farm so students can eat lunch, learn about Ugandan Jewish life and celebrate Shabbat, African style. We will be staying in eastern Uganda amid lush agricultural plains surrounded by hills and mountains. You will get to know students, teachers, and community members—and enjoy spectacular sightseeing. Average summertime temperature is a comfortable 78 F. ● Spend Shabbat in the Abayudaya community ● Help build an organic school farm and kitchen with a fuel efficient oven so students can eat lunch at school, which gives parents an incentive to send children to school. ● Use your skills to teach class ● Learn how to make challah, African style ● Make Ugandan handcrafts with the Namutumba Women’s Group ● Participate in a Goat Give with Buyanga students and their families ● Optional: Enjoy a 3-day gorilla trek or 5-day gorilla trek and wildlife safari combination add-on. jewishminneapolis.org/uganda | 2 Minneapolis Jewish Federation Uganda WHAT TO EXPECT You will receive a warm welcome and wonderful hospitality! The 2,000 Abayudaya live in eight villages in eastern Uganda in close proximity with their Christian and Muslim neighbors. -

A Foreign Policy Determined by Sitting Presidents: a Case
T.C. ANKARA UNIVERSITY GRADUATE SCHOOL OF SOCIAL SCIENCES DEPARTMENT OF INTERNATIONAL RELATIONS A FOREIGN POLICY DETERMINED BY SITTING PRESIDENTS: A CASE STUDY OF UGANDA FROM INDEPENDENCE TO DATE PhD Thesis MIRIAM KYOMUHANGI ANKARA, 2019 T.C. ANKARA UNIVERSITY GRADUATE SCHOOL OF SOCIAL SCIENCES DEPARTMENT OF INTERNATIONAL RELATIONS A FOREIGN POLICY DETERMINED BY SITTING PRESIDENTS: A CASE STUDY OF UGANDA FROM INDEPENDENCE TO DATE PhD Thesis MIRIAM KYOMUHANGI SUPERVISOR Prof. Dr. Çınar ÖZEN ANKARA, 2019 TABLE OF CONTENTS TABLE OF CONTENTS ............................................................................................ i ABBREVIATIONS ................................................................................................... iv FIGURES ................................................................................................................... vi PHOTOS ................................................................................................................... vii INTRODUCTION ...................................................................................................... 1 CHAPTER ONE UGANDA’S JOURNEY TO AUTONOMY AND CONSTITUTIONAL SYSTEM I. A COLONIAL BACKGROUND OF UGANDA ............................................... 23 A. Colonial-Background of Uganda ...................................................................... 23 B. British Colonial Interests .................................................................................. 32 a. British Economic Interests ......................................................................... -
Shabbat Program Shabbat Program
SHABBAT PROGRAM SHABBAT PROGRAM January 18 and 19, 2019 / 13 Sh’vat 5779 Parashat Beshalach Martin Luther King, Jr. Day Shabbat מִי־כָמֹכָה בָּאֵלִם ה' מִי כָּמֹכָה נֶאְדָּר בַּקֹּדֶשׁ נוֹ�א תְהִת עֹשׂ�ה פֶלֶא: "Who is like You, Eternal One, among the celestials; Who is like You, majestic in holiness, awesome in splendor, working wonders!" (Exodus 15:11) 1 Welcome to CBST! ברוכים וברוכות הבאים לקהילת בית שמחת תורה! קהילת בית שמחת תורה מקיימת קשר רב שנים ועמוק עם ישראל, עם הבית הפתוח בירושלים לגאווה ולסובלנות ועם הקהילה הגאה בישראל. אנחנו מזמינים אתכם\ן לגלוּת יהדוּת ליבראלית גם בישראל! מצאו את המידע על קהילות רפורמיות המזמינות אתכם\ן לחגוג את סיפור החיים שלכן\ם בפלאיירים בכניסה. לפרטים נוספים ניתן לפנות לרב נועה סתת: [email protected] 2 JANUARY 18, 2019 / 13 TEVET 5779 PARASHAT BESHALACH - MARTIN LUTHER KING JR. SHABBAT Program Standing on the Parted Shores Noah Aronson (Born 1983)* We Shall Overcome Melody Hineh Mah Tov הִנּ ֵה מַה טוֹב 30 Charles Albert Tindley (1851-1933)* *(Candle Blessings Abraham Wolf Binder (1895-1967 הַדְלָקַת נֵרוֹת שׁ�ל שׁ�בָּת 38 *(Shalom Aleichem Israel Goldfarb (1879-1956 שׁ�לוֹם עֲלֵיכֶם 40 קַבָּלַת שׁ�בָּת KABBALAT SHABBAT / WELCOMING SHABBAT *(Shiru Ladonai (Psalm 96) Shlomo Carlebach (1926-1994 שׁ�ֽירוּ לַה' (תהלים צו) 54 *(Yir’am Hayam (Psalm 98) Yoel Sykes (Born 1986 (תהלים צח) י��עַם הַיּ�ם 52 *Mizmor L’David (Psalm 29) Western Sephardic Melody מִזְמוֹר לְדָו�ד (תהלים כט) 62 Abayudaya Ugandan* (L'chah Dodi (Shlomo Alkabetz לְכָה דוֹדִ י 66 Chassidic* *(Tsadik Katamar (Psalm 92) Louis Lewandowski (1821-1894 -

