Senate Committee Substitute for Senate Bill No
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Compensation Manual
Compensation Manual Fiscal Year 2020-21 Last Updated 6/8/2021 Department of Human Resources / Classification and Compensation Division Legal Notices The Department of Human Resources (DHR) makes available this information, subject to the following terms and conditions. By keeping this file, you agree to the terms and conditions as outlined in this legal notice. DHR reserves the right to change these terms and conditions from time to time at its sole discretion. Use of Software. The software and accompanying documentation that are made available to download from this Web site are the copyrighted work of Adobe and/or its suppliers. Use of the software is governed by the terms of the end user license agreement, which accompanies or is included with such software. You will not be able to download or install any software that is accompanied by or includes an end user license agreement unless you agree to the terms of such end user license agreement. If you do not agree to these terms, you will not be able to use the software. Use of Manual Information. Except as otherwise indicated elsewhere on this site, you may view, copy, print, and distribute this document available in this manual subject to the following conditions: 1. The document may be used solely for personal, informational, non-commercial purposes; 2. The document may not be modified or altered in any way; 3. Any copy of the document or portion thereof must include this permission notice; and 4. DHR reserves the right to revoke such authorization at any time, and any such use shall be discontinued immediately upon written notice from Adobe. -

A File in the Online Version of the Kouroo Contexture (Approximately
SETTING THE SCENE FOR THOREAU’S POEM: YET AGAIN WE ATTEMPT TO LIVE AS ADAM 11th Century 1010s 1020s 1030s 1040s 1050s 1060s 1070s 1080s 1090s 12th Century 1110s 1120s 1130s 1140s 1150s 1160s 1170s 1180s 1190s 13th Century 1210s 1220s 1230s 1240s 1250s 1260s 1270s 1280s 1290s 14th Century 1310s 1320s 1330s 1340s 1350s 1360s 1370s 1380s 1390s 15th Century 1410s 1420s 1430s 1440s 1450s 1460s 1470s 1480s 1490s 16th Century 1510s 1520s 1530s 1540s 1550s 1560s 1570s 1580s 1590s 17th Century 1610s 1620s 1630s 1640s 1650s 1660s 1670s 1680s 1690s 18th Century 1710s 1720s 1730s 1740s 1750s 1760s 1770s 1780s 1790s 19th Century 1810s Alas! how little does the memory of these human inhabitants enhance the beauty of the landscape! Again, perhaps, Nature will try, with me for a first settler, and my house raised last spring to be the oldest in the hamlet. To be a Christian is to be Christ- like. VAUDÈS OF LYON 1600 William Gilbert, court physician to Queen Elizabeth, described the earth’s magnetism in DE MAGNETE. Robert Cawdrey’s A TREASURIE OR STORE-HOUSE OF SIMILES. Lord Mountjoy assumed control of Crown forces, garrisoned Ireland, and destroyed food stocks. O’Neill asked for help from Spain. HDT WHAT? INDEX 1600 1600 In about this year Robert Dudley, being interested in stories he had heard about the bottomlessness of Eldon Hole in Derbyshire, thought to test the matter. George Bradley, a serf, was lowered on the end of a lengthy rope. Dudley’s little experiment with another man’s existence did not result in the establishment of the fact that holes in the ground indeed did have bottoms; instead it became itself a source of legend as spinners would elaborate a just-so story according to which serf George was raving mad when hauled back to the surface, with hair turned white, and a few days later would succumb to the shock of it all. -

