July 1– September 30, 2016 Project Year 3, Quarter 4 Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bangladesh Needs Assessment Working Group (NAWG) Report on Landslides
Bangladesh Needs Assessment Working Group (NAWG) Report on Landslides Landslides, Bangladesh, June 2017 Report date: 19 June 2017 (Source: UNICEF) Md. Yousuf Ali, Director-MIM, DDM, Email: [email protected] Contact for Inquiries: Arshad Muhammad, Assistant Country Director – Programs , CARE, Email: [email protected] Landslides, Bangladesh June 2017 Contents Contents 2 Background 3 Key Findings 4 Context of the Affected Area 6 Key characteristics of the affected districts by the landslides 8 Situation Overview 10 Detailed Findings 15 Access and Infrastructure 15 Communication 16 Child Protection 18 Education 19 Food Security 20 Livelihoods and Income 20 Gender Based Violence 21 Gender 23 Health 23 Market 25 Nutrition 26 Shelter 27 Water, Sanitation and Hygiene (WASH) 28 Annex A: Affected people per Upazila 30 2 Landslides, Bangladesh June 2017 Background On June 13th the districts of Bandarban, Chittagong, Rangamati, Khagrachari and Cox’s Bazaar suffered from possibly the deadliest landslides in their history. The disaster killed an estimated 160 persons, including 115 persons in Rangamati alone. According to the Chittagong Divisional Health Office Control Room Report, a total of 187 injured persons were admitted in local level hospitals. Approximately 85% of patients were admitted in Rangamati. While landslide related disaster occurs nearly every year, the second highest death toll of 127 deceased persons was recorded in 2007 [Disaster Forum, June 2017]. Monsoon rains caused severe flooding in low-lying areas to significantly damage road and communication infrastructure. Flood water rendered remote communities in Bandarban, Chittagong, and Rangamati districts were inaccessible by road. On June 14th, mudslides in southeast Bangladesh claimed additional lives in Cox's Bazaar and Khagrachari districts to further damage homes and infrastructure. -

Climate Change Adaptation Project Preparation in LGED Context And
Climate Change and Bangladesh: Optimization of Projects for LGED Monzur Sadeque Executive Engineer (Planning), LGED 1 Scope of the Presentation • LGED & Climate Change Adaptation Projects • Unutilized & Underutilized Potentials • Scopes of Different Sectors • LGED’s Responsibilities • Near Future Projects 2 Himalaya Bay of Bangle A Sand witch Country between the Mountain and the Sea 3 Background • The country is lying in front of natural disasters ; flood and cyclone storms • Climate change impacts increasing natural disasters with other impacts like sea level rise, salinity intrusion, draught, extreme weather, erosion, drainage congestion etc. 4 Background • The country is vulnerable to climate change due to climatic, physiographic and socio economic factors like population, low income, poor resource management etc. • Needs solution of present problems as well as future anticipated problems….. 5 What are the Risks ? 