ECFG-Uganda-2020R.Pdf
About this Guide This guide is designed to prepare you to deploy to culturally complex environments and achieve mission objectives. The fundamental information contained within will help you understand the cultural dimension of your assigned location and gain skills necessary for success. The guide consists of two parts: Part 1 introduces “Culture General,” the Uganda ECFG foundational knowledge you need to operate effectively in any global environment (Photos a courtesy of Pro Quest 2011). Part 2 presents “Culture Specific” Uganda, focusing on unique cultural features of Ugandan society and is designed to complement other pre- deployment training. It applies culture-general concepts to help increase your knowledge of your assigned deployment location. For further information, visit the Air Force Culture and Language Center (AFCLC) website at www.airuniversity.af.edu/AFCLC/ or contact AFCLC’s Region Team at [email protected]. Disclaimer: All text is the property of the AFCLC and may not be modified by a change in title, content, or labeling. It may be reproduced in its current format with the expressed permission of the AFCLC. All photography is provided as a courtesy of the US government, Wikimedia, and other sources as indicated. GENERAL CULTURE CULTURE PART 1 – CULTURE GENERAL What is Culture? Fundamental to all aspects of human existence, culture shapes the way humans view life and functions as a tool we use to adapt to our social and physical environments. A culture is the sum of all of the beliefs, values, behaviors, and symbols that have meaning for a society. All human beings have culture, and individuals within a culture share a general set of beliefs and values. -

2 Moshe Kornfeld University of Michigan the Chosen Universalists
Moshe Kornfeld University of Michigan The Chosen Universalists: Jewish Philanthropy and Youth Activism in Post-Katrina New Orleans Introduction I arrived at 6:00 pm with a bag of chips and a jar of salsa, the best potluck offering I could muster from the convenience store across the street. The email announcement for the event had read: “ALL are invited to join a ton of awesome groups who are partnering for this event! Moishe House NOLA, Jewish Newcomers, JGrad, Minyan Nahar, and LGBTQ Jewish NOLA are all so excited to get everyone together this Friday” (email correspondence, October 19, 2010). I had traveled to New Orleans earlier that week, and was eager to meet members of the youth activist community, a group that I imagined would figure prominently in my study of post-Katrina Jewish service, philanthropy, and activism. The home where the event took place, Moishe House NOLA, was the local chapter of an international not-for-profit agency dedicated to engaging Jewish young adults. The organization provides rent subsidies and programming budgets to select groups of young Jews living in cities around the world; in exchange, Moishe House residents host events for their Jewish peers. The sparsely furnished home, a second-floor duplex apartment, included a series of rooms in a row—a living room, followed by a dining room, a kitchen, and finally a large, carpeted den. The residence, presumably chosen for its expansive common spaces that could accommodate large groups, was located in the Irish Channel, an uptown New Orleans neighborhood. In the front room, a mostly empty space used for the storage of 2 bikes and shoes, the hosts had set up a table with nametag labels and promotional materials describing the various potluck sponsors. -

