Risk Analysis Draft May 2008
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Risk Assessment Guidance
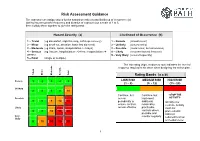
Risk Assessment Guidance The assessor can assign values for the hazard severity (a) and likelihood of occurrence (b) (taking into account the frequency and duration of exposure) on a scale of 1 to 5, then multiply them together to give the rating band: Hazard Severity (a) Likelihood of Occurrence (b) 1 – Trivial (eg discomfort, slight bruising, self-help recovery) 1 – Remote (almost never) 2 – Minor (eg small cut, abrasion, basic first aid need) 2 – Unlikely (occurs rarely) 3 – Moderate (eg strain, sprain, incapacitation > 3 days) 3 – Possible (could occur, but uncommon) 4 – Serious (eg fracture, hospitalisation >24 hrs, incapacitation >4 4 – Likely (recurrent but not frequent) weeks) 5 – Very likely (occurs frequently) 5 – Fatal (single or multiple) The risk rating (high, medium or low) indicates the level of response required to be taken when designing the action plan. Trivial Minor Moderate Serious Fatal Rating Bands (a x b) Remote 1 2 3 4 5 LOW RISK MEDIUM RISK HIGH RISK (1 – 8) (9 - 12) (15 - 25) Unlikely 2 4 6 8 10 Continue, but Continue, but -STOP THE Possible review implement ACTIVITY- 3 6 9 12 15 periodically to additional Identify new ensure controls reasonably controls. Activity Likely remain effective practicable must not controls where 4 8 12 16 20 proceed until possible and risks are Very monitor regularly reduced to a low likely 5 10 15 20 25 or medium level 1 Risk Assessments There are a number of explanations needed in order to understand the process and the form used in this example: HAZARD: Anything that has the potential to cause harm. -

Guidelines for Human Exposure Assessment Risk Assessment Forum
EPA/100/B-19/001 October 2019 www.epa.gov/risk Guidelines for Human Exposure Assessment Risk Assessment Forum EPA/100/B-19/001 October 2019 Guidelines for Human Exposure Assessment Risk Assessment Forum U.S. Environmental Protection Agency DISCLAIMER This document has been reviewed in accordance with U.S. Environmental Protection Agency (EPA) policy. Mention of trade names or commercial products does not constitute endorsement or recommendation for use. Preferred citation: U.S. EPA (U.S. Environmental Protection Agency). (2019). Guidelines for Human Exposure Assessment. (EPA/100/B-19/001). Washington, D.C.: Risk Assessment Forum, U.S. EPA. Page | ii TABLE OF CONTENTS DISCLAIMER ..................................................................................................................................... ii LIST OF TABLES.............................................................................................................................. vii LIST OF FIGURES ........................................................................................................................... viii LIST OF BOXES ................................................................................................................................ ix ABBREVIATIONS AND ACRONYMS .............................................................................................. x PREFACE ........................................................................................................................................... xi AUTHORS, CONTRIBUTORS AND -
Operational Risk Management Guide
OPERATIONAL RISK MANAGEMENT GUIDE U.S. DEPARTMENT OF AGRICULTURE FOREST SERVICE 2020 Last Updated 02/26/2020 RISK MANAGEMENT COUNCIL IN COOPERATION WITH THE OFFICE OF SAFETY & OCCUPATIONAL HEALTH and THE NATIONAL AVIATION SAFETY COUNCIL Contents Contents ....................................................................................................................................................................................... 2 Executive Summary .................................................................................................................................................................. i Introduction ............................................................................................................................................................................... 1 What is Operational Risk Management? ................................................................................................................... 1 The Terminology of ORM ................................................................................................................................................ 1 Principles of ORM Application ........................................................................................................................................... 6 The Five-Step ORM Process ................................................................................................................................................ 7 Step 1: Identify Hazards .................................................................................................................................................. -

Safety Manual
Eastern Elevator Safety and Health Manual January 2017 Page 1 of 125 SAFETY AND HEALTH MANUAL Index by Section Number Safety Policy ................................................................................................................. …4 Section 1: General Health and Safety Policies ............................................................. …5 Section 2: Hazard Communication ................................................................................ ..13 Section 3: Personal Protective Equipment (PPE) ......................................................... ..18 Section 4: Emergency Action Plan ................................................................................ ..31 Section 5: Fall Protection .............................................................................................. ..34 Section 6: Ladder Safety ............................................................................................... ..38 Section 7: Bloodborne Pathogens ................................................................................ ..42 Section 8: Motor Vehicle / Fleet Safety ......................................................................... ..47 Section 9: Hearing Conservation .................................................................................. ..50 Section 10: Lockout / Tagout ........................................................................................ ..53 Section 11: Fire Prevention .......................................................................................... -