6 Mainstreaming the Risks • In 1990s- WOMEN IN DEV. (WID) • In 2000s- Environment & Sustainable Development • In 2010s- Climate Mainstreaming 7 Climate Change Projects-LGED Name of Financed Area the Project and By Estimated Cost (Crore Tk) CDTA/ PPTA/PDA for ADB Amtoli, Coastal Towns (Climate Galachipa,Pirozep Infrastructure Improvement Investment ur, Mathbaria, Project (3 projects) Fund) Daulatkhan, 48.52 Bhola, Kalapara, Barguna Coastal Towns ADB -Same- Infrastructure Improvement (CIF) Project 876.00 8 Climate Change Projects-LGED Name of Financed Area the Project and By Estimated Cost (Crore Tk) CDTA/ PPTA/PDA for ADB Amtoli, Coastal Towns (Climate Galachipa,Pirozep Infrastructure Improvement Investment ur, Mathbaria, Project (3 projects) Fund) Daulatkhan, 48.52 Bhola, Kalapara, Barguna Coastal Towns ADB -Same- Infrastructure Improvement (CIF) Project 876.00 9 Climate Change Projects-LGED Name of Financed Area the Project & Estimated By Cost (Crore Tk. -

Project Plan 3-5 Years
PROJECT DESIGN FORM1 Project title: Enhancing CBID in Bangladesh Region: SAR Country: Bangladesh Partner Name Centre for Disability in Development (CDD) Project start 1 January 2020 – 31 December 2022 /end date: Project Number Applied (if available): 1 This Form is to be used for planning of all projects with a total budget of >50,000 EUR. The term “Project” within the document always also refers to Programmes. For projects with an overall project budget of <50,000 EUR, the following documents are to be submitted: i) Project Idea and Programmatic Approval Form (PPA) Section I. A-C + Section II.; ii) Logical Framework and Cost plan CBM International - Project Design Form Version 1.0 (approved June 2018) 1 Contents I. Project Abstract 3 II. Full Project Design 8 1. Relevance of the Project 8 2. Effectiveness and quality 12 3. Efficiency 20 4. Sustainability and Contribution to Change 23 III. Annexes A. Description of Project context 26 B. Logical framework / cost plan 36 C. Activity schedule 36 D. Risk Register 36 E. Monitoring and Evaluation (M&E) Plan 36 F. Quality criteria for Project Design 37 CBM International - Project Design Form Version 1.0 (approved June 2018) 2 I. Project Abstract A) Project Information Name of Partner Centre for Disability in Development Region: SAR Country: Bangladesh Project title Enhancing CBID in Bangladesh Project Location Chittagong City Corporation Ward No. 13, 14 & 15 and Bashkhali and Rangunia Sub-Districts of Chittagong District. Timeframe 1st January 2020-31st December 2022 Target group Direct Beneficiaries of the project are at least 2,000 persons with disabilities. -

Final Draft SRCWP Project
Government of Bangladesh Ministry of Environment and Forests Bangladesh Forest Department Dudpukuria-Dhopachari Wildlife SanctuaryDraft ManagementProject plan Final 2015 - 2025 SRCWP FINAL VERSION Dudpukuria-Dhopachari Wildlife Sanctuary Management Plan 2015 - 2025 Final Version, 15 December 2014 15 December 2014 This management plan has been prepared under the CLIMATE-RESILIENT ECOSYSTEMS AND STRENGTHENING REGIONAL COOPERATION LIVELIHOODS (CREL) PROJECT FOR WILDLIFE PROTECTION PROJECT (SRCWP) DraftProject Funded by USAIDFinal Funded by the World Bank SRCWP Implemented by Implemented by Winrock International (US) Agriconsulting S.p. A. (ITA) - Agrer S.A. (BE) - SODEV Consult (BD) 2 Dudpukuria-Dhopachari Wildlife Sanctuary Management Plan 2015 - 2025 Final Version, 15 December 2014 Office of the Chief Conservator of Forests Forest Department, Banabhaban, Agargaon, Dhaka-1207, Bangladesh Phone:+88-02-8181737, Fax: +88-02-8181741 Office of the Divisional Forest Officer Chittagong South Forest Division Ban Pahar, Nandankanan, Chittagong Dudpukuria Beat, Khurushia Range Chittagong South Forest Division Dudpukuria Post Office: Padua, Rangunia Upazila, Chittagong District Draft Dhopachari Beat, Dohazari Range Project Chittagong South Forest Division West Dhopachari, Camp para,Final Post Office: Dhopachari, Chandanish Upazila, Chittagong District SRCWP 3 Dudpukuria-Dhopachari Wildlife Sanctuary Management Plan 2015 - 2025 Final Version, 15 December 2014 Acknowledgements 1. This management plan is the result of a joint effort of the Bangladesh Forest Department and other stakeholders and partners. 