NHC Men's Club-Kippah Project: the Jews of Abayudaya
NHC Men’s Club-Kippah Project: The Jews of Abayudaya MITCH SPIEGEL·WEDNESDAY, AUGUST 15, 2018 The Abayudaya are a Baganda community in eastern Uganda near the town of Mbale who practice a form of Judaism. Abayudaya means “people of Judah”. They are devout in their practice, keeping kashrut, and observing Shabbat. About 100 years ago, a chieftain named; Semei Kakungulu, after studying different religions, decided to reject all the forms of biblical religions except for the Torah. He embraced his own textual interpretation of the first five books of Moses, which made him (and his followers and later their descendants) something very close to Jews. Initially, they did not convert, but rather just followed the path of Judaism. They suffered persecution under Idi Amin (in the 1970`s) and the community dwindled to 300. In 2008, the head of the community, Gershom Sizomu, came to the USA to officially convert under the auspices of the Conservative movement. The entire community then underwent a conversion and was recognized as part of the Conservative movement in 2009. As of today, most of the 2,500 members of the community have converted. These Jews are isolated and suffer from poverty. As a community they are not recognized as Jewish by Israel`s Orthodox Chief Rabbinate. NHC Men`s Club is selling Kippot made by women of Abayudaya. All proceeds will go to helping this community of Jews. Kippot are $18.00 and available for pick up in the office. Please make check out to NHC Men`s Club and write Kippah Project in the memo. -

CELEBRATE the 100TH ANNIVERSARY of the ABAYUDAYA JEWISH COMMUNITY in UGANDA 17-Day Tour of Tanzania & Uganda June 17-July 3, 2019 YOUR TRIP PLANNERS VINEYARD GLOBAL
EAST AFRICA SPIRITUAL JOURNEY FEATURING SCHOLARS-IN-RESIDENCE RABBI JEFFREY SUMMIT, Rabbi Jeff rey Summit, Ph.D., Research Professor of Music and Judaic Studies, Tufts University RICHARD SOBOL, Award-winning Photojournalist and Author of Abayudaya: The Jews of Uganda CELEBRATE THE 100TH ANNIVERSARY OF THE ABAYUDAYA JEWISH COMMUNITY IN UGANDA 17-Day Tour of Tanzania & Uganda June 17-July 3, 2019 YOUR TRIP PLANNERS VINEYARD GLOBAL Vineyard Journeys is a project of Vineyard Global A trip to Tanzania in 2015 convinced Mindy LLC, a boutique marketing consulting fi rm that to shift her consulting agency’s focus to the focuses on the global hospitality industry with international tourism industry. Ever since, a specialty in African destinations. The fi rm was Vineyard has been providing marketing services founded in 2011 by Managing Director Mindy to international and domestic properties, Harris. After more than a decade on the pulpit including Finca Rosa Blanca Resort and Coffee of both Conservative and Reform congregations, Plantation in Costa Rica, and most recently Mindy decided to hang up her cantorial hat, and Basecamp Explorer, a collection of safari move into the private sector. lodges in Kenya. Mindy has now traveled 4 Building this trip has been a labor of love times to the African continent, and has visited for Mindy – an effort to combine a passion many destinations within Uganda, Kenya and for the African landscape and a personal Tanzania, and knows the region well. relationship with Rabbi Gershom Sizomu and This trip is coordinated in collaboration with the Abayudaya into a once-in-a-lifetime travel highly respected ground operators: Uganda experience for Jewish guests from the US. -
Irving J. Fain Social Action Awards Models of Outstanding Synagogue Social Action Rac.Org/Fain Active Commitment to Social Justice Is a Hallmark of Reform Judaism
Irving J. Fain Social Action Awards Models of Outstanding Synagogue Social Action rac.org/fain Active commitment to social justice is a hallmark of Reform Judaism. That commitment has inspired Reform congregations across North America to develop and pursue a wide range of activities and programs designed l’taken et ha’olam, to mend the world. By reaching out to those in need, by forming coalitions of concern across religious and racial lines, by advocating for equality and justice, the congregations of our Movement help realize the vision of the prophets and create communities informed by that vision. Irving J. Fain was a passionate proponent of social justice and served for a decade as Chair of the Commission on Social Action of Reform Judaism. The Fain Awards, established in 1983 in his honor and memory, are awarded every two years to congregations whose work in the area of social justice is exemplary. We hope and expect that the 2015 Fain Award winners will inspire others to embark creatively and energetically on the road to justice. The Religious Action Center pursues social justice and religious liberty by mobilizing the Jewish community and serving as its advocate in Washington, D.C. The Center is led by the Commission on Social Action of the Central Conference of American Rabbis and the Union for Reform Judaism (and its affiliates) and is supported by the congregations of the Union. Award Winners Ferguson Activism Central Reform Congregation St. Louis, MO Central Reform Congregation’s clergy, lay leaders and members have been on the front lines of the Ferguson protest movement. -