The Recovery of Manuscripts
Cultural heritage The Recovery of manuscripts David RUNDLE ABSTRACT Manuscripts were the cornerstone of humanism. They had been the main vector for transmission of the ancient texts and culture in the Middle Ages. Most of them had nonetheless been lost or forgotten in remote libraries. In order to recover the ancient Greek and Latin texts they favoured, humanists went on a European quest to find these manuscripts. From Italy, at first, humanists travelled all across Europe, visiting convents and libraries, in search of the lost works of Tacitus, Cicero, etc. building and securing the antique legacy of European culture. Portrait of Poggio holding a manuscript on the first page of the Ruins of Rome (Biblioteca apostolica Vaticana, Urb. Lat. 224, fol. 3). This treatise dedicated to another prominent manuscript hunter, the pope Nicholas V, is a meditation on the loss of Roman culture. Manuscripts were humanism’s lifeblood, its inspiration and its purpose. The production of new books in a new, or revived, style of Latin and with a new, or revived, presentation on the page was central to their activities. But before they could even be conceived, there needed to be classical texts to be imitated. Behind the humanists’ practices lay an agenda of manuscript recovery all across Europe. They were conscious of themselves as cut off from the classical past and set themselves the challenge of discovering works which had not been seen—they said- —by scholars for centuries. In writing of their achievements in doing this, they exaggerated both their own heroic endeavours and the dire state that preceded them. -
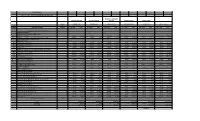
Unit Rate Cost Unit Rate Cost Unit Rate Cost Unit Rate Cost Unit Rate Cost Unit Rate Cost $427.00 $2,562.00 $0.00 $0.00 $250.00
PROGRAM 1410S -------- ---------------------------------- ------- August 22, 2019 - July 31, 2020 option through (July 2021) MERLIZ INC, DBA DOME FREDERIC PRINTING INV TECH SERVICES PRINTING MONARCH LITHO SCHMITZ PRESS BASIS AURORA, CO ROSWELL, GA MCCLELLAN, CA MONTEBELLO, CA SPARKS, MD GPO ESTIMATE ITEM OF NUMBER ITEM DESCRIPTION AWARD UNIT RATE COST UNIT RATE COST UNIT RATE COST UNIT RATE COST UNIT RATE COST UNIT RATE COST -------- ---------------------------------- ------- Category 1: Format A & Format B I. COMPLETE PRODUCT: A. Makeready and/or Setup per printed side (1) FORMAT A (14 x 20) 6 $427.00 $2,562.00 $0.00 $0.00 $250.00 $1,500.00 $695.00 $4,170.00 $247.00 $1,482.00 $308.00 $1,848.00 (2) FORMAT B (any trim size over 14x20, to include 24-1/2 x 40) 11 $369.00 $4,059.00 $0.00 $0.00 $500.00 $5,500.00 $730.00 $8,030.00 $247.00 $2,717.00 $372.00 $4,092.00 B. Running Rate per 1000 copies, per side 1 FORMAT A (14 x 20) (a) 1,000 through 29,999 copies 40 $75.00 $3,000.00 $125.11 $5,004.40 $58.84 $2,353.60 $57.00 $2,280.00 $42.90 $1,716.00 $63.61 $2,544.40 (b) 30,000 through 59,999 copies 30 $70.00 $2,100.00 $108.56 $3,256.80 $58.38 $1,751.40 $56.50 $1,695.00 $37.65 $1,129.50 $61.62 $1,848.60 (c) 60,000 through 89,999 copies 60 $65.00 $3,900.00 $99.23 $5,953.80 $56.06 $3,363.60 $56.00 $3,360.00 $34.85 $2,091.00 $59.02 $3,541.20 (d) 90,000 and over 90 $60.00 $5,400.00 $90.44 $8,139.60 $54.09 $4,868.10 $55.50 $4,995.00 $33.85 $3,046.50 $56.53 $5,087.70 2 FORMAT B (any trim size over 14x20, to include 24-1/2 x 40) (a) 1,000 through 29,999 -