2. Special thanks go to Bangladesh Forest Department, Md. Yunus Ali, CCF (overall guidance), Mr. Ratan Kumar Majumder, DCCF, (focal point), Mr. Tariqul Islam, ACCF, (focal point) Mr. Dewan Jafrul Hasan, CF, Chittagong Circle, (field co-operation) and Bipul Krishna, DFO, Chittagong South Forest Division (field co-operation). -

(RTIP-II), Region-2 PHASE II UZR SUBPROJECTS
Local Government Engineering Department (LGED) Public Disclosure Authorized Second Rural Transport Improvement Project (RTIP-II), Region-2 Public Disclosure Authorized PHASE II UZR SUBPROJECTS WITHOUT ACQUISITION OF PRIVATE LANDS 2014 – 2015 Public Disclosure Authorized SOCIAL IMPACT MANAGEMENT PLAN (SIMP) Public Disclosure Authorized January 2015 Social Impact Management Plan Social Impact Management Plan (SIMP) Region 2, Second Year UZR Subprojects without Acquisition of Private Land Table of Contents 1. INTRODUCTION ........................................................................................................... 1 1.1. Project Background .................................................................................................. 1 1.2. Region 2 Project area ............................................................................................... 1 1.3. Second Year Subprojects in Region 2 ...................................................................... 2 1.4. Social Implication of UZR Subprojects without Land Acquisition ......................... 2 1.5. Measures to Minimize Impacts ................................................................................ 4 1.6. Social Impact Management Plan (SIMP) ................................................................. 4 1.7. Approval and Disclosure .......................................................................................... 4 2. SOCIOECONOMIC INFORMATION ........................................................................... 5 2.1. Project -

Community Health Program at Remote Hill District, Bangladesh 1
Nadira Sultana ACCESS Health International May 2011 Community Health Program at Remote Hill District, Bangladesh 1 Community Health Program at Remote Hill District, Bangladesh Nadira Sultana ACCESS Health International Bangladesh May 2011 2 Table of Contents Acknowledgements ........................................................................................................................4 Disclaimer.......................................................................................................................................4 Copyright ........................................................................................................................................4 Executive Summary ........................................................................................................................5 Introduction....................................................................................................................................7 Background of Chittagong Hill