Hypoglycemia in Diabetes: Common, Often Unrecognized
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Treatment of Diabetes Mellitus
TREATMENT OF DIABETES MELLITUS DIABETES is a condition that affects how the body makes energy from food. Food is broken down into sugar (glucose) in the body and released into the blood. When the blood sugar level rises after a meal, insulin responds to let the sugar into the cells to be used as energy. In diabetes, the body either does not make enough insulin or it stops responding to insulin as well as it should. This results in sugar staying in the blood and leads to serious health problems over time. DIAGNOSIS OF DIABETES1 • A1C Test: Lab test measuring average blood sugar over past two to three months • Fasting Blood Sugar Test: Lab test measuring blood sugar after eight hours of no food or drink • Oral Glucose Tolerance Test (OGTT): Measures blood sugar before and two hours after drinking a specific sugary liquid • Random Blood Sugar Test: Measures blood sugar at a moment in time, without any kind of preparation (like fasting) FASTING BLOOD ORAL GLUCOSE TOLERANCE RANDOM BLOOD RESULT A1C TEST SUGAR TEST TEST SUGAR TEST Diabetes ≥ 6.5% ≥126 mg/dL ≥ 200 mg/dL ≥ 200 mg/dL Prediabetes 5.7 – 6.4% 100 – 125 mg/dL 140 – 199 mg/dL N/A Normal < 5.7% ≤99 mg/dL < 140 mg/dL N/A NON-DRUG TREATMENTS2 THERAPY COST WHAT TO EXPECT Diet (Mediterranean diet) and exercise (30 minutes a day, five days a week of moderate- Weight loss $-$$ intensity exercise); 7% weight loss decreases risk of diabetes3 Psychological intervention $$-$$$ Psychotherapy may reduce diabetic distress and improve glycemic control4,5 nationalcooperativerx.com PRESCRIPTION TREATMENTS -

295-304 Research Article Pulsatile Drug Delivery of Chitosan Co
Available online www.jocpr.com Journal of Chemical and Pharmaceutical Research, 2015, 7(12):295-304 ISSN : 0975-7384 Research Article CODEN(USA) : JCPRC5 Pulsatile drug delivery of chitosan coated beads of miglitol with fast dissolving glimepiride tablet Bhise S. H.*, Surve B. S., Aloorkar N. H., Majumdar S. H. and Kulkarni A. S. Department of Pharmaceutics, Satara College of Pharmacy, Satara, Shivaji University, Maharashtra, India _____________________________________________________________________________________________ ABSTRACT : Pulsatile drug delivery system was developed which have three parts fast dissolving tablet of glimepiride, sustained release chitosan coated microbeads of miglitol and plug of HPMC E5 and spray dried lactose. After pre- formulation studies fast dissolving tablets were prepared by direct compression method; which shows instant drug release and % CDR of glimepiride fast dissolving tablet was found to be 70.81%. polymer plug have lag time 2.30 hr, chitosan coated miglitol beads shows sustained release upto 81.66% .this system is evaluated using different physicochemical parameters and in-vitro studies. Result suggests that the system can be applicable for diabetes treatment. Key words: Pulsatile, microbeads, sustained release, miglitol, glimepiride. _____________________________________________________________________________________________ INTRODUCTION Oral controlled drug delivery systems represent the most popular form of controlled drug delivery system which release the drug with constant or variable release rates.[1] Dose of drug, reduced dosage frequency, avoidance of side effects, and improved patient compliance. However, there are certain conditions for which such a release pattern is not suitable. These conditions demand release of drug after a lag time. In other words, it is required that the drug should not be released at all during the initial phase of dosage form administration. -

