Quarterly Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bangladesh - Researched and Compiled by the Refugee Documentation Centre of Ireland on Friday 20 November 2015
Bangladesh - Researched and compiled by the Refugee Documentation Centre of Ireland on Friday 20 November 2015 Treatment of Jamaat-e-Islami/Shibir(student wing) by state/authorities In June 2015 a report published by the United States Department of State commenting on events of 2014 states: “ICT prosecutions of accused 1971 war criminals continued. No verdicts were announced until November, when the ICT issued death sentences in separate cases against Motiur Rahman Nizami and Mir Quasem Ali. At the same time, the Supreme Court Appellate Division upheld one of two death sentences against Mohammad Kamaruzzaman. All three men were prominent Jamaat leaders, and Jamaat called nationwide strikes in protest” (United States Department of State (25 June 2015) 2014 Country Reports on Human Rights Practices – Bangladesh). This report also states: “On August 10, Shafiqul Islam Masud, assistant secretary of the Jamaat-e-Islami Dhaka City Unit, was arrested, charged, and held in police custody with 154 others for arson attacks and vandalism in 2013. He was arrested and held four additional times in August and September 2014. According to a prominent human rights lawyer, Masud's whereabouts during his detentions were unknown, and lawyers were not allowed to speak with him. Defense lawyers were not allowed to speak before the court during his September 23 and 25 court appearances” (ibid). This document also points out that: “In some instances the government interfered with the right of opposition parties to organize public functions and restricted the broadcasting of opposition political events. Jamaat's appeal of a 2012 Supreme Court decision cancelling the party's registration continued” (ibid). -

{Ef<B$Fl{Qil:Cng<
:.":nE 3:+i:1i i,tti1.,-1 it"1--t ffi *,..:-j qsDqBfre'er$FFTI qER {o)l tF= F- -= Sffiffi-$t*** mffi *ffi {ef<B$fl{qil:cng< [-Irhan f)evelopment Direetorate (UDD) -ry Tqr{ € ut"tN{EfctfdT*, enerqrsfi <t(Ekm.ttrsK I s.i1.q.&'6 Introductirn r ..1.1 ;, id --!-.j,rtrlrj<- n - tI€qI . Histon of L-rban De 05 sss Project , &rttrr"ix q-q rc;(Eq'iildr $]T rF{ c+rrtr+ S"rGrqF i,: D:r elcrpment 16 . &i'ilr3*Ff q-< fgfeEt6-d 166 aa 5fr;11 qaj f,urrp; . 'SFr;i 6l€i5f f?i<rii +z< a<;rtc'fl"I-{r-|l< qicm e?:== ,] _i8 eft{tffim ad.mroffid}rfl . r,,ercq"rc:r$ ?l;{ sK s3'<MK hU" <.s i} ftu g.:+ J 5<;- Fl,r.-<i hurdaii,u er Snet:ic Guidelines for 19 qh,r " ltEftr rqEK ii<ffiR B"rcq6rK EdR{ 1fiq6q; 6csa; PLiii: : nS B en a:ul e--le.sor: Hi av Corridor . qfta Erfr"r <rqt"t'rtr+ gfi <r<<rrr< rrrrzx sarF€{q eFE lmpiernenmrir,l Slfir-. Or- Der elopment Plen For Cor's bazar To*-n ,\nd Sea Beach p rir<s"it L TO Teknaf 22 . Preparation of Der elopment Plan tbr q'rk \[irsharai 23 " Edr;r qf{Iig(-T Sbsa clq r?lm rfrn ma lf,s a.c Upazila. China-eong District: Risk Sensiti'r'e qBrIAgi <s:f$M ft(+" ufrcs"lt Research . frqqqrmTqftrebiB-{ \a . q"fftfu ' Resealcl-i Entitle.l \;rrr -:-:. : I- :.:.,: tr' :-,-,pntent 25 'rc<T$f{Rms s Vfr<raqfr+rfiR@3t' \s Dilectolrte (L'DDt since i.r,--< (<;Tlc{r{-{r"11-{ qttem okrq< cqsnB . -