Tract...............................................................................................7 Christian Hospital Chandraghona (CHC).........................................................................................9 Community Health Program (CHP)...............................................................................................10 Mobile Clinics (MCs).....................................................................................................................16 Hospital Referral...........................................................................................................................18 -

List of Upazilas of Bangladesh
List Of Upazilas of Bangladesh : Division District Upazila Rajshahi Division Joypurhat District Akkelpur Upazila Rajshahi Division Joypurhat District Joypurhat Sadar Upazila Rajshahi Division Joypurhat District Kalai Upazila Rajshahi Division Joypurhat District Khetlal Upazila Rajshahi Division Joypurhat District Panchbibi Upazila Rajshahi Division Bogra District Adamdighi Upazila Rajshahi Division Bogra District Bogra Sadar Upazila Rajshahi Division Bogra District Dhunat Upazila Rajshahi Division Bogra District Dhupchanchia Upazila Rajshahi Division Bogra District Gabtali Upazila Rajshahi Division Bogra District Kahaloo Upazila Rajshahi Division Bogra District Nandigram Upazila Rajshahi Division Bogra District Sariakandi Upazila Rajshahi Division Bogra District Shajahanpur Upazila Rajshahi Division Bogra District Sherpur Upazila Rajshahi Division Bogra District Shibganj Upazila Rajshahi Division Bogra District Sonatola Upazila Rajshahi Division Naogaon District Atrai Upazila Rajshahi Division Naogaon District Badalgachhi Upazila Rajshahi Division Naogaon District Manda Upazila Rajshahi Division Naogaon District Dhamoirhat Upazila Rajshahi Division Naogaon District Mohadevpur Upazila Rajshahi Division Naogaon District Naogaon Sadar Upazila Rajshahi Division Naogaon District Niamatpur Upazila Rajshahi Division Naogaon District Patnitala Upazila Rajshahi Division Naogaon District Porsha Upazila Rajshahi Division Naogaon District Raninagar Upazila Rajshahi Division Naogaon District Sapahar Upazila Rajshahi Division Natore District Bagatipara -

A Study on Residential Shift of the Remittance Receiving Households
MURP THESIS A STUDY ON RESIDENTIAL SHIFT OF THE REMITTANCE RECEIVING HOUSEHOLDS KAUSIK DAS KAUSIK DAS DEPARTMENT OF URBAN AND REGIONAL PLANNING BANGLADESH UNIVERSITY OF ENGINEERING AND TECHNOLOGY DHAKA, BANGLADESH MAY 2010 MAY 2010 A STUDY ON RESIDENTIAL SHIFT OF THE REMITTANCE RECEIVING HOUSEHOLDS By KAUSIK DAS MASTER OF URBAN AND REGIONAL PLANNING DEPARTMENT OF URBAN AND REGIONAL PLANNING BANGLADESH UNIVERSITY OF ENGINEERING AND TECHNOLOGY DHAKA, BANGLADESH MAY 2010 The thesis titled, “A STUDY ON RESIDENTIAL SHIFT OF THE REMITTANCE RECEIVING HOUSEHOLDS” submitted by Kausik Das, Roll No: 100615032(F),Session: October 2006, has been accepted as satisfactory in partial fulfillment of the requirements for the degree of MASTER OF URBAN AND REGIONAL PLANNING (MURP) on 4 May, 2010 BOARD OF EXAMINERS Md. Musleh Uddin Hasan Assistant Professor Department of Urban and Regional Planning, BUET Chairman &Supervisor Dr. Sarwar Jahan Professor and Head Department of Urban and Regional Planning, BUET Member(Ex-Officio) Dr. Shakil Akther Associate Professor Department of Urban and Regional Planning, BUET Member Dr. Chowdhury Rafiqul Abrar Professor Department of International Relations, Member (External) Dhaka University Director RMMRU, Dhaka CANDIDATE’S DECLARATION It is hereby declared that this thesis or any part of it has not been submitted elsewhere for the award of any degree or diploma. Kausik Das Student No. 100615032 URP, BUET, Dhaka Dedicated to My parents TABLE OF CONTENT Page No. List of Tables iv List of Figures v List of Maps v Abbreviation -
