Shipyard Welder Ignites Hydraulic Fluid and Is Fatally Burned
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Welding, Cutting and Brazing Safety Guidelines
Welding, Cutting and Brazing Safety Guidelines April 2020 Welding, Cutting and Brazing Safety Guidelines Table of Contents I. Purpose II. Responsibilities III. Hazard Identification & Prevention IV. Protection of Personnel V. Health Protection/ Ventilation Requirements VI. Operational Safety VII. Training & Record Keeping Appendix A Filter Shade Selection Guide by Welding Type Welding, Cutting and Brazing Safety Guidelines I. Purpose The purpose of the University of Northern Colorado’s Welding, Cutting and Brazing (WC&B) program is to protect faculty, staff, students and visitors from hazards associated with activities that requires the use of equipment involving open flames, sparks and heat that pose fire and other health hazards. This program establishes minimum requirements for performing work during such activities in a safe and cautious manner. II. Responsibilities The appropriate department shall be responsible for following in accordance with this guideline. A. Environment, Health & Safety (EHS) Department shall: • Review and approve, in coordination with the AVP Facilities Management the designated areas approved for welding and cutting activities. • Maintain a list of designated areas. • Inspect designated areas to be sure that conditions have not become unsafe for welding and/or cutting annually. • Provide training for fire watches. • Suspend welding and cutting work if conditions become unsafe for the work being performed. • Investigate any incidents that may occur during operations. B. Supervisors shall: • Ensure employees who will be performing such operations are properly trained on this procedure before performing work on campus. • Ensure the safe operation of equipment, incorporating information from Material Safety Data Sheets (MSDS) on welding materials used, appropriate Personal Protective Equipment (PPE), evaluation of combustible materials and hazardous areas present or likely to be present in the work location. -

Welder Type: Full Time, Monday-Thursday 7:00A - 4:30P, Friday 7:00A – 11:00A Department: Metal Fabrication Reports To: Metal Fabrication Department Manager
Job Title: Welder Type: Full Time, Monday-Thursday 7:00a - 4:30p, Friday 7:00a – 11:00a Department: Metal Fabrication Reports To: Metal Fabrication Department Manager ABOUT SHUR-CO®: Shur-Co®, LLC, is headquartered in Yankton, South Dakota, and is a leading provider of covering systems, parts and service to the global transportation market. With over 60 years of industry experience, Shur-Co® now manufactures a wide offering of tarp systems and accessories for trucks, trailers, carts and specialty equipment used in the agriculture, construction, waste and flatbed markets. Shur-Co® operates 12 production sites and sales locations in the United States, Canada and the United Kingdom, giving you the opportunity to work with employees and customers all over the world. We are always looking for well-qualified candidates to fill a variety of open positions. Check out all of our opportunities at www.Shur-Co.com/employment. SUMMARY: Lay out, fit, and weld fabricated steel and aluminum components, by performing the following duties. Must be able to efficiently weld small and large gauge metal with high quality. ESSENTIAL DUTIES AND RESPONSIBILITIES: • Select equipment and plan layout, assembly and welding. • Require minimal guidance from Lead in welding area. • Direct setup personnel in layout, and align the fitting of components together. • Set up equipment and weld parts using arc, gas-shielded arc, or gas welding equipment. • Responsible for welding tasks as assigned by Lead and/or Department Manager. • Responsible for the equipment care and proper machine settings to optimize the welding equipment. • Report to the Area Lead any nonconformance of components and/or machine function characteristics. -