A PRACTICAL GUIDE for USE of REAL TIME DETECTION SYSTEMS for WORKER PROTECTION and COMPLIANCE with OCCUPATIONAL EXPOSURE LIMITS May 2019
A PRACTICAL GUIDE FOR USE OF REAL TIME DETECTION SYSTEMS FOR WORKER PROTECTION AND COMPLIANCE WITH OCCUPATIONAL EXPOSURE LIMITS May 2019 WHITE PAPER May 2019 A PRACTICAL GUIDE FOR USE OF REAL TIME DETECTION SYSTEMS FOR WORKER PROTECTION AND COMPLIANCE WITH OCCUPATIONAL EXPOSURE LIMITS Prepared by: Energy Facility Contractor’s Group (EFCOG) Industrial Hygiene and Safety Task Group and Members of the American Industrial Hygiene Association (AIHA) Exposure Assessment Strategies Group Dina Siegel1, David Abrams 2, John Hill3, Steven Jahn2, Phil Smith2, Kayla Thomas4 1 Los Alamos National Laboratory 2 AIHA Exposure Assessment Strategies Committee 3 Savannah River Site 4 Kansas City National Security Campus A PRACTICAL GUIDE FOR USE OF REAL TIME DETECTION SYSTEMS FOR WORKER PROTECTION AND COMPLIANCE WITH OCCUPATIONAL EXPOSURE LIMITS May 2019 Table of Contents 1.0 Executive Summary 2.0 Introduction 3.0 Discussion 3.1 Occupational Exposure Assessment 3.2 Regulatory Compliance 3.3 Occupational Exposure Limits 3.4 Traditional Use of Real Time Detection Systems 3.5 Use and Limitations of Real Time Detection Systems 3.6 Use of Real Time Detection Systems for Compliance 3.7 Documentation/Reporting of Real Time Detection Systems Results 3.8 Peak Exposures Data Interpretations 3.9 Conclusions 4.0 Matrices 5.0 References 6.0 Attachments Page | 2 A PRACTICAL GUIDE FOR USE OF REAL TIME DETECTION SYSTEMS FOR WORKER PROTECTION AND COMPLIANCE WITH OCCUPATIONAL EXPOSURE LIMITS May 2019 1.0 Executive Summary This white paper presents practical guidance for field industrial hygiene personnel in the use and application of real time detection systems (RTDS) for exposure monitoring. -

Supplementary File 2: Assessment of Quality and Bias
Supplementary File 2: Assessment of quality and bias In preparing the tool, it was not possible to identify a dominant factor for which studies should be controlled for, instead recognising several key variables. Comparability was therefore scored against a single criterion of ‘effectively controlling for relevant factors’, meaning a maximum of eight points, rather than nine, were available. Where a nested cohort or matched case group was identified within an interventional study, it was agreed that the quality of the study as applied to impact of ETS would be appraised, and not the main interventional study outcomes. This acknowledged that high quality trials not relevant to the impact of ETS exposure could contain poor quality cohorts that were appropriate for inclusion, or vice versa. A point was awarded for satisfactory response on each question, indicated by a tick in the relevant table. Cohort Outcome Measures Domain and outcomes Point Representativeness of the exposed cohort A Truly representative of the paediatric population undergoing surgery B Somewhat representative of the paediatric population undergoing surgery C Selected subgroup of the population undergoing surgery D No description of the cohort selection process Selection of the non-exposed cohort A Drawn from the same community as the exposed cohort B Drawn from a different source C No description of the derivation of the non-exposed cohort Ascertainment of exposure A Secure record (e.g. surgical record, biological test) B Structured interview C Written self-report of self-completed questionnaire D No description Demonstration that outcome of interest was not present at start of the study A Yes B No Comparability of cohorts on the basis of the design or analysis A Study controls for reasonable factors (e.g. -
Exposure Assessment Concepts
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site. Copyright 2006, The Johns Hopkins University, Patrick Breysse, and Peter S. J. Lees. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed. Exposure Assessment Concepts Patrick N. Breysse, PhD, CIH Peter S.J. Lees, PhD, CIH Johns Hopkins University Section A Introduction Origin of Hygiene Hygeia was the Greek goddess of health Rene Dubos wrote: “For the worshippers of Hygeia, health is … a positive attribute to which men are entitled if they govern their lives wisely” Prevention is key 4 Exposure—Definition Contact between the outer boundary of the human body (skin, nose, lungs, GI tract) and a contaminant Requires the simultaneous presence of a contaminant and the contact between the person and that medium Quantified by concentration of contaminant and time and frequency of contact 5 Route of Exposure Inhalation Ingestion Dermal Direct injection Inhalation is most common in workplace—but not in general environment Moving towards concept of total exposure 6 Exposure Assessment Magnitude – Concentration in media (ppm, f/cc) Duration – Minutes, hours, days, working life, lifetime Frequency – Daily, weekly, seasonally 7 Types of Air Sampling: Time Source: U.S. -