A Torah Grows in Uganda
Left: Dr. Lieberman with the congregation in Putti and their new torah. Below: In the OR In 2010, Dr. Isadore “Izzy” Lieberman, an orthopedic surgeon from Plano, Texas, was on his yearly volunteer medical mission in Uganda when he discovered something remarkable. After an exhausting five and a half hour drive, he arrived in Putti, also known as the Abayudaya Jewish Community, a small village of approximately 250 people who practice Judaism and who strive to be recognized as Orthodox despite their impoverished and isolated existence. Touched by the community’s dedication to their faith, Dr. Li- eberman promised to donate a “Kosher Sefer Torah” to the village to replace their makeshift 12-inch paper version. One year later, after much hard work and $25,000 raised, Dr. Lieberman returned to Putti, torah in hand, welcomed with cheers and songs of joy. As one would expect, Putti is not the easiest place to practice Judaism. From 1971 to 1979 the infamous Ugandan dictator Idi Amin banned the religion, resulting in many converting to other faiths. In fact, Abayudaya calls itself “Remnant of Israel” because its people are the last remaining Jewish practitioners in the area. Today, the Putti Village Assistance Organization strives to work to create a sustainable community economically, ecologically and educationally. Projects include building a new henhouse that will act as a sustainable business for the village, obtaining mosquito whelmed by the need, emotions and challenges that the peo- nets to reduce the risk of malaria, promoting overall health and ple of Putti face every day. He says, “It realigns my universe. -

Abayudaya Psalms in Luganda
1 Abayudaya: Music from the Jewish People of Uganda Compiled and annotated by Jeffrey A. Summit Translations and transcription by Gershom Sizomu, J.J. Keki, Dennis Bogere, Moses Sebagabo and Jeffrey A. Summit Notes on translation and transcription: When singing psalms in Luganda, the Abayudaya make certain changes to the text of Bible. The actual performance is transcribed, followed in brackets by the printed biblical text. When translating biblical or traditional liturgical text, I give the entire text in Luganda or Hebrew followed by the entire translation of the text in English. Biblical translations are taken from Tanakh, The Holy Scriptures: The New Jewish Publication Society Translation According to the Traditional Hebrew Text (Philadelphia: The Jewish Publication Society 1988). English translations and transcriptions of Hebrew liturgical passages, are taken as indicated from Siddur Sim Shalom for Shabbat and Festivals (New York: The Rabbinic Assembly 1998) and Kol Haneshamah, Shabbat Eve (Wyncote, PA: The Reconstructionist Press 1989). When presenting translations of other songs in Luganda, Lusoga, Lugwere and Lunyole, I give interlinear translation. Orthography is contested in these languages and here I use the spelling chosen by leaders of the Abayudaya community. The Abayudaya’s Hebrew pronunciation is influenced by Luganda, where words end with a vowel. As a result, when singing in Hebrew, the Abayudya often add a vowel to the end of a word. Thus, likrat, “to welcome” becomes likrati, and olam “world,” becomes olamu. 1. “Psalm 136” Sung in Luganda 1. Leader: Mumwebaze Adonai [Mukama]; kubanga mulungi: Chorus: Kubanga okusaasira kwe kwa luberera [Verse in Luganda bible: Kubanga okusaasira kwe kubeerera emirembe gyonna.] 2.