Bangladesh Needs Assessment Working Group (NAWG) Report on Landslides
Bangladesh Needs Assessment Working Group (NAWG) Report on Landslides Landslides, Bangladesh, June 2017 Report date: 19 June 2017 (Source: UNICEF) Md. Yousuf Ali, Director-MIM, DDM, Email: [email protected] Contact for Inquiries: Arshad Muhammad, Assistant Country Director – Programs , CARE, Email: [email protected] Landslides, Bangladesh June 2017 Contents Contents 2 Background 3 Key Findings 4 Context of the Affected Area 6 Key characteristics of the affected districts by the landslides 8 Situation Overview 10 Detailed Findings 15 Access and Infrastructure 15 Communication 16 Child Protection 18 Education 19 Food Security 20 Livelihoods and Income 20 Gender Based Violence 21 Gender 23 Health 23 Market 25 Nutrition 26 Shelter 27 Water, Sanitation and Hygiene (WASH) 28 Annex A: Affected people per Upazila 30 2 Landslides, Bangladesh June 2017 Background On June 13th the districts of Bandarban, Chittagong, Rangamati, Khagrachari and Cox’s Bazaar suffered from possibly the deadliest landslides in their history. The disaster killed an estimated 160 persons, including 115 persons in Rangamati alone. According to the Chittagong Divisional Health Office Control Room Report, a total of 187 injured persons were admitted in local level hospitals. Approximately 85% of patients were admitted in Rangamati. While landslide related disaster occurs nearly every year, the second highest death toll of 127 deceased persons was recorded in 2007 [Disaster Forum, June 2017]. Monsoon rains caused severe flooding in low-lying areas to significantly damage road and communication infrastructure. Flood water rendered remote communities in Bandarban, Chittagong, and Rangamati districts were inaccessible by road. On June 14th, mudslides in southeast Bangladesh claimed additional lives in Cox's Bazaar and Khagrachari districts to further damage homes and infrastructure. -

Climate Change Adaptation Project Preparation in LGED Context And
Climate Change and Bangladesh: Optimization of Projects for LGED Monzur Sadeque Executive Engineer (Planning), LGED 1 Scope of the Presentation • LGED & Climate Change Adaptation Projects • Unutilized & Underutilized Potentials • Scopes of Different Sectors • LGED’s Responsibilities • Near Future Projects 2 Himalaya Bay of Bangle A Sand witch Country between the Mountain and the Sea 3 Background • The country is lying in front of natural disasters ; flood and cyclone storms • Climate change impacts increasing natural disasters with other impacts like sea level rise, salinity intrusion, draught, extreme weather, erosion, drainage congestion etc. 4 Background • The country is vulnerable to climate change due to climatic, physiographic and socio economic factors like population, low income, poor resource management etc. • Needs solution of present problems as well as future anticipated problems….. 5 What are the Risks ? 6 Mainstreaming the Risks • In 1990s- WOMEN IN DEV. (WID) • In 2000s- Environment & Sustainable Development • In 2010s- Climate Mainstreaming 7 Climate Change Projects-LGED Name of Financed Area the Project and By Estimated Cost (Crore Tk) CDTA/ PPTA/PDA for ADB Amtoli, Coastal Towns (Climate Galachipa,Pirozep Infrastructure Improvement Investment ur, Mathbaria, Project (3 projects) Fund) Daulatkhan, 48.52 Bhola, Kalapara, Barguna Coastal Towns ADB -Same- Infrastructure Improvement (CIF) Project 876.00 8 Climate Change Projects-LGED Name of Financed Area the Project and By Estimated Cost (Crore Tk) CDTA/ PPTA/PDA for ADB Amtoli, Coastal Towns (Climate Galachipa,Pirozep Infrastructure Improvement Investment ur, Mathbaria, Project (3 projects) Fund) Daulatkhan, 48.52 Bhola, Kalapara, Barguna Coastal Towns ADB -Same- Infrastructure Improvement (CIF) Project 876.00 9 Climate Change Projects-LGED Name of Financed Area the Project & Estimated By Cost (Crore Tk. -