Welding on the Farm: Selecting a Welding Unit for the Farm Or Ranch
Welding on the Farm: Selecting a Welding Unit for the Farm or Ranch Farms encounter a wide variety of welding repairs and projects – having the right welder depends on a lot of factors. Do you have to bring the welder to the work or can you take the work to the welder? Which process (MIG, Stick, or TIG) fits your needs? This article examines all these issues and more. The weather finally cleared, and Wisconsin dairy farmer Al Hoffmann has 385 acres of haylage to cut and store when the chopper blower band for the silo snaps in half. Part of the 3/16 in. steel band has worn paper thin and snapped, and on this Saturday, the nearest replacement band is two days away. Using a 200 amp Millermatic® wire welder, Al saves the band by tack welding it together and then welding on a back-up strip of steel. The repaired chopper blower moves more than 800 tons of haylage in the next few days... ...It's evening milking time. Al is half done with his 185 cows when a hinge breaks on the air gate in the milking parlor. Al resumes milking a few minutes later, after he repairs the gate with a portable Millermatic wire welder that runs off his 115 V household current. "This farm has a lot of old iron, but welders keep my machinery running," Al says. In addition to the two wire welders, Al also uses a 175 amp Stick (shielded metal arc) welder, primarily for hardfacing the bucket on his skid loader or repairing his manure spreader. -

Job Opening: Tig Welder Millwright
Job Opening: Tig Welder Millwright Position Overview The role of Journeyman Tig Welder Millwright is to compliment our current team of technicians and assist Knack’s food and beverage customer base with advanced welding, fabrication, and industrial support, to maintain and improve their processing operations. The scope ranges anywhere from day to day maintenance or welding repairs, up to the plant project scale. This takes place on the customer job site or at our shop. Required Personal Responsibilities: • Display Initiative and ability to work self-sufficiently with minimal supervision. Journeyman level experience. • Ability to be resourceful and independently creative to get the job done under pressure or tight timelines. • Work within a team environment and maintain a positive attitude. • Professional, informative, and responsive communication to the manager, staff and customers. • Interacts with customers to understand their requests or concerns. • Interacts with customers to provide feedback on job completion or the necessary performance of tasks. • Must be able to respond to plant emergencies as directed outside of normal working hours. • Operation, maintenance and repair of responsible tools and equipment. • High level of integrity. Required Technical Skills: • Understand, install, troubleshoot and maintain various types of food processing equipment including but not limited to: pumps, conveyors, agitators, tanks, exchangers, valving, etc. • Advanced Journeyman level sanitary stainless steel tig welding experience. • Journeyman ability to design, fabricate and build basic and/or complex structures, supports or framework. • Ability to perform oxy fuel and plasma cutting processes. • Perform safe rigging procedures for lifting or installing various equipment. • Perform demolition of equipment/systems and the ability to properly isolate, rig and remove safely and in proper sequence. -

Welder / Mechanic Job Code: 2340 Department: General Services Date: 2/08 Reports To: Shop Supervisor
Welder/Mechanic Page 1 of 2 CITY OF CONCORD CLASS SPECIFICATION CLASS TITLE: WELDER / MECHANIC JOB CODE: 2340 DEPARTMENT: GENERAL SERVICES DATE: 2/08 REPORTS TO: SHOP SUPERVISOR JOB SUMMARY: Performs skilled acetylene and electric arc welding work in the fabrication, repair, and reinforcement of metal parts and equipment. Also performs extensive heavy-duty mechanical repairs. ESSENTIAL JOB FUNCTIONS: Performs cutting and welding operations on machinery and equipment; repairs parts for machinery and equipment. Determines appropriate welding techniques and equipment to use; works from sketches, blueprints, and instructions given both orally and in writing. Performs designing, layout and fabrication of various metal items used by the city. Performs on location welding operations on city structures and equipment. Operates air arc machine to cut heavy material. Fabricates metal articles such as brackets, pipe hangers, braces, sanders, rakes, teeth, and plow blades. Maintains and makes repairs on welding equipment; sharpens and tempers tools. Mounts bodies on new cabs and chassis. Welds and repairs tractor trucks and trailers. Performs general repair and maintenance of city vehicles. Performs inspections of city vehicles. Responds to call for roadside assistance. Operates hydraulic hose equipment. Diagnoses and repairs hydraulic and electrical equipment. Performs other related duties as assigned. MATERIAL AND EQUIPMENT USED: Wirer Feed-Mik Welder Cutting Torches Placemat Cutter Mechanical Hand Tools Gas Welder Arc Welder MINIMUM QUALIFICATIONS REQUIRED: Education and Experience: High School diploma or GED; and, additional training in welding apprenticeship; and, four years of experience as journeyman welder; or, any combination of education, training and experience, which provides the knowledge, skills, and abilities required for the job. -
Physical Demands Analysis Welder Prepared
Physical Demands Analysis 154 Meadowlark Health Centre 156 Street & 87 Avenue Welder Edmonton, Alberta T5R 5W9 Tel (780) 429-4761 Fax (780) 425-4274 Prepared for: Toll Free 1-800-493-5446 Alberta Construction Association Job Title: Welder Assessment Edmonton, AB Data Collection August 18, 2020 Location: Date: Completed By: Erika Job BSc.OT Submitted on: November 11, 2020 Disclaimer: The Physical Demands noted in this report may vary depending on company and location. Please contact the company directly to confirm this physical demands analysis is an accurate representation of the specific job title for the specific location. Work Shift Duration: 5 days/week, 8 hours/day; may vary depending on volume Schedule: Break Schedule: Total of 1 hour break per day / 2-15 minute coffee breaks, 1-30 minute lunch break Shift Rotation: Not applicable On call is required: No Overtime required: No; but available (longer days/Saturday) Education / Education required: A Journeyman Welder participates in a 3 year program including 8 weeks of Experience: in school training and 1500 hours of on the job training per year. Hours required for position: A minimum of 4500 hours of on the job training is requires to be a Journeyman Welder. Tickets that may be required (not limited to): Basic Safety Orientation provided on site. Other onsite training including WHIMIS, machinery use. Labour N/A Provider: Job The Journeyman Welder is responsible for performing welding which includes repairs on various Overview: The heavy equipment such as loaders, excavators, crushers, trailers, dump trucks, dump roll of bins etc. They are also responsible for fabricating and welding components such as supports and structures throughout the shop and for various equipment. -