Effect of the Α-Glucosidase Inhibitor Miglitol on the Glucose Profile in Japanese Type 2 Diabetic Patients Receiving Multiple Daily Insulin Injections
Endocrine Journal 2012, 59 (4), 345-352 ORIGINAL Effect of the α-glucosidase inhibitor miglitol on the glucose profile in Japanese type 2 diabetic patients receiving multiple daily insulin injections Hiroyuki Kato, Akio Ohta, Suzuko Kobayashi, Satoshi Ishii, Yukiyoshi Sada, Hidetoshi Kobayashi, Shintaro Ohmori, Akihiko Kondo, Takuyuki Katabami, Junro Fuse, Hisashi Fukuda, Yoshio Nagai and Yasushi Tanaka Department of Internal Medicine, Division of Metabolism and Endocrinology, St. Marianna University School of Medicine, Kawasaki 216-8511, Japan Abstract. Strict postprandial glycemic control may have a preventive effect on atherogenesis in patients with type 2 diabetes. The α-glucosidase inhibitor (α-GI) miglitol is useful for controlling the early postprandial increase of glucose, but the combined effect of miglitol and multiple daily insulin injections (MDI) on glucose excursion has not been evaluated. First, we retrospectively compared the daily glucose profile, evaluated by self-monitoring of blood glucose (SMBG) at nine times on the day before discharge from hospital, between type 2 diabetic patients receiving MDI (n=81) or MDI plus miglitol at 150 mg daily (n=24). Second, we prospectively examined the effect of adding miglitol to MDI on the daily glucose profile (SMBG) in 19 other type 2 diabetic patients. Although the daily insulin dosage and the glucose level before meals did not differ between the two groups, the 1-h postprandial glucose level after each meal, 2-h glucose level after lunch and dinner, mean and standard deviation of glucose, and amplitude of glucose excursion were significantly lower or smaller in the MDI plus miglitol group than in the MDI group. -

Women with Higher BMI at Lower Risk for Glaucoma
44 WOMEN'S HEALTH SEPTEMBER 1, 2010 • FAMILY PRACTICE NEWS DRUGS, PREGNANCY, AND LACTATION Use of Antidiabetic Agents During Pregnancy n a previous column, I looked at the abinese), tolazamide (Tolinase), and tolbu- thetic analogue of human amylin given was discovered. No developmental toxi- ways uncontrolled hyperglycemia tamide (Orinase). They can cause marked by subcutaneous injection, but the ani- city was observed in the newborns. Iduring pregnancy causes significant and persistent neonatal hypoglycemia if mal data suggest moderate risk (struc- Pioglitazone (Actos) and rosiglitazone toxicity for the mother, embryo, fetus, taken close to birth. To prevent this toxi- tural anomalies in rats). The drug— (Avandia), thiazolidinediones used as ad- newborn, and adolescent (“Toxicity of city, therapy should be changed to insulin which slows the rate of gastric emptying, juncts to diet and exercise, lower insulin Diabetes in Pregnancy,” December in the third trimester or, at least, several prevents a postprandial rise in plasma resistance but do not promote insulin re- 2009, p. 52). days before birth. glucagon, and promotes satiety—is best lease. Animal reproduction data suggest This column examines the The second-generation sul- avoided in pregnancy. risk, but the human experience is too use of antidiabetic agents, fonylureas glipizide (Glu- Saxagliptin (Onglyza) and sitagliptin limited to assess the risk, so they should other than insulin, that are cotrol), glimepiride (Amaryl), (Januvia), inhibitors of the enzyme be avoided in pregnancy. used for non–insulin-depen- and glyburide (DiaBeta, Gly- dipeptidyl peptidase–4, are indicated as In summary, only metformin and gly- dent diabetes during preg- nase, and Micronase) are pre- monotherapy or in combination with buride have sufficient human pregnancy nancy and lactation. -

Comparative Review of Oral Hypoglycemic Agents in Adults
SECTION 18.5 Comparative Review of Oral Hypoglycemic Agents in Adults Harinder Chahal For WHO Secretariat Table of Contents Acronyms: ............................................................................................................................................................................... 3 I. Background and Rationale for the review: ....................................................................................................................... 4 II. Medications under comparative review: ......................................................................................................................... 4 Table 1 - New oral hypoglycemic agents for comparison with current EML agents .......................................................... 5 III. Literature searches and methodology: ............................................................................................................................ 5 1. Title Search Results: .................................................................................................................................................... 6 2. Statement about quality of evidence: ........................................................................................................................ 6 IV. Clinical efficacy and safety evaluation: ............................................................................................................................ 6 1. DPP-4 Inhibitors (Sitagliptin, Saxagliptin) and Metformin: ........................................................................................ -

