Miotic Adie's Pupils
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Medical Diary Official Publication for the Federation of Medical Societies of Hong Kong
VOL.12 NO.9 SEPTEMBER 2007 ॷġ෫ġᚂġଉ THE HONG KONG MEDICAL DIARY OFFICIAL PUBLICATION FOR THE FEDERATION OF MEDICAL SOCIETIES OF HONG KONG www.fmshk.org Editorial Editorial Dr. Timothy YY Lai Medical Bulletin Management of Tearing in Adults Dr. Alan CK Ng Dr. Dylan DN Chan Ocular Allergy in Children Dr. Koon-man Lam Neuro-ophthalmology for General Practitioners: A Revision Dr.CarmenKMChan Normal Tension Glaucoma - a Sick Eye in a Sick Body Dr. Dexter YL Leung Retinal Complications of High Myopia Dr. Timothy YY Lai Amblyopia: An overview Dr. Wilson WK Yip Prof. Dorothy SP Fan Surgical Correction for Near Sightedness Dr. Arthur CK Cheng Traditional Chinese Medicine and Ophthalmology Dr. Jane CC Yeung Special Feature Rosiglitazone and Risk of Myocardial Infarction: Clear Danger or Dr. Norman Chan Media Hype? Clinical Quiz Clinical Quiz Dr. Helen KS Tung Society News Medical Diary of September Calendar of Events ISSN 1812 - 1691 ᚂᖒԙষΙড়ᒑȅᩧҕஶቆᜰЖ VOL.12 NO.9 SEPTEMBER 2007 Contents The Federation of Medical Societies of Hong Kong 4/F Duke of Windsor Social Service Building, Contents 15 Hennessy Road, Wanchai, Hong Kong Tel: 2527 8898 Fax: 2865 0345 Editorial President Dr. FONG To-sang, Dawson 方道生醫生 1st Vice- President Editorial 2 Dr. CHAN Chi-kuen 陳志權醫生 2nd Vice- President Dr. Timothy YY Lai Dr. LO Sze-ching, Susanna 盧時楨醫生 Hon. Secretary Dr. LO See-kit, Raymond 勞思傑醫生 Medical Bulletin Deputy Hon. Secretary Dr. CHAN Sai-kwing 陳世炯醫生 Management of Tearing in Adults 4 Hon. Treasurer Mr. LAM Lop-chi, Nelson 林立志先生 Dr.AlanCKNg Deputy Hon. Treasurer Dr. Dylan DN Chan Mr. -

Pupillary Disorders LAURA J
13 Pupillary Disorders LAURA J. BALCER Pupillary disorders usually fall into one of three major cat- cortex generally do not affect pupillary size or reactivity. egories: (1) abnormally shaped pupils, (2) abnormal pupillary Efferent parasympathetic fibers, arising from the Edinger– reaction to light, or (3) unequally sized pupils (anisocoria). Westphal nucleus, exit the midbrain within the third nerve Occasionally pupillary abnormalities are isolated findings, (efferent arc). Within the subarachnoid portion of the third but in many cases they are manifestations of more serious nerve, pupillary fibers tend to run on the external surface, intracranial pathology. making them more vulnerable to compression or infiltration The pupillary examination is discussed in detail in and less susceptible to vascular insult. Within the anterior Chapter 2. Pupillary neuroanatomy and physiology are cavernous sinus, the third nerve divides into two portions. reviewed here, and then the various pupillary disorders, The pupillary fibers follow the inferior division into the orbit, grouped roughly into one of the three listed categories, are where they then synapse at the ciliary ganglion, which lies discussed. in the posterior part of the orbit between the optic nerve and lateral rectus muscle (Fig. 13.3). The ciliary ganglion issues postganglionic cholinergic short ciliary nerves, which Neuroanatomy and Physiology initially travel to the globe with the nerve to the inferior oblique muscle, then between the sclera and choroid, to The major functions of the pupil are to vary the quantity of innervate the ciliary body and iris sphincter muscle. Fibers light reaching the retina, to minimize the spherical aberra- to the ciliary body outnumber those to the iris sphincter tions of the peripheral cornea and lens, and to increase the muscle by 30 : 1. -