Ironworkers Local 97 Standard Agreement
IRONWORKERS LOCAL 97 STANDARD AGREEMENT Between: Local 97 of the International Association of Bridge, Structural, Ornamental and Reinforcing lronworkers (Hereinafter Referred to as the "Union") And: Construction Labour Relations Association of B.C. {CLR) * (On its own behalf, and on behalf of its member Employers who have authorized the Association to execute this document and those members added from time to time by notice given to the BCBCBTU. (hereinafter referred to as "CLR") May 1, 2016 to April 30, 2019 lronworkers Local 97 Standard Agreement May 1, 2016 to April 30, 2019 Drug & Alcohol Abuse Statement of Policy •Where a pattern of chemical dependence is suspected or apparent and documented; •And where the problem is affecting the Member's ability to do his assigned job; • And where it may affect the safety of that or other tradesmen on that job; The Union office will address the situation with that Member. The discussion will be CONFIDENTIAL, NON-THREATENING AND SUPPORTIVE. The Member in question will, at the initial discussion, be made aware of the Union's concern and a suggestion made that he or she seek help for the problem through the Rehabilitation Plan or any other resources at his disposal. The Member then has his choices. At this point, a time frame to effect a change in the pattern will be contracted with the Member. Given a fair time allowance with no significant change in behaviour or a worsening of the situation, the Mandatory Referral process will take place. The Member will be re-confronted and informed that unless treatment is sought, dispatch privileges (may) will be revoked until there is evidence that the addiction had been dealt with in a recognized treatment process or facility. -