The Ginger Fox's Two Crowns Central Administration and Government in Sigismund of Luxembourg's Realms
Doctoral Dissertation THE GINGER FOX’S TWO CROWNS CENTRAL ADMINISTRATION AND GOVERNMENT IN SIGISMUND OF LUXEMBOURG’S REALMS 1410–1419 By Márta Kondor Supervisor: Katalin Szende Submitted to the Medieval Studies Department, Central European University, Budapest in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Medieval Studies, CEU eTD Collection Budapest 2017 Table of Contents I. INTRODUCTION 6 I.1. Sigismund and His First Crowns in a Historical Perspective 6 I.1.1. Historiography and Present State of Research 6 I.1.2. Research Questions and Methodology 13 I.2. The Luxembourg Lion and its Share in Late-Medieval Europe (A Historical Introduction) 16 I.2.1. The Luxembourg Dynasty and East-Central-Europe 16 I.2.2. Sigismund’s Election as King of the Romans in 1410/1411 21 II. THE PERSONAL UNION IN CHARTERS 28 II.1. One King – One Land: Chancery Practice in the Kingdom of Hungary 28 II.2. Wearing Two Crowns: the First Years (1411–1414) 33 II.2.1. New Phenomena in the Hungarian Chancery Practice after 1411 33 II.2.1.1. Rex Romanorum: New Title, New Seal 33 II.2.1.2. Imperial Issues – Non-Imperial Chanceries 42 II.2.2. Beginnings of Sigismund’s Imperial Chancery 46 III. THE ADMINISTRATION: MOBILE AND RESIDENT 59 III.1. The Actors 62 III.1.1. At the Travelling King’s Court 62 III.1.1.1. High Dignitaries at the Travelling Court 63 III.1.1.1.1. Hungarian Notables 63 III.1.1.1.2. Imperial Court Dignitaries and the Imperial Elite 68 III.1.1.2. -

The Availability of Credit in the English Countryside, 1400–1480*
The availability of credit in the English countryside, 1400–1480* by Chris Briggs Abstract Credit was central to the peasant economy, but its supply varied over time. Using information from the records of three Cambridgeshire manorial courts and a church court, this article charts changes in the number of rural credit transactions initiated in the fifteenth century, and seeks explanations for them. It argues that new credit transactions declined in number in the period studied, though caution is required concerning the real extent of the decline. Legal and institutional changes arising from the decline of the manor courts and the rise of the church courts’ debt jurisdiction were key. It is argued that these changes were as important as monetary difficulties in shaping the willingness of rural lenders to give credit. Credit played a fundamental role in the agrarian economy of medieval England. In an era in which the supply of coined money was never sufficient to meet all the demands placed upon it, and in which the cash income of most rural households was concentrated at particular times of the year, the ability to obtain credit was essential. Most medieval English rural credit was extended by individuals rather than institutions or landlords, and usually flowed between villagers. In the countryside and more generally, later medieval credit took two main forms. The first was the straightforward loan of cash, grain or goods, while the second consisted of credit given in the form of a sale, most commonly in a deferred payment for goods or -

PEARL DRUMS UK Consumer Pricelist 2021 Pearl Drums | Pearl Percussion | Pearl Drum Pedals and Hardware
PEARL DRUMS UK Consumer Pricelist 2021 Pearl Drums | Pearl Percussion | Pearl Drum Pedals and Hardware Valid from 06.04.2021 1 OFFICE IN THE NETHERLANDS Pearl Music Europe B.V. Craenakker 28 NL-5951 CC Belfeld P.O.Box 1078 NL-5900 BB Venlo [email protected] KEY TO DRUM NUMBERING SYSTEM Serie Diameter Depth Type * ** Colour Masters Serie RF 22 18 B X 100 *: RFP 22 18 B B 102 B = Bass Drum F = Floortom MRV 18 16 F 160 T = Tom Tom RF 12 09 T 330 S = Snare Drum MRV 14 50 S D 102 **: Sonstige X = without BB3 MCT 22 16 B 351 B = with BB3 SSC 18 16 F 110 D = Snare Drum DMP 13 10 T 262 double STL- 100 lugs EXX 14 55 S 91 Snare Drums MRV 14 55 S STA 14 50 IP 14 65 2 PRODUCT INDEX Masterworks........................................................... 4 Reference Series..................................................... 11 Reference Pure Series............................................. 13 Masters Maple Gum................................................. 15 Masters Maple Reserve........................................... 16 Masters Maple Complete.......................................... 18 Session Studio Select............................................... 20 Crystal Beat............................................................. 21 Decade Maple Series................................................ 22 Export Lacquer Series ............................................. 23 Export Series........................................................... 24 Roadshow................................................................ 25 MidTown................................................................. -