Accommodation in the Holmes-Adie Syndrome by G
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.21.4.290 on 1 November 1958. Downloaded from J. Neurol. Neurosurg. Psychiat., 1958, 21, 290. ACCOMMODATION IN THE HOLMES-ADIE SYNDROME BY G. F. M. RUSSELL From the Neurological Research Unit, the National Hospital, Queen Square, London In 1936, Bramwell suggested that the title response to near and far vision respectively. But it "Holmes-Adie syndrome" be given to the clinical has also been noted that the reaction to convergence complex of a slowly reacting pupil and absent tendon may be remarkably wide in its range, considering reflexes in recognition of the descriptions by Holmes that it often follows a stage of complete paralysis (1931) and Adie (1932). Both authors had empha- (Strasburger, 1902). Not only is the reaction to sized the chief clinical features-dilatation of the convergence well preserved when compared to the pupil, apparent loss of the reaction to light, slow reaction to light, but it may in fact be excessive constriction and relaxation in response to near and (Alajouanine and Morax, 1938; Heersema and distant vision, and partial loss of the tendon reflexes. Moersch, 1939). In assessing the degree of tonicity Although the syndrome had been recognized wholly there are, therefore, two criteria: slowness ofguest. Protected by copyright. or in part many years previously (Strasburger, 1902; pupillary movement and preservation of the range Saenger, 1902; Nonne, 1902; Markus, 1906; Weill of movement. and Reys, 1926), credit must go to Adie for stressing Adler and Scheie (1940) showed that the tonic the benign nature of the disorder and distinguishing pupil constricts after the conjunctival instillation it clearly from neurosyphilis. -

Cranial Nerve Palsy
Cranial Nerve Palsy What is a cranial nerve? Cranial nerves are nerves that lead directly from the brain to parts of our head, face, and trunk. There are 12 pairs of cranial nerves and some are involved in special senses (sight, smell, hearing, taste, feeling) while others control muscles and glands. Which cranial nerves pertain to the eyes? The second cranial nerve is called the optic nerve. It sends visual information from the eye to the brain. The third cranial nerve is called the oculomotor nerve. It is involved with eye movement, eyelid movement, and the function of the pupil and lens inside the eye. The fourth cranial nerve is called the trochlear nerve and the sixth cranial nerve is called the abducens nerve. They each innervate an eye muscle involved in eye movement. The fifth cranial nerve is called the trigeminal nerve. It provides facial touch sensation (including sensation on the eye). What is a cranial nerve palsy? A palsy is a lack of function of a nerve. A cranial nerve palsy may cause a complete or partial weakness or paralysis of the areas served by the affected nerve. In the case of a cranial nerve that has multiple functions (such as the oculomotor nerve), it is possible for a palsy to affect all of the various functions or only some of the functions of that nerve. What are some causes of a cranial nerve palsy? A cranial nerve palsy can occur due to a variety of causes. It can be congenital (present at birth), traumatic, or due to blood vessel disease (hypertension, diabetes, strokes, aneurysms, etc). -

Adie Syndrome: a Case Report
J Am Board Fam Pract: first published as 10.3122/jabfm.10.6.439 on 1 November 1997. Downloaded from Adie Syndrome: A Case Report T. Micheal Sherrill, MD, and DavidJ Lutz In 1932 Adie 1 described a syndrome in which were roughly equal, and the right corneal reflex unilateral accommodation and pupillary contrac was decreased. A rapid plasma reagin was ob tion were abnormal. It typically was observed in tained and found to be negative. The patient was young women with no history or evidence of subsequently referred to an ophthalmologist for syphilis and involved a unilateral dilated pupil confirmation of the diagnosis and to rule out that was unresponsive to light. He noted that other abnormalities. Confirmation was per deep tendon reflexes were absent or markedly di formed using'a dilute solution of pilocarpine. minished in these patients. He concluded that it was "a benign disorder sui generis." We report a Discussion recent case of Adie syndrome. Patients with Adie syndrome have anisocoria characterized by a dilated pupil that is minimally Case Report reactive or unresponsive to light. Deep tendon A 37-year-old woman came to the office with reflexes (knees and ankles) are either diminished right pupil dilatation. It was noticed by a nurse or absent.2 This disorder is most often seen in for the first time earlier that morning and had not young women, who have an average age of onset been present previously according to the patient's in their 30s. It usually occurs in one eye, but oc report. The patient's only visual complaint was curs bilaterally in up to 4 percent of patients.3 mild photophobia in sunlight. -