Chittagong C09.Pdf
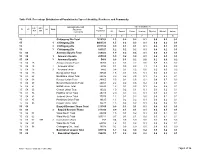
Table C-09: Percentage Distribution of Population by Type of disability, Residence and Community Administrative Unit Type of disability (%) UN / MZ / Total ZL UZ Vill RMO Residence WA MH Population Community All Speech Vision Hearing Physical Mental Autism 1 2 3 4 5 6 7 8 9 10 15 Chittagong Zila Total 7616352 1.3 0.2 0.2 0.1 0.5 0.2 0.1 15 1 Chittagong Zila 4463723 1.5 0.2 0.3 0.1 0.6 0.2 0.1 15 2 Chittagong Zila 2971102 0.9 0.1 0.1 0.1 0.4 0.1 0.1 15 3 Chittagong Zila 181527 1.2 0.2 0.2 0.1 0.4 0.2 0.1 15 04 Anowara Upazila Total 259022 1.9 0.2 0.4 0.1 0.8 0.3 0.1 15 04 1 Anowara Upazila 253556 1.9 0.2 0.4 0.1 0.8 0.3 0.1 15 04 3 Anowara Upazila 5466 0.8 0.1 0.2 0.0 0.2 0.0 0.2 15 04 15 Anowara Union Total 10260 4.2 0.3 2.2 0.6 0.8 0.2 0.2 15 04 15 1 Anowara Union 4794 8.1 0.5 4.5 1.1 1.5 0.3 0.3 15 04 15 3 Anowara Union 5466 0.8 0.1 0.2 0.0 0.2 0.0 0.2 15 04 19 Bairag Union Total 30545 1.8 0.1 0.5 0.1 0.6 0.3 0.1 15 04 28 Barakhain Union Total 28836 3.0 0.2 0.5 0.1 1.8 0.3 0.1 15 04 38 Barasat Union Total 28865 2.5 0.2 0.6 0.2 0.8 0.7 0.2 15 04 47 Burumchhara Union Total 20061 2.2 0.2 0.6 0.2 1.0 0.1 0.1 15 04 57 Battali Union Total 23630 1.3 0.1 0.2 0.1 0.5 0.2 0.1 15 04 66 Chatari Union Total 19022 1.0 0.2 0.1 0.1 0.3 0.2 0.1 15 04 76 Haildhar Union Total 25315 2.0 0.4 0.3 0.1 0.7 0.3 0.1 15 04 81 Juidandi Union Total 17575 1.2 0.1 0.2 0.0 0.6 0.1 0.1 15 04 85 Paraikora Union Total 19635 1.3 0.2 0.2 0.1 0.6 0.2 0.1 15 04 95 Roypur Union Total 35278 1.5 0.2 0.2 0.1 0.6 0.2 0.1 15 06 Bayejid Bostami Thana Total 211355 0.9 0.1 0.1 0.1 0.4 0.1 0.1 15 06 2 Bayejid Bostami Thana 211355 0.9 0.1 0.1 0.1 0.4 0.1 0.1 15 06 01 Ward No-01 Total 29209 1.5 0.1 0.2 0.1 0.9 0.1 0.1 15 06 02 Ward No-02 Total 103314 0.7 0.1 0.1 0.0 0.3 0.1 0.1 15 06 02 998 2 Cantonment (Part) 758 0.4 0.0 0.0 0.0 0.1 0.0 0.3 15 06 03 Ward No-03 Total 68794 1.2 0.1 0.2 0.1 0.5 0.2 0.1 15 06 98 Chittagang Cnt. -

List of 50 Bed Hospital
List of 50 Bed UHC No. of Sl. No. Organization Name Division Name District Name Upazila Name Bed 1 Amtali Upazila Health Complex, Barguna Barisal Barguna Amtali 50 2 Betagi Upazila Health Complex, Barguna Barisal Barguna Betagi 50 3 Patharghata Upazila Health Complex, Barguna Barisal Barguna Patharghata 50 4 Agailjhara Upazila Health Complex, Barishal Barisal Barishal Agailjhara 50 5 Gournadi Upazila Health Complex, Barishal Barisal Barishal Gaurnadi 50 6 Muladi Upazila Health Complex, Barishal Barisal Barishal Muladi 50 7 Borhanuddin Upazila Health Complex, Bhola Barisal Bhola Burhanuddin 50 8 Charfession Upazila Health Complex, Bhola Barisal Bhola Charfession 50 9 Daulatkhan Upazila Health Complex, Bhola Barisal Bhola Daulatkhan 50 10 Lalmohan Upazila Health Complex, Bhola Barisal Bhola Lalmohan 50 11 Nalchithi Upazila Health Complex, Jhalokati Barisal Jhalokati Nalchity 50 12 Galachipa Upazila Health Complex, Patuakhali Barisal Patuakhali Galachipa 50 13 Kalapara Upazila Health Complex, Patuakhali Barisal Patuakhali Kalapara 50 14 Mathbaria Upazila Health Complex, Pirojpur Barisal Pirojpur Mathbaria 50 15 Nesarabad Upazila Health Complex, Pirojpur Barisal Pirojpur Nesarabad 50 16 Nasirnagar Upazila Health Complex, Brahmanbaria Chittagong Brahmanbaria Nasirnagar 50 17 Sarail Upazila Health Complex, Brahmanbaria Chittagong Brahmanbaria Sarail 50 18 Haziganj Upazila Health Complex, Chandpur Chittagong Chandpur Hajiganj 50 19 Kachua Upazila Health Complex, Chandpur Chittagong Chandpur Kachua 50 20 Matlab(daxin) Upazila Health Complex, -