NOTICE to CONGRESS: MONTHLY UPDATE on FLOOD MAPPING Biggert-Waters Flood Insurance Reform Act of 2012 and Homeowner Flood Insurance Affordability Act of 2014
NOTICE TO CONGRESS: MONTHLY UPDATE ON FLOOD MAPPING Biggert-Waters Flood Insurance Reform Act of 2012 and Homeowner Flood Insurance Affordability Act of 2014 December 2015 http://www.fema.gov/risk-mapping-assessment-planning TABLE OF CONTENTS 1. Introduction .................................................................................................................................... 1 2. Background ..................................................................................................................................... 2 3. Risk MAP Program ........................................................................................................................ 3 4. Notification ...................................................................................................................................... 3 4.1. Estimated Issuance of Preliminary Maps ................................................................................... 4 4.2. Estimated Issuance of Revised Preliminary Maps ...................................................................... 6 4.3. Actions Taken by the Administrator .......................................................................................... 7 5. Additional Information ............................................................................................................. 12 Appendix A: Flood Maps ................................................................................................................... 13 Appendix B: Acronyms ..................................................................................................................... -

The 1430S: a Period of Extraordinary Internal Climate Variability During the Early Spörer Minimum and Its Impacts in Northweste
The 1430s: A period of extraordinary internal climate variability during the early Spörer Minimum and its impacts in Northwestern and Central Europe Chantal Camenisch1,2, Kathrin M. Keller1,3, Melanie Salvisberg1,2, Benjamin Amann1,4,5, 5 Martin Bauch6, Sandro Blumer1,3, Rudolf Brázdil7,8, Stefan Brönnimann1,4, Ulf Büntgen1,8,9, Bruce M. S. Campbell10, Laura Fernández-Donado11, Dominik Fleitmann12, Rüdiger Glaser13, Fidel González-Rouco11, Martin Grosjean1,4, Richard C. Hoffmann14, Heli Huhtamaa1,2,15, Fortunat Joos1,3, Andrea Kiss16, Oldřich Kotyza17, Flavio Lehner18, Jürg Luterbacher19,20, Nicolas Maughan21, Raphael Neukom1,4, Theresa Novy22, Kathleen 10 Pribyl23, Christoph C. Raible1,3, Dirk Riemann13, Maximilian Schuh24, Philip Slavin25, Johannes P. Werner26, Oliver Wetter1,2 1Oeschger Centre for Climate Change Research, University of Bern, Bern, Switzerland 2Economic, Social, and Environmental History, Institute of History, University of Bern, Bern, Switzerland 3Climate and Environmental Physics, Physics Institute, University of Bern, Bern, Switzerland 15 4Institute of Geography, University of Bern, Bern, Switzerland 5Department of Geography and Planning, Queen's University, Kingston (ON), Canada 6German Historical Institute in Rome, Rome, Italy 7Institute of Geography, Masaryk University, Brno, Czech Republic 8Global Change Research Institute, Czech Academy of Sciences, Brno, Czech Republic 20 9Swiss Federal Research Institute WSL, Birmensdorf, Switzerland 10School of the Natural and Built Environment, The Queen’s University of -