Chapter-Vi : Socio-Economic Profile of the Study Area
Chapter-vi : Socio-economic Profile of the Study Area 189---198 Physical feature and socio-historical background Demography Literacy Administrative Unit Transport Communications Socio-economic Profile ofthe Study Area 189 For a proper understanding of the problem, it is essential to briefly refer to an ecological profile of Kushtia district as the values and characteristics of the masses very much depend upon, and are influenced by geographical, economic, social and political background of the area. Physical feature and socio-historical background Kushtia is not an ancient township but one of the eighteen oldest districts in independent Bangladesh. There is no much evidence to know the ancient history of Kushtia. The only tool to be informed about the district what was portrayed through description by different persons based on different regimes in the region governed. Hamilton's Gazetteer has mentioned of Kushtia town and of the fact that the local people called the town Kushtay (Kushte). In Tolemy's map, several little islands have been portrayed under the Ganges basin. These islands are considered as ancient Kushtia. 1 The district was under Natore Zemindar in 1725. Then it was under Rajshahi civil administration of Kanadarnagar Pargana. 2 Later East India Company transferred Kushtia under Jessore district in 1776. It was brought under Pabna district in 1828. Then Mahkuma Administration was established under Kushtia in 1861 and then brought under Nadia district.3 During the British rule, railway connection with Kolkata, capital of British India, established in 1860, made the town an alluring location for mills and factories, including the Jagneshwar Engineering Works (1896), Renwick and Company ( 1904 ), and the Mohini Mills (1919). -

Bangladesh Rice Journal Bangladesh Rice Journal
ISSN 1025-7330 BANGLADESH RICE JOURNAL BANGLADESH RICE JOURNAL BANGLADESH RICE JOURNAL VOL. 21 NO. 2 (SPECIAL ISSUE) DECEMBER 2017 The Bangladesh Rice Journal is published in June and December by the Bangladesh Rice Research Institute (BRRI). The journal is a peer reviewed one based on original Theme : Cropping Patterns of Bangladesh research related to rice science. The manuscript should be less than eight printed journal pages or about 12 type written pages. An article submitted to the Bangladesh Rice Journal must not have been published in or accepted for publication by any other journal. DECEMBER 2017 ISSUE) NO. 2 (SPECIAL VOL. 21 Changes of address should be informed immediately. Claims for copies, which failed to reach the paid subscribers must be informed to the Chief Editor within three months of the publication date. Authors will be asked to modify the manuscripts according to the comments of the reviewers and send back two corrected copies and the original copy together to the Chief Editor within the specified time, failing of which the paper may not be printed in the current issue of the journal. BRJ: Publication no.: 263; 2000 copies BANGLADESH RICE RESEARCH INSTITUTE Published by the Director General, Bangladesh Rice Research Institute, Gazipur 1701, Bangladesh GAZIPUR 1701, BANGLADESH Printed by Swasti Printers, 25/1, Nilkhet, Babupura, Dhaka 1205 ISSN 1025-7330 BANGLADESH RICE JOURNAL VOL. 21 NO. 2 (SPECIAL ISSUE) DECEMBER 2017 Editorial Board Chief Editor Dr Md Shahjahan Kabir Executive Editors Dr Md Ansar Ali Dr Tamal Lata Aditya Associate Editors Dr Krishna Pada Halder Dr Md Abdul Latif Dr Abhijit Shaha Dr Munnujan Khanam Dr AKM Saiful Islam M A Kashem PREFACE Bangladesh Rice Journal acts as an official focal point for the delivery of scientific findings related to rice research. -
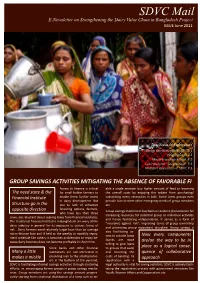
SDVC Mail E-Newsletter on Strengthening the Dairy Value Chain in Bangladesh Project ISSUE June 2011
SDVC Mail E-Newsletter on Strengthening the Dairy Value Chain in Bangladesh Project ISSUE June 2011 The Areas of Exploration Savings activities inside SDVC P.1 Progress in AI P.2 Micro‐Franchise Model P.2 Case study on “Sangrampur” P.3 Midterm evaluation of SDVC P.3 GROUP SAVINGS ACTIVITIES MITIGATING THE ABSENCE OF FAVORABLE FI Access to finance is critical able a single member buy higher amount of feed to lessening The need state & the for small holder farmers to the overall costs by enjoying the rebate from purchasing/ Financial Institute enable them further invest subscribing every necessities in bulk. Some times groups even in dairy development. But provide loan to meet other emergency needs of group members Structure go in the due to lack of attractive etc. financing options, farmers, opposite direction Group savings mechanism has been an evident phenomenon for who have less than three increasing resources for potential group or individual activities cows, are reluctant about seeking loans from financial institutes. and hence facilitating independence. It serves as a form of The traditional financial institutes in Bangladesh are wary of the “insurance against risk”; improving sense of group ownership dairy industry in general for its exposure to various forms of and promoting group repayment discipline. Group savings is risk . Dairy farmers need relatively larger loan than an average also facilitating ac‐ micro‐finance loan and if held to the weekly or monthly repay‐ cess to outside loans Now every components ment schedule like others, it becomes problematic to repay be‐ (banks are more cause dairy business does not become profitable in short time. -