Impacts of Welding on Environmental Problems and Health and Solutions to Overcome These Problems
IMPACTS OF WELDING ON ENVIRONMENTAL PROBLEMS AND HEALTH AND SOLUTIONS TO OVERCOME THESE PROBLEMS 1MOSTAFA HASHEMI FARD, 2MOHSEN HASHEMI FARD B.Eng, Welding Technology, Applied Science and Technology University Unit Alavicheh, Isfahan Experimental expert, Welding Technology Abstract— According to scientific progress and industrialization, engineering sciences and processes have significant progress in all the areas. There are important problems because of this progress in addition to the advantages such as life simplicity, life quality improvement and many other advantages. Environmental problems are one of the main problems due to the rapid development of engineering technologies. Therefore, nowadays environment should enter on different the field of engineering, and it should control, guide and develop these processes according to the specific principles and effects of these processes on environment and health. According to the nature and used equipment, welding is a job with the major impact on environment and human health. Released fume in welding, is a combination of various and fine particles such as carbon monoxide, silicates and so on. Welding fume analysis showed this fume is rich in toxic and hazardous compounds. On the other hand, medical investigations proved, welders are in serious danger of acute and chronic respiratory diseases. The problems are not limited to the respiratory diseases only. In this regard, it can be noted some problems such as suffocation, skin diseases, visual disturbances, many long-term negative effects and environmental problems due to the welding fume. It is very painful that many welders don’t know anything about these problems, and the suffered from irrecoverable effects because this lack of awareness. -
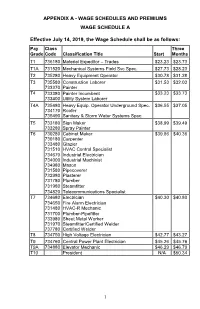
1 Appendix A
APPENDIX A - WAGE SCHEDULES AND PREMIUMS WAGE SCHEDULE A Effective July 14, 2019, the Wage Schedule shall be as follows: Pay Class Three Grade Code Classification Title Start Months T1 736180 Materiel Expeditor – Trades $23.23 $23.73 T1A 731520 Mechanical Systems Field Svc Spec. $27.73 $28.23 T2 735280 Heavy Equipment Operator $30.78 $31.28 T3 735580 Construction Laborer $31.53 $32.03 733370 Painter T4 733380 Painter Incumbent $33.23 $33.73 733400 Utility System Laborer T4A 735480 Heavy Equip. Operator Underground Spec. $36.55 $37.05 734170 Roofer 735490 Sanitary & Storm Water Systems Spec. T5 733180 Sign Maker $38.99 $39.49 733280 Spray Painter T6 730280 Cabinet Maker $39.86 $40.36 730180 Carpenter 733480 Glazier 731510 HVAC Control Specialist 734670 Industrial Electrician 734000 Industrial Machinist 734980 Mason 731580 Pipecoverer 732980 Plasterer 731780 Plumber 731980 Steamfitter 734820 Telecommunications Specialist T7 734680 Electrician $40.30 $40.80 734650 Fire Alarm Electrician 731480 HVAC-R Mechanic 731700 Plumber-Pipefitter 733980 Sheet Metal Worker 731970 Steamfitter/Certified Welder 737780 Certified Welder T8 734750 High Voltage Electrician $42.77 $43.27 T9 734760 Central Power Plant Electrician $45.26 $45.76 T9A 734880 Elevator Mechanic $46.29 $46.79 T10 President N/A $50.34 1 WAGE SCHEDULE B Effective July 12, 2020, the Wage Schedule shall be as follows: Pay Class Three Grade Code Classification Title Start Months T1 736180 Materiel Expeditor – Trades $23.94 $24.44 T1A 731520 Mechanical Systems Field Svc Spec. $28.58 $29.08 T2 735280 Heavy Equipment Operator $31.72 $32.22 T3 735580 Construction Laborer $32.49 $32.99 733370 Painter T4 733380 Painter Incumbent $34.24 $34.74 733400 Utility System Laborer T4A 735480 Heavy Equip. -

Welding Technology (WELD) 1
Welding Technology (WELD) 1 WELD 0004. Welding Operator Orientation WELDING TECHNOLOGY Units: 0.5 Prerequisite: Completion of WELD 2A and 5A with grades of "C" or better (WELD) Hours: 9 lecture Orientation course to prepare students for enrollment in WELD 84 (pass/ WELD 0001A. Introductory Welding for Metalworking no pass grading) (not transferable) Units: 2 WELD 0005A. Introduction to Shielded Metal Arc Welding (SMAW) - Formerly known as WELD 15 Career Path Hours: 72 (18 lecture, 54 laboratory) Units: 2 Hands-on survey class that focuses on the three common welding Formerly known as WELD 20 processes of Shielded Metal Arc Welding, Gas Metal Arc Welding, Advisory: Concurrent enrollment in WELD 1A or previous welding and Gas Tungsten Arc Welding, including correct setup and "how to" experience techniques. Plasma Arc Cutting and Oxyacetylene Cutting processes Hours: 72 (18 lecture, 54 laboratory) are also covered. This class is a survey of basic welding, cutting and An introduction to the principles of shielded metal arc welding (SMAW), fabrication used by the welding industry, metalworking artists, and setup/use of SMAW equipment, and safe use of tools and equipment interested hobbyists. Perfect for students who have never welded before. including oxyacetylene cutting. Provides instruction in welding carbon (CSU) steel weld joints in various positions. This is a required foundation WELD 0001B. Principles of Fabrication welding technology course for students who wish to pursue a career in Units: 2 structural or pipe welding outdoors at various construction sites. (C-ID Formerly known as WELD 70 WELD 101X) (not transferable) Prerequisite: Completion of WELD 1A and completion of WELD 2A, WELD WELD 0005B. -