Quarterly Report
Mayer Hashi Family Planning Project in Bangladesh (MH-II) QUARTERLY REPORT Reporting Period: January 1– March 31, 2016 Project Year 3, Quarter 2 Report Submitted to: Office of Population Health, Nutrition and Education United States Agency for International Development USAID/Dhaka By MH-II Project Associate Cooperative Agreement No. AID-388-LA-13-00002 Under Leader Award No. GPO-A-00-08-00007-00 Date of Submission April 30,2016 Table of Contents Acronyms and Abbreviations ......................................................................................................... 2 Executive Summary ........................................................................................................................ 5 Appendix 1. Activity Description and Achievements by IR ........................................................ 16 Appendix 2: Indicator Tracking Table ........................................................................................ 137 Appendix 3: Findings from QA and FP Compliance Monitoring Visit...................................... 141 Appendix 4: Number of districts coverage with MH-II key Intervention in Q2 ........................ 143 1 Acronyms and Abbreviations ANC Antenatal care AUFPO Assistant Upazilla Family Planning Officer BRAC Bangladesh Rural Advancement Committee BCC Behavior change communication BCCWG Behavior Change Communication Working Group BEPZ Bangladesh Export Processing Zone BGMEA Bangladesh Garment Manufacturers and Exporters Association BKMI Bangladesh Knowledge management Iniative BMRC -

Inventory of LGED Road Network, March 2005, Bangladesh
BASIC INFORMATION OF ROAD DIVISION : CHITTAGONG DISTRICT : CHITTAGONG ROAD ROAD NAME CREST TOTAL SURFACE TYPE-WISE BREAKE-UP (Km) STRUCTURE EXISTING GAP CODE WIDTH LENGTH (m) (Km) EARTHEN FLEXIBLE BRICK RIGID NUMBER SPAN NUMBER SPAN PAVEMENT PAVEMENT PAVEMEN (m) (m) (BC) (WBM/HBB/ T BFS) (CC/RCC) 1 2 3 4 5 6 7 8 9 10 11 12 UPAZILA : RANGUNIA ROAD TYPE : UPAZILA ROAD 415702002 Dovashi Bazar Rd- Chandraghona Hospital.Road.4.40 0.980.00 0.98 0.00 0.00 2 8.00 0 0.00 415702003 R&H - Rajarhat Rd. 2.60 1.501.50 0.00 0.00 0.00 4 21.22 1 16.00 415702004 Dhamirhat - Rajarhat Rd. 4.00 1.400.86 0.00 0.54 0.00 3 16.70 0 0.00 415702006 Hazee Sayed Ali Road (UZR #98) 4.00 15.009.00 0.00 6.00 0.00 28 93.56 3 63.00 415702008 Kalurghat-Sarandeep-Banderjari-Sharafvatta Rd 3.05 6.205.50 0.00 0.70 0.00 24 345.65 3 47.10 (Rangunia Part) (UZR #96) 415702009 Shishutal-Ranirhat Connect Rd. (UZR #97) 7.32 4.251.55 2.70 0.00 0.00 11 71.50 0 0.00 415702010 Parua D. C. Rd. (UZR #99) 4.00 14.005.22 1.95 6.83 0.00 9 64.30 1 80.00 415702011 Ramgotirhat-Santirhat-Pomra Rd. (UZR #102)4.00 7.001.00 0.50 5.50 0.00 14 35.10 0 0.00 415702012 SagunBagicha-Hosnabad Rd. (UZR #103) 4.00 8.055.65 0.00 2.40 0.00 4 36.70 2 70.00 415702013 Ramgotirhat-Lamburhat-PasKhain-Bramanhat Rd 7.32 0.700.00 0.00 0.70 0.00 3 23.00 0 0.00 (Rangunia Part) (UZR #104) UPAZILA ROAD TOTAL: 10 Nos.