Oral Health Fact Sheet for Dental Professionals Adults with Type 2 Diabetes
Oral Health Fact Sheet for Dental Professionals Adults with Type 2 Diabetes Type 2 Diabetes ranges from predominantly insulin resistant with relative insulin deficiency to predominantly an insulin secretory defect with insulin resistance, American Diabetes Association, 2010. (ICD 9 code 250.0) Prevalence • 23.6 million Americans have diabetes – 7.8% of U.S. population. Of these, 5.7 million do not know they have the disease. • 1.6 million people ≥20 years of age are diagnosed with diabetes annually. • 90–95% of diabetic patients have Type 2 Diabetes. Manifestations Clinical of untreated diabetes • High blood glucose level • Excessive thirst • Frequent urination • Weight loss • Fatigue Oral • Increased risk of dental caries due to salivary hypofunction • Accelerated tooth eruption with increasing age • Gingivitis with high risk of periodontal disease (poor control increases risk) • Salivary gland dysfunction leading to xerostomia • Impaired or delayed wound healing • Taste dysfunction • Oral candidiasis • Higher incidence of lichen planus Other Potential Disorders/Concerns • Ketoacidosis, kidney failure, gastroparesis, diabetic neuropathy and retinopathy • Poor circulation, increased occurrence of infections, and coronary heart disease Management Medication The list of medications below are intended to serve only as a guide to facilitate the dental professional’s understanding of medications that can be used for Type 2 Diabetes. Medical protocols can vary for individuals with Type 2 Diabetes from few to multiple medications. ACTION TYPE BRAND NAME/GENERIC SIDE EFFECTS Enhance insulin Sulfonylureas Glipizide (Glucotrol) Angioedema secretion Glyburide (DiaBeta, Fluconazoles may increase the Glynase, Micronase) hypoglycemic effect of glipizide Glimepiride (Amaryl) and glyburide. Tolazamide (Tolinase, Corticosteroids may produce Diabinese, Orinase) hyperglycemia. Floxin and other fluoroquinolones may increase the hypoglycemic effect of sulfonylureas. -
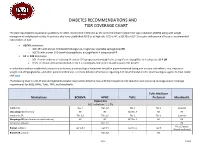
Diabetes Recommendations and Tier Coverage Chart
DIABETES RECOMMENDATIONS AND TIER COVERAGE CHART The American Diabetes Association guidelines for 2020, recommend metformin as the preferred initial treatment for type 2 diabetes (T2DM) along with weight management and physical activity. In patients who have established ASVD or at high risk, CKD, or HF, a SGLT2i or GLP-1 receptor with proven efficacy is recommended independent of A1C. • ASCVD dominates: o GLP-1RA with proven CVD benefit (dulaglutide, liraglutide, injectable semaglutide) OR o SGLT2i with proven CVD benefit (canagliflozin, empagliflozin) if adequate eGFR • HF or CKD dominates: o SGLT2i with evidence of reducing HF and/or CKD progression (empagliflozin, canagliflozin, dapagliflozin) if adequate eGFR OR o If SGLT2i intolerant/contraindicated or eGFR is inadequate, then GLP-1RA with proven CVD benefit In individuals without established cardiovascular disease, pharmacological treatment should be patient-centered taking into account side-effects, cost, impact on weight, risk of hypoglycemia, and other patient preferences. For more detailed information regarding ADA recommendations for pharmacological agents to treat T2DM click here. The following chart is a list of oral and injectable diabetes medications listed by class with their respective A1C reduction and insurance coverage and/or coverage requirements for BCBS, HPHC, Tufts, TMP, and MassHealth. Tufts Medicare Medications BCBSMA HPHC Tufts Preferred MassHealth Biguanides A1C reduction: 1-1.5% metformin Tier 1 Tier 1;2 Tier 1 Tier 1 Covered Glucoghage (metformin) NC NC NC;Tier -