Community Exposure Assessment (Excluding Health
(excluding health Community Exposure Assessment care providers) Physical distance >2 Duration of interaction1 Ventilation3 Source control and PPE Risk assessment metres maintained2 Case and contact are both wearing masks (cloth or medical); OR Case is wearing both a mask (cloth or Low risk medical) and a face shield4 regardless of PPE worn by (self-monitor)5 <15 minutes (except No Regardless of contact; OR Contact is wearing both a mask and eye for very brief ventilation protection regardless of PPE worn by case interactions such as High risk passing by someone) Either case or contact is not wearing a mask (self-isolate)6 Regardless of Low risk Yes Regardless of PPE worn by either case or contact ventilation (self-monitor) Case and contact are both wearing masks (cloth or medical); OR Case is wearing both a mask (cloth or Low risk medical) and a face shield regardless of PPE worn (self-monitor) Well by contact; OR Contact is wearing both a mask and ventilated eye protection regardless of PPE worn by case No High risk Either case or contact is not wearing a mask (self-isolate) Poorly High risk Regardless of PPE worn by either case or contact ventilated (self-isolate) 15 minutes – 1 hour Well Low risk Regardless of PPE worn by either case or contact ventilated (self-monitor) Case and contact are both wearing masks (cloth or medical); OR Case is wearing both a mask (cloth or Low risk Yes medical) and a face shield regardless of PPE worn (self-monitor) Poorly by contact; OR Contact is wearing both a mask and ventilated eye protection regardless of PPE worn by case High risk Either case or contact is not wearing a mask (self-isolate) COVID-19 Info-Line 905-688-8248 press 7 Toll-free: 1-888-505-6074 niagararegion.ca/COVID19 Created December 2020. -

VHA Dir 7702, Industrial Hygiene Exposure Assessment Program
Department of Veterans Affairs VHA DIRECTIVE 7702 Veterans Health Administration Transmittal Sheet Washington, DC 20420 April 29, 2016 INDUSTRIAL HYGIENE EXPOSURE ASSESSMENT PROGRAM 1. REASON FOR ISSUE: The Veterans Health Administration (VHA) has developed this program to meet Occupational Safety and Health (OSH) requirements established by VA Directive 7700, Occupational Safety and Health. This Directive specifies actions and expected performance criteria for Industrial Hygiene programs. 2. SUMMARY OF CONTENTS: Hazardous exposures adversely impact VHA staff, patients, and visitors. This Directive establishes VHA policy for implementing the Industrial Hygiene Exposure Assessment Program. The Program establishes the responsibilities and procedures for preventing adverse health effects from occupational exposures, ensures compliance with laws and regulations mandating a safe and healthful working environment, and provides a comprehensive approach for prioritizing and managing occupational exposure risks. The systemic approach described in this Directive will allow designated staff to anticipate, recognize, evaluate, and control occupational exposure hazards present in VHA facilities. 3. RELATED ISSUES: VA Directive 7700 and VHA Directive 7701. 4. RESPONSIBLE OFFICE: The Director, Office of Occupational Safety Health and Green Environmental Management (GEMS) Programs (10NA8) is responsible for the contents of this Directive. Questions may be referred to 202-632-7889. 5. RESCISSIONS: None. 6. RECERTIFICATION: This VHA Directive is due to be recertified on or before the last working day of April 2021. David J. Shulkin, M.D. Under Secretary for Health DISTRIBUTION: Emailed to the VHA Publication Distribution List on 5/3/2016. T-1 April 29, 2016 VHA DIRECTIVE 7702 INDUSTRIAL HYGIENE EXPOSURE ASSESSMENT PROGRAM 1. PURPOSE This Veterans Health Administration (VHA) Directive provides VHA policy for implementing the elements of the Industrial Hygiene (IH) program. -