Taking the Mystery out of Abnormal Pupils
Taking the mystery out of abnormal pupils No financial disclosures Course Title: Taking the mystery out [email protected] of abnormal pupils Lecturer: Brad Sutton, OD, FAAO Clinical Professor IU School of Optometry . •Review of Anatomy Iris anatomy Iris sphincter Iris dilator Parasympathetic pathway Sympathetic pathway Parasympathetic Pathway Parasympathetic Pathway Light stimulates the retina then impulse Four neuron arc travels with the ganglion cells through the Retina to the pretectal nucleus in the chiasm into the optic tracts. 80% go to the midbrain (1) LGN , 20% to the pretectal nuclei.They Pretectal nucleus to the EW nucleus (2) then hemidecussate and terminate at the EW nucleus EW nucleus to the ciliary ganglion (3) Ciliary ganglion to the iris sphincter with short ciliary nerves (4) 1 Points of Interest Sympathetic Pathway Within the second order neuron there are Three neuron arc 30 near response fibers for every light Posterior hypothalamus to ciliospinal response fiber. This allows for light - near center of Budge ( C8 - T2 ). (1) dissociation. Center of Budge to the superior cervical The third order neuron runs with cranial ganglion in the neck (2) nerve III from the brain stem to the ciliary Superior cervical ganglion to the dilator ganglion. Superficially located prior to the muscle (3) cavernous sinus. Points of Interest Second order neuron runs along the surface of the lung, can be affected by a Pancoast tumor Third order neuron runs with the carotid artery then with the ophthalmic division of cranial nerve V 2 APD Testing testing……………….AKA……… … APD / reverse APD Direct and consensual response Which is the abnormal pupil ? Very simple rule. -

Miotics in Closed-Angle Glaucoma
Brit. J. Ophthal. (I975) 59, 205 Br J Ophthalmol: first published as 10.1136/bjo.59.4.205 on 1 April 1975. Downloaded from Miotics in closed-angle glaucoma F. GANIAS AND R. MAPSTONE St. Paul's Eye Hospital, Liverpool The initial treatment of acute primary closed-angle Table i Dosage in Groups I, 2, and 3 glaucoma (CAG) is directed towards lowering intraocular pressure (IOP) to normal levels as Group Case no. Duration IOP Time rapidly as possible. To this end, aqueous inflow is (days) (mm. Hg) (hrs) reduced by a drug such as acetazolamide (Diamox), and aqueous outflow is increased via the trabecular I I 2 8 5 meshwork by opening the closed angle with miotics. 3 7 21 3 The use of miotics is of respectable lineage and hal- 5 '4 48 7 lowed by usage, but regimes vary from "intensive" 7 8 I4 5 9 I0 I8 6 (i.e. frequent) to "occasional" (i.e. infrequent) instilla- I I 2 12 6 tions. Finally, osmotic agents are used after a variable '3 5 20 6 interval of time if the IOP remains raised. Tlle pur- I5 '4 I8 6 pose of this paper is to investigate the value of '7 '4 i6 6 miotics in the initial treatment of CAG. I9 6 02 2 2 2 8 2I 5 Material and methods 4 20t 20 6 Twenty patients with acute primary closed-angle glau- 6 I i8 5 http://bjo.bmj.com/ coma were treated, alternately, in one of two ways 8 4 i8 5 detailed below: I0 6 I8 6 I2 I0 20 6 (I) Intravenous Diamox 500 mg. -

Drug Class Review Ophthalmic Cholinergic Agonists
Drug Class Review Ophthalmic Cholinergic Agonists 52:40.20 Miotics Acetylcholine (Miochol-E) Carbachol (Isopto Carbachol; Miostat) Pilocarpine (Isopto Carpine; Pilopine HS) Final Report November 2015 Review prepared by: Melissa Archer, PharmD, Clinical Pharmacist Carin Steinvoort, PharmD, Clinical Pharmacist Gary Oderda, PharmD, MPH, Professor University of Utah College of Pharmacy Copyright © 2015 by University of Utah College of Pharmacy Salt Lake City, Utah. All rights reserved. Table of Contents Executive Summary ......................................................................................................................... 3 Introduction .................................................................................................................................... 4 Table 1. Glaucoma Therapies ................................................................................................. 5 Table 2. Summary of Agents .................................................................................................. 6 Disease Overview ........................................................................................................................ 8 Table 3. Summary of Current Glaucoma Clinical Practice Guidelines ................................... 9 Pharmacology ............................................................................................................................... 10 Methods ....................................................................................................................................... -