The Synergistic Effect of Miglitol Plus Metformin Combination Therapy in the Treatment of Type 2 Diabetes
Clinical Care/Education/Nutrition ORIGINAL ARTICLE The Synergistic Effect of Miglitol Plus Metformin Combination Therapy in the Treatment of Type 2 Diabetes 1 JEAN-LOUIS CHIASSON, MD The recently developed class of 2 LISA NADITCH, MD ␣-glucosidase inhibitors has a unique FOR THE MIGLITOL CANADIAN UNIVERSITY mode of action; it blocks oligosaccharide INVESTIGATOR GROUP catabolism, delays carbohydrate diges- tion and absorption, and smooths and lowers postprandial plasma blood glu- cose peaks (6–9). Substantial evidence supports their use as monotherapy or ad- OBJECTIVE — To investigate the efficacy and safety of miglitol in combination with met- junct therapy for poorly controlled type 2 formin in improving glycemic control in outpatients in whom type 2 diabetes is insufficiently diabetes (5,10–14). Miglitol is the first controlled by diet alone. pseudomonosaccharide ␣-glucosidase in- RESEARCH DESIGN AND METHODS — In this multicenter, double-blind, placebo- hibitor derived from 1-deoxynojirimycin controlled study, 324 patients with type 2 diabetes were randomized, after an 8-week placebo and is structurally a glucose analog run-in period, to treatment with either placebo, miglitol alone, metformin alone, or miglitol plus (15,16). Its efficacy in monotherapy metformin for 36 weeks. The miglitol was titrated to 100 mg three times a day and metformin was (13,17) and in combination with sulfo- administered at 500 mg three times a day. The primary efficacy criterion was change in HbA1c nylureas (11) as a glucose-lowering agent from baseline to the end of treatment. Secondary parameters included changes in fasting and in type 2 diabetes has been shown in a postprandial plasma glucose and insulin levels, serum triglyceride levels, and responder rate. -

8. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2018
Diabetes Care Volume 41, Supplement 1, January 2018 S73 8. Pharmacologic Approaches to American Diabetes Association Glycemic Treatment: Standards of Medical Care in Diabetesd2018 Diabetes Care 2018;41(Suppl. 1):S73–S85 | https://doi.org/10.2337/dc18-S008 8. PHARMACOLOGIC APPROACHES TO GLYCEMIC TREATMENT The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” includes ADA’s current clinical practice recommendations and is intended to provide the components of diabetes care, general treatment goals and guidelines, and tools to evaluate quality of care. Members of the ADA Professional Practice Committee, a multidisciplinary expert committee, are responsible for updating the Standards of Care annually, or more frequently as warranted. For a detailed description of ADA standards, statements, and reports, as well as the evidence-grading system for ADA’s clinical practice recommendations, please refer to the Standards of Care Introduction. Readers who wish to comment on the Standards of Care are invited to do so at professional.diabetes.org/SOC. PHARMACOLOGIC THERAPY FOR TYPE 1 DIABETES Recommendations c Most people with type 1 diabetes should be treated with multiple daily in- jections of prandial insulin and basal insulin or continuous subcutaneous insulin infusion. A c Most individuals with type 1 diabetes should use rapid-acting insulin analogs to reduce hypoglycemia risk. A c Consider educating individuals with type 1 diabetes on matching prandial insulin doses to carbohydrate intake, premeal blood glucose levels, and anticipated physical activity. E c Individuals with type 1 diabetes who have been successfully using continuous subcutaneous insulin infusion should have continued access to this therapy after they turn 65 years of age. -