Project Plan 3-5 Years
PROJECT DESIGN FORM1 Project title: Enhancing CBID in Bangladesh Region: SAR Country: Bangladesh Partner Name Centre for Disability in Development (CDD) Project start 1 January 2020 – 31 December 2022 /end date: Project Number Applied (if available): 1 This Form is to be used for planning of all projects with a total budget of >50,000 EUR. The term “Project” within the document always also refers to Programmes. For projects with an overall project budget of <50,000 EUR, the following documents are to be submitted: i) Project Idea and Programmatic Approval Form (PPA) Section I. A-C + Section II.; ii) Logical Framework and Cost plan CBM International - Project Design Form Version 1.0 (approved June 2018) 1 Contents I. Project Abstract 3 II. Full Project Design 8 1. Relevance of the Project 8 2. Effectiveness and quality 12 3. Efficiency 20 4. Sustainability and Contribution to Change 23 III. Annexes A. Description of Project context 26 B. Logical framework / cost plan 36 C. Activity schedule 36 D. Risk Register 36 E. Monitoring and Evaluation (M&E) Plan 36 F. Quality criteria for Project Design 37 CBM International - Project Design Form Version 1.0 (approved June 2018) 2 I. Project Abstract A) Project Information Name of Partner Centre for Disability in Development Region: SAR Country: Bangladesh Project title Enhancing CBID in Bangladesh Project Location Chittagong City Corporation Ward No. 13, 14 & 15 and Bashkhali and Rangunia Sub-Districts of Chittagong District. Timeframe 1st January 2020-31st December 2022 Target group Direct Beneficiaries of the project are at least 2,000 persons with disabilities. -

Bid Document Supply and Installation of Shop Signage in 279 Upazilas
Tender Document Ref. No.: 20201001/ Rural Electrification and Renewable Energy Development Project-II (REREDP-II) - Additional Financing-II TENDER DOCUMENT FOR THE PROCUREMENT OF GOODS For IDA Financed Project Name of the Tender: Supply and Installation of Shop Signage in 279 Upazilas for IDCOL (3 Lots) Lot-1: Supply and Installation of Shop Signage in 81 Upazilas Lot-2: Supply and Installation of Shop Signage in 87 Upazilas Lot-3: Supply and Installation of Shop Signage in 111 Upazilas (Through National Competitive Bidding) Invitation for Tender No. : IDCOL/2020/OCT/NCB/01 Issued on : 04 October 2020 Tender Package No. : G-33 under REREDP-II (AF-II) Infrastructure Development Company Limited UTC Building (Level-16), 8 Panthapath, Kawran Bazar, Dhaka-1215 IDCOL NCB G-33 under REREDPII-AF-II / SIGNAGE i Table of Contents Section 1. Instructions to Tenderers ................................................................... 1 A. General ....................................................................................................................... 1 1. Scope of Tender ........................................................................................................... 1 2. Interpretation ................................................................................................................ 1 3. Source of Funds ........................................................................................................... 1 4. Corrupt, Fraudulent, Collusive or Coercive Practices ............................................ -