Assigning Risk Assessment Codes
Exhibit 1 240 FW 5 Page 1 of 4 Assigning Risk Assessment Codes The Department of the Interior describes its Risk Assessment System in 485 DM 6, Inspections and Abatements. The policy mandates inspections, assignment of Risk Assessment Codes (RACs) to identified hazards, and abatement of the hazards within certain timeframes. The RACs are based on the hazard severity, probability of occurrence, and number of people exposed or potentially lost in the event of an accident. While all hazards should be resolved as soon as possible, the Risk Assessment System provides managers with safety risk ranking information to assist them in making informed decisions concerning hazard control. It also provides decisionmakers with a consistent and defensible approach to prioritizing safety hazard abatement efforts among the many competing resource demands and priorities. Step 1 – Learn the terminology Hazard – Anything that may cause harm, injury, or ill health. Risk – Risk is a measure of both the likelihood (probability) and the consequence (severity) of all hazards related to an activity or condition. Risk Assessment System (RAS) – A method provided by the Department to assist managers to prioritize safety and health deficiencies. Risk Assessment Code (RAC) – A hazard number ranking system from 1 (the highest level of risk) to 5 (the lowest level of risk). Risk Assessment Matrix – A tool used to assign RACs (see example below). XX/XX/13 OCCUPATIONAL SAFETY AND HEALTH Exhibit 1 240 FW 5 Page 2 of 4 Step 2 – Using the RAC Matrix Tool, assigning a code Evaluate each deficiency based on both the likelihood (probability) of an outcome occurring and the consequence (severity) of a potential outcome. -

Environmental Compliance (Ec)
LANL Waste Characterization, Reduction, and Repackaging Facility DOE ORR 7/21 OCCUPATIONAL AND INDUSTRIAL SAFETY AND HYGIENE PROGRAM (OSH) OBJECTIVE OSH.1: LANS has established and implemented Occupational and Industrial Safety and Hygiene (OISH) programs to ensure safe accomplishment of work at WCRR. Sufficient numbers of qualified personnel as well as adequate facilities and equipment are available to support WCRRF operations. (CRs 1, 4, 6, and 7) CRITERIA 1. The IH Program has conducted current and comprehensive exposure assessments. An adequate monitoring program is in place including equipment. (Exposure to radioactive contamination will be evaluated in the Radiological Protection Functional Area). (TSR; 10 CFR 851, CRD 18) 2. The Occupational Safety program has incorporated hazards and appropriate controls for the WCRR work activities such as ladder safety, electrical, Lockout/Tagout, hotwork, and vehicular safety. (TSR; 10 CFR 851) 3. Hoisting and rigging program complies with TSR requirements concerning spotters (TSR 5.6.10) and engineered lifts (5.10.3). Forklift management and operational procedures comply with TSR controls. (TSR; 10 CFR 851) 4. Adequate numbers of Industrial Hygiene and Occupational Safety professionals are assigned and perform effectively (work place surveillances, work package reviews, walk-down, etc). 5. Adequate facilities are available to ensure WCRRF operational support in the area of occupational and industrial safety. 6. The level of knowledge of occupational and industrial safety personnel concerning their roles and responsibilities for WCRR operations is adequate. (DOE O 440.1A, DOE O 5480.20A) APPROACH Requirement: • 10 CFR 851, Worker Safety and Health Program Document Review: • Review Contractor Management Self Assessment Report (MSA), and Contractor Operational Readiness Review (CORR) Report and corrective actions for all findings to determine if: – All Pre-Start Findings are resolved and the corrective actions are appropriate for the issue determined. -

Incidence of Laryngospasm and Bronchospasm in Pediatric Adenotonsillectomy
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln US Army Research U.S. Department of Defense 2012 Incidence of Laryngospasm and Bronchospasm in Pediatric Adenotonsillectomy Michael I. Orestes Walter Reed Army Medical Center Lina Lander University of Nebraska Medical Center, [email protected] Susan Verghese Children’s National Medical Center Rahul K. Shah Children’s National Medical Center, [email protected] Follow this and additional works at: https://digitalcommons.unl.edu/usarmyresearch Orestes, Michael I.; Lander, Lina; Verghese, Susan; and Shah, Rahul K., "Incidence of Laryngospasm and Bronchospasm in Pediatric Adenotonsillectomy" (2012). US Army Research. 257. https://digitalcommons.unl.edu/usarmyresearch/257 This Article is brought to you for free and open access by the U.S. Department of Defense at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in US Army Research by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. The Laryngoscope VC 2012 The American Laryngological, Rhinological and Otological Society, Inc. Incidence of Laryngospasm and Bronchospasm in Pediatric Adenotonsillectomy Michael I. Orestes, MD; Lina Lander, ScD; Susan Verghese, MD; Rahul K. Shah, MD Objectives/Hypothesis: To evaluate and describe airway complications in pediatric adenotonsillectomy. Study Design: Retrospective case-control study. Methods: A chart review of patients that underwent adenotonsillectomy between 2006 and 2010 was performed. Peri- operative complications, patient characteristics, and surgeon and anesthesia technique were recorded. Results: A total of 682 charts were reviewed. Eleven cases (1.6%) of laryngospasm were identified: one was preopera- tive, seven occurred in the operating room postextubation, and three occurred in the recovery area. Four patients were given succinylcholine, one was reintubated, and the other cases were managed conservatively.