Wire Feeder Welder
WIRE FEEDER IMT891-D WELDER (125, 140, 180 MODELS) June, 2011 For use with machines having Code Numbers: 11173 thru 11506, 11550, 11658 TABLE OF CONTENTS Installation . .Section A Technical Specifications . .A-1, A-2 Safety Precautions . .A-2 Location . .A-2 Stacking . .A-2 Tilting . .A-2 Identify and Locate Components for 180 Amp and 140 Amp Units . .A-3 Identify and Locate Components for 125 Amp Flux Core Unit . .A-3 OPERATORʼS MANUAL Operation . .Section B Safety and Product Description . .B-1 Controls and Settings . .B-2, B-3 Drive Roll and Wire Guides Table . .B-4 Setting Up and Making a Flux-Cored Weld B-4 thru B- ISO 9001 ANSI RAB 6 QMS Setting Up and Making a MIG Weld and Designed and Manufactured Under a Quality Program Certified by ABS Quality Evaluations, Inc. Install Shielding Gas . .B-7 thru B-10 to ISO 9001 Requirements. CERTIFICATE NUMBER: 30273 Setting Up and Making a Aluminum Weld . .B-11 Accessories . .Section C Optional Accessories . .C-1 Utility Carts . .C-2, C-3 Safety Depends on You Maintenance . .Section D Lincoln arc welding and cutting Safety Precautions . .D-1 equipment is designed and built MANUAL DE OPERACIÓN MANUAL Wire Feed Compartment, Fan Motor, Wire Reel with safety in mind. However, Maintenance . .D-1 your overall safety can be Gun And Cable Maintenance . .D-2 increased by proper installation Overload Protection . .D-2 ... and thoughtful operation on your part. DO NOT INSTALL, Component Replacement Procedures . .D-2 OPERATE OR REPAIR THIS EQUIPMENT WITHOUT READ- Troubleshooting . .Section E ING THIS MANUAL AND THE Safety Precautions . -

Modesto City Schools Job Description
MODESTO CITY SCHOOLS JOB DESCRIPTION LEAD CARPENTER/WELDER DEFINITION: Under the direction of the Supervisor-Maintenance and Operations, lead and participate in a variety of skilled carpentry, welding and metal fabrication activities in the maintenance, repair, construction, alteration, forming, framing and finishing of buildings, furniture and facilities; construct, install, maintain and repair woodwork; develop and implement carpentry and welding projects; train and provide work direction and guidance to assigned personnel. ESSENTIAL DUTIES AND RESPONSIBILITIES: Perform skilled carpentry work in the maintenance, repair, construction, alteration, forming, framing and finishing of buildings, furniture and facilities; receive and respond to work orders; assure compliance with building, health and safety laws, codes, regulations and standards. Develop and implement carpentry construction, maintenance, repair and enhancement projects; estimate labor, material and equipment requirements for projects; monitor, assess and modify activities in response to project progress. Lead and participate in a variety of skilled welding and metal fabrication activities in the repair, alteration, fabrication, installation and maintenance of various types of metal, parts and equipment utilizing oxyacetylene and electric arc welding, soldering and brazing processes; assure compliance with building and safety laws, codes, regulations and standards applicable to the welding trade. Oversee and participate in the brazing, hard facing, cutting, soldering and