Canine Red Eye Elizabeth Barfield Laminack, DVM; Kathern Myrna, DVM, MS; and Phillip Anthony Moore, DVM, Diplomate ACVO
PEER REVIEWED Clinical Approach to the CANINE RED EYE Elizabeth Barfield Laminack, DVM; Kathern Myrna, DVM, MS; and Phillip Anthony Moore, DVM, Diplomate ACVO he acute red eye is a common clinical challenge for tion of the deep episcleral vessels, and is characterized general practitioners. Redness is the hallmark of by straight and immobile episcleral vessels, which run Tocular inflammation; it is a nonspecific sign related 90° to the limbus. Episcleral injection is an external to a number of underlying diseases and degree of redness sign of intraocular disease, such as anterior uveitis and may not reflect the severity of the ocular problem. glaucoma (Figures 3 and 4). Occasionally, episcleral Proper evaluation of the red eye depends on effective injection may occur in diseases of the sclera, such as and efficient diagnosis of the underlying ocular disease in episcleritis or scleritis.1 order to save the eye’s vision and the eye itself.1,2 • Corneal Neovascularization » Superficial: Long, branching corneal vessels; may be SOURCE OF REDNESS seen with superficial ulcerative (Figure 5) or nonul- The conjunctiva has small, fine, tortuous and movable vessels cerative keratitis (Figure 6) that help distinguish conjunctival inflammation from deeper » Focal deep: Straight, nonbranching corneal vessels; inflammation (see Ocular Redness algorithm, page 16). indicates a deep corneal keratitis • Conjunctival hyperemia presents with redness and » 360° deep: Corneal vessels in a 360° pattern around congestion of the conjunctival blood vessels, making the limbus; should arouse concern that glaucoma or them appear more prominent, and is associated with uveitis (Figure 4) is present1,2 extraocular disease, such as conjunctivitis (Figure 1). -