List of Trainees of Egp Training
Consultancy Services for “e-GP Related Training” Digitizing Implementation Monitoring and Public Procurement Project (DIMAPPP) Contract Package # CPTU/S-03 Central Procurement Technical Unit (CPTU), IMED Ministry of Planning Training Time Duration: 1st July 2020- 30th June 2021 Summary of Participants # Type of Training No. of Participants 1 Procuring Entity (PE) 876 2 Registered Tenderer (RT) 1593 3 Organization Admin (OA) 59 4 Registered Bank User (RB) 29 Total 2557 Consultancy Services for “e-GP Related Training” Digitizing Implementation Monitoring and Public Procurement Project (DIMAPPP) Contract Package # CPTU/S-03 Central Procurement Technical Unit (CPTU), IMED Ministry of Planning Training Time Duration: 1st July 2020- 30th June 2021 Number of Procuring Entity (PE) Participants: 876 # Name Designation Organization Organization Address 1 Auliullah Sub-Technical Officer National University, Board Board Bazar, Gazipur 2 Md. Mominul Islam Director (ICT) National University Board Bazar, Gazipur 3 Md. Mizanoor Rahman Executive Engineer National University Board Bazar, Gazipur 4 Md. Zillur Rahman Assistant Maintenance Engineer National University Board Bazar, Gazipur 5 Md Rafiqul Islam Sub Assistant Engineer National University Board Bazar, Gazipur 6 Mohammad Noor Hossain System Analyst National University Board Bazar, Gazipur 7 Md. Anisur Rahman Programmer Ministry Of Land Bangladesh Secretariat Dhaka-999 8 Sanjib Kumar Debnath Deputy Director Ministry Of Land Bangladesh Secretariat Dhaka-1000 9 Mohammad Rashedul Alam Joint Director Bangladesh Rural Development Board 5,Kawranbazar, Palli Bhaban, Dhaka-1215 10 Md. Enamul Haque Assistant Director(Construction) Bangladesh Rural Development Board 5,Kawranbazar, Palli Bhaban, Dhaka-1215 11 Nazneen Khanam Deputy Director Bangladesh Rural Development Board 5,Kawranbazar, Palli Bhaban, Dhaka-1215 12 Md. -

Bounced Back List.Xlsx
SL Cycle Name Beneficiary Name Bank Name Branch Name Upazila District Division Reason for Bounce Back 1 Jan/21-Jan/21 REHENA BEGUM SONALI BANK LTD. NA Bagerhat Sadar Upazila Bagerhat Khulna 23-FEB-21-R03-No Account/Unable to Locate Account 2 Jan/21-Jan/21 ABDUR RAHAMAN SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number SHEIKH 3 Jan/21-Jan/21 KAZI MOKTADIR HOSEN SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 4 Jan/21-Jan/21 BADSHA MIA SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 5 Jan/21-Jan/21 MADHAB CHANDRA SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number SINGHA 6 Jan/21-Jan/21 ABDUL ALI UKIL SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 7 Jan/21-Jan/21 MRIDULA BISWAS SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 8 Jan/21-Jan/21 MD NASU SHEIKH SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 9 Jan/21-Jan/21 OZIHA PARVIN SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 10 Jan/21-Jan/21 KAZI MOHASHIN SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 11 Jan/21-Jan/21 FAHAM UDDIN SHEIKH SONALI BANK LTD. NA Chitalmari Upazila Bagerhat Khulna 16-FEB-21-R04-Invalid Account Number 12 Jan/21-Jan/21 JAFAR SHEIKH SONALI BANK LTD. -

POPULATION & HOUSING CENSUS-2011 -..:: Bangladesh
POPULATION & HOUSING CENSUS-2011 COMMUNITY REPORT : JHENAIDAH Bangladesh Bureau of Statistics Statistics and Informatics Division Ministry of Planning BANGLADESH POPULATION AND HOUSING CENSUS 2011 COMMUNITY REPORT Zila: JHENAIDAH February 2015 BANGLADESH BUREAU OF STATISTICS (BBS) STATISTICS AND INFORMATICS DIVISION (SID) MINISTRY OF PLANNING GOVERNMENT OF THE PEOPLE’S REPUBLIC OF BANGLADESH ISBN-978-984-33-8587-1 COMPLIMENTARY Published by Bangladesh Bureau of Statistics (BBS) Statistics and Informatics Division (SID) Ministry of Planning Website: www.bbs.gov.bd This book or any portion thereof cannot be copied, microfilmed or reproduced for any commercial purpose. Data therein can, however, be used and published with acknowledgement of their sources. Contents Page Message of Honorable Minister, Ministry of Planning v Message of Honorable State Minister, Ministry of Finance and Ministry of Planning vii Foreword ix Preface xi Census results at national, divisional and zila level xiii Physical features of Jhenaidah zila xiv Map of Jhenaidah zila xv Geo-code of Jhenaidah zila, upazila and union/ward xvi Chapter-1: Introductory notes on census 1 Chapter-2: Concepts and definitions 7 Chapter-3: Summary findings 3.1: Harinakundu upazila 11 3.2: Jhenaidah Sadar upazila 15 3.3: Kaliganj upazila 19 3.4: Kotchandpur upazila 23 3.5: Maheshpur upazila 27 3.6: Shailkupa upazila 31 Chapter-4: Community tables Table C-01: Area, household, population and density by residence and community 37 Table C-02: Distribution of household, population by sex, residence