Jack Waddell MEDIEVAL ARMS, ARMOR, and TACTICS And
MEDIEVAL ARMS, ARMOR, AND TACTICS And Interactive Qualifying Project Submitted to the faculty Of the WORCESTER POLYTECHNIC INSTITUTE In partial fulfillment of the requirements of the Degree of Bachelor or Science By Jack Waddell And 7 Brent Palermo Date: December 10th , 2002 Approved: Abstract This project examined and photographed nearly 300 examples of medieval arms and armor in the Higgins Armory collection, and documented the characteristics of armor, weapons, and their associated tactics during the middle ages (approximately 500CE to 1500CE) as well as the historical and technological background against which they were employed. 2 Acknowledgements We would like to thank the Higgins Armory Museum for providing us with access to authentic medieval artifacts and essential research tools. 3 Table of Contents 1. Abstract Vol 1, p 2 2. Acknowledgements 3 3. Table of Contents 4 4. Introduction (By Brent Palermo) 5 5. Historical background of the Middle Ages (By Jack Waddell) 6 a. History 6 b. Feudalism 35 c. War in the Middle Ages 40 d. Medieval Technology 47 6. Armor of the Middle Ages (By Jack Waddell) 55 a. Introduction 55 b. Armor for the Body 57 c. Armor for the Head 69 d. Armor for the Legs 78 e. Armor for the Arms 81 f. Shields 87 g. Snapshots of Armor Ensembles over Time 90 7. Weapons of the Middle Ages (By Brent Palermo) 100 a. Daggers 100 b. Swords 105 c. Axes 112 d. Halberds 115 e. Glaives 116 f. Bills 117 g. Maces 117 h. Morning Stars 118 i. Flails 119 j. War Hammers 120 k. -

Timetable 0T9NAAT
Cardiff Airport - Cardiff Service T9 (TCAT009) Bank Holiday Mondays (Inbound) Timetable valid from 7th October 2019 until further notice Operator: NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT Cardiff Airport (Terminal) 0010 0450 0510 0530 0550 0610 0630 0650 0710 0730 0750 0810 0830 0850 0910 0930 0950 1010 1030 Copthorne Hotel (Rhur Cross, Port Road) 0022s 0502s 0522s 0542s 0602s 0622s 0642s 0702s 0722s 0742s 0802s 0822s 0842s 0902s 0922s 0942s 1002s 1022s 1042s Cardiff Bay (Red Dragon Centre) 0040s 0520s 0540s 0600s 0620s 0640s 0700s 0720s 0740s 0800s 0820s 0840s 0900s 0920s 0940s 1000s 1020s 1040s 1100s Cardiff City Centre (Canal St) (Arr) 0045s 0525s 0545s 0605s 0625s 0645s 0705s 0725s 0745s 0805s 0825s 0845s 0905s 0925s 0945s 1005s 1025s 1045s 1105s Cardiff City Centre (Canal St) (Dep) -- 0530s 0550s 0610s 0630s 0650s 0710s 0730s 0750s 0810s 0830s 0850s 0910s 0930s 0950s 1010s 1030s 1050s 1110s Cardiff Centrail Rail Station -- 0531s 0551s 0611s 0631s 0651s 0711s 0731s 0751s 0811s 0831s 0851s 0911s 0931s 0951s 1011s 1031s 1051s 1111s Operator: NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT NADT Cardiff Airport (Terminal) 1050 1110 1130 1150 1210 1230 1250 1310 1330 1350 1410 1430 1450 1510 1530 1550 1610 1630 1650 Copthorne Hotel (Rhur Cross, Port Road) 1102s 1122s 1142s 1202s 1222s 1242s 1302s 1322s 1342s 1402s 1422s 1442s 1502s 1522s 1542s 1602s 1622s 1642s 1702s Cardiff Bay (Red Dragon Centre) 1120s 1140s 1200s 1220s 1240s 1300s 1320s 1340s -

February 2017
February 2017 Table of Contents Table of Contents ......................................................................................................................................... i List of Figures ............................................................................................................................................ iii List of Tables .............................................................................................................................................. iv Acronyms .................................................................................................................................................... vi Executive Summary ................................................................................................................................. viii Chapter 1. Background .............................................................................................................................. 2 1.1 Purpose of this Plan ............................................................................................................................ 2 1.1.1 Problem this Program Addresses ................................................................................................................... 2 1.1.2 Mid-Columbia Coho History ......................................................................................................................... 3 1.1.3 Local Adaptation ...........................................................................................................................................