Medications Used to Treat Type 2 Diabetes
Medications Used to Treat Type 2 Diabetes This handout shows the different medications that your healthcare provider may prescribe to treat your type 2 diabetes, and where and how these medications work in your body to lower blood glucose. Type 2 diabetes medications are taken orally (by mouth), by injection (inserted into the fat under your skin), or inhaled (breathed in). Oral Injectable Alpha-glucosidase inhibitors (acarbose, miglitol) Amylin mimetic (pramlintide) Help to slow down the breakdown of starches (such Helps to decrease the amount of glucose made by your liver. as bread and potatoes) and certain types of sugar (such as table sugar) from your food in your intestines: Helps to slow down the breakdown of foods in your stomach this slows down increases in blood glucose. and intestines: this slows down increases in blood glucose Biguanide (metformin) GLP-1 receptor agonists (albiglutide, dulaglutide, exenatide, liraglutide) Helps to decrease the amount of glucose made by your liver Help your pancreas to make more insulin: insulin helps to lower blood glucose Helps to improve the way that insulin works in your Help to decrease the amount of glucose made by your muscles: if your muscles are more sensitive to insulin, it liver is easier for insulin to bring glucose from your blood into Helps to slow down the breakdown of foods in your muscles where glucose can be used for energy your stomach and intestines: this slows down increases in blood glucose DPP-4 inhibitors (alogliptin, linagliptin, saxagliptin, sitagliptin) Fat Tissue -

Glycemic Management of Type 2 Diabetes
Glycemic Management of Type 2 Diabetes Gail Nunlee-Bland, M.D. Professor Medicine & Pediatrics Director, Diabetes Treatment Center Howard University 1 Disclosures • None Learning Objectives • Understand the importance of lifestyle therapy in diabetes management • Know the classes of antihyperglycemic agents, mechanism of action, benefits and side effects of these agents • Recognize the importance of individualized treatment goals for diabetic patients AACE Comprehensive Care Plan Disease management from Antihyperglycemic a multidisciplinary team pharmacotherapy Comprehensive Care Plan Comprehensive diabetes Therapeutic lifestyle self-education for the change patient 4 Handelsman YH, et al. Endocr Pract. 2015;21(suppl 1):1-87. Glycemic Management of Type 2 Diabetes THERAPEUTIC LIFESTYLE CHANGE 5 Components of Therapeutic Lifestyle Change • Healthful eating • Sufficient physical activity • Sufficient sleep • Avoidance of tobacco products • Limited alcohol consumption • Stress reduction 6 Handelsman YH, et al. Endocr Pract. 2015;21(suppl 1):1-87. Glycemic Management of Type 2 Diabetes ANTIHYPERGLYCEMIC THERAPY 7 Cardiovascular Outcomes Trials: A Brief History • 2008 FDA guidance mandating assessment of CV safety of all antihyperglycemic agents in RCTs – Designed as noninferiority studies to demonstrate study drug was not associated with more MACE than placebo • Some study designs tested for superiority if noninferiority criteria were met – Primary endpoint: composite of cardiovascular death, nonfatal MI, and nonfatal stroke • Some primary -

Standards of Medical Care in Diabetes—2019
S90 Diabetes Care Volume 42, Supplement 1, January 2019 9. Pharmacologic Approaches to American Diabetes Association Glycemic Treatment: Standards of Medical Care in Diabetesd2019 Diabetes Care 2019;42(Suppl. 1):S90–S102 | https://doi.org/10.2337/dc19-S009 The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” includes ADA’s current clinical practice recommendations and is intended to provide the components of diabetes care, general treatment goals and guidelines, and tools to evaluate quality of care. Members of the ADA Professional Practice Committee, a multidisciplinary expert committee, are responsible for updating the Standards of Care annually, or more frequently as warranted. For a detailed description of ADA standards, statements, and reports, as well as the evidence-grading system for ADA’s clinical practice recommendations, please refer to the Standards of Care Introduction. Readers who wish to comment on the Standards of Care are invited to do so at professional.diabetes.org/SOC. PHARMACOLOGIC THERAPY FOR TYPE 1 DIABETES Recommendations 9.1 Most people with type 1 diabetes should be treated with multiple daily 9. PHARMACOLOGIC APPROACHES TO GLYCEMIC TREATMENT injections of prandial and basal insulin, or continuous subcutaneous insulin infusion. A 9.2 Most individuals with type 1 diabetes should use rapid-acting insulin analogs to reduce hypoglycemia risk. A 9.3 Consider educating individuals with type 1 diabetes on matching prandial insulin doses to carbohydrate intake, premeal blood glucose levels, and anticipated physical activity. E 9.4 Individuals with type 1 diabetes who have been successfully using continuous subcutaneous insulin infusion should have continued access to this therapy after they turn 65 years of age.