Mydriasis Associated with Local Dysfunction of Parasympathetic Nerves in Two Dogs
NOTE Internal Medicine Mydriasis Associated with Local Dysfunction of Parasympathetic Nerves in Two Dogs Teppei KANDA1), Kazuhiro TSUJI1), Keiko HIYAMA2), Takeshi TSUKA1), Saburo MINAMI1), Yoshiaki HIKASA1), Toshinori FURUKAWA3) and Yoshiharu OKAMOTO1)* 1)Department of Veterinary Medicine, Faculty of Agriculture, Tottori University, 4–101, Koyama-minami, Tottori 680–8553, 2)Takamori Animal Hospital, 3706–2, Agarimichi, Sakaiminato, Tottori 684–0033 and 3)Department of Comparative Animal Science, College of Life Science, Kurashiki University of Science and the Arts, 2640, Tsurajima-nishinoura, Kurashiki, Okayama 712–8505, Japan. (Received 13 August 2009/Accepted 16 November 2009/Published online in J-STAGE 9 December 2009) ABSTRACT. In clinical practice, photophobia resulting from persistent mydriasis may be associated with dysfunction of ocular parasympa- thetic nerves or primary iris lesions. We encountered a 5-year-old Miniature Dachshund and a 7-year-old Shih Tzu with mydriasis, abnormal pupillary light reflexes, and photophobia. Except for sustained mydriasis and photophobia, no abnormalities were detected on general physical examination or ocular examination of either dog. We performed pharmacological examinations using 0.1% and 2% pilo- carpine to evaluate and diagnose parasympathetic denervation of the affected pupillary sphincter muscles. On the basis of the results, we diagnosed a pupillary abnormality due to parasympathetic dysfunction and not to overt primary iris lesions. The test revealed that neuroanatomic localization of the lesion was postciliary ganglionic in the first dog. KEY WORDS: autonomic nervous system, canine, mydriasis, ophthalmology, tonic pupil. J. Vet. Med. Sci. 72(3): 387–389, 2010 Mydriasis and miosis are normal physiological reactions and we report herein the clinical features, diagnosis, and that allow the eye to adjust to the level of incoming light. -
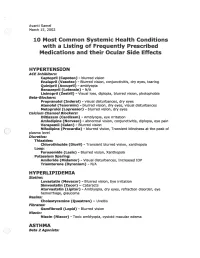
2002 Samel 10 Most Common Systemic Health Conditions with A
Avanti Samel / March 15, 2002 10 Most Common Systemic Health Conditions with a Listing of Frequently Prescribed Medications and their Ocular Side Effects HYPERTENSION ACE Inhibitors: Captopril (Capoten}- blurred vision Enalapril (Vasotec) - Blurred vision, conjunctivitis, dry eyes, tearing Quinipril (Accupril)- amblyopia Benazepril (Lotensin)- N/A Lisinopril (Zestril) - Visual loss, diplopia, blurred vision, photophobia Beta-Blockers: Propranolol (Inderal)- visual disturbances, dry eyes Atenolol (Tenormin)- blurred vision, dry eyes, visual disturbances Metoprolol (Lopressor) - blurred vision, dry eyes calcium Channel Blockers: Diltiazem (Cardizem)- Amblyopia, eye irritation Amlodipine (Norvasc)- abnormal vision, conjunctivitis, diplopia, eye pain Verapamil (Calan)- Blurred vision Nifedipine (Procardia) - blurred vision, Transient blindness at the peak of plasma level · Diuretics: Thiazides: Chlorothiazide (Diuril) - Transient blurred vision, xanthopsia Loop: Furosemide (Lasix) - Blurred vision, Xanthopsia Potassium Sparing: Amiloride (Midamor) - Visual disturbances, Increased lOP Triamterene (Dyrenium)- N/A HYPERLIPIDEMIA Statins: Lovastatin (Mevacor) - Blurred vision, Eye irritation Simvastatin (Zocor)- Cataracts Atorvastatin (Lipitor)- Amblyopia, dry eyes, refraction disorder, eye hemorrhage, glaucoma Resins: Cholestyramine (Questran)- Uveitis Fibrates: Gemfibrozil (Lopid)- Blurred vision Niacin: Niacin (Niacor) - Toxic amblyopia, cystoid macular edema ASTHMA ( ) Beta 2 Agonists: Albuterol (Proventil) - N/A ( Salmeterol (Serevent)- -

COMPLEMENTARY THERAPY ASSESSMENT VISUAL TRAINING for REFRACTIVE ERRORS August 2013
COMPLEMENTARY THERAPY ASSESSMENT VISUAL TRAINING FOR REFRACTIVE ERRORS August 2013 SUMMARY DESCRIPTION OF VISUAL TRAINING Vision training consists of a variety of programs designed to enhance visual efficiency and processing. Vision training, or orthoptics, typically addresses how well both eyes work together. Eye exercises may include, muscle relaxation techniques, biofeedback, eye patches, eye massages, the use of under-corrected prescription lenses, and/or nutritional supplements. Training is most often provided by an optometrist. BENEFITS One randomized controlled trial (RCT) of biofeedback training for control of accommodation for myopia reported no statistically significant benefits from training (Level I evidence). Another RCT (2013), which investigated vision training modalities to evaluate changes in peripheral refraction profiles in myopes, also found no evidence of benefits (Level 1 evidence). In other studies undertaken over the last 60 years, an improvement in subjective visual acuity (VA) in myopes with no corresponding improvement in objective VA has been reported (Level II/III evidence). RISKS The only risk attributable to visual training is financial. Most health insurers do not cover visual training programs. At the start of treatment, the optometrist should provide a reasonable estimate of what improvement to expect and how long it will take. CONCLUSIONS There is Level I evidence that visual training for control of accommodation has no effect on myopia. In other studies (Level II/III evidence), an improvement in subjective VA for patients with myopia that have undertaken visual training has been shown, but no corresponding physiological cause for the improvement has been demonstrated. It is postulated that the improvements in myopic patients noted in these studies were due to improvements in interpreting blurred images, changes in mood or motivation, creation of an artificial contact lens by tear film changes, or a pinhole effect from miosis of the pupil.