VHA Dir 7702, Industrial Hygiene Exposure Assessment Program
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
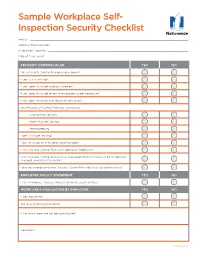
Sample Workplace Self- Inspection Security Checklist
Sample Workplace Self- Inspection Security Checklist Facility: ������������������������������������������������������������������������������������������������������������������������� Address/Work Location: �������������������������������������������������������������������������������������������������������� Assessment Done By: ����������������������������������������������������������������������������������������������������������� Date of Assessment: ������������������������������������������������������������������������������������������������������������ SECURITY CONTROL PLAN YES NO Has a Security Control Plan been developed? If yes, is it in writing? If yes, does it include a policy statement? If yes, does it include review of employee incident exposure? If yes, does it include evaluation of work areas? Identification of Control Methods considered: Engineering Controls Work Practice Controls Recordkeeping Does it include training? Does it include an evacuation and floor plan? Is the Security Control Plan accessible to all employees? Is the Security Control Plan reviews and updated when a task has been added or changed, and at least annually? Have you coordinated your Security Control Plan with local law enforcement? EMPLOYER POLICY STATEMENT YES NO Is the Workplace Violence Policy statement clearly written? WORK AREA EVALUATION BY EMPLOYER YES NO If yes, how often? Are all areas being evaluated? If no, which areas are not being evaluated? Comments: Continued >> Loss Control Services Workplace Security Checklist CONTROL MEASURES -

Guidelines for Human Exposure Assessment Risk Assessment Forum
EPA/100/B-19/001 October 2019 www.epa.gov/risk Guidelines for Human Exposure Assessment Risk Assessment Forum EPA/100/B-19/001 October 2019 Guidelines for Human Exposure Assessment Risk Assessment Forum U.S. Environmental Protection Agency DISCLAIMER This document has been reviewed in accordance with U.S. Environmental Protection Agency (EPA) policy. Mention of trade names or commercial products does not constitute endorsement or recommendation for use. Preferred citation: U.S. EPA (U.S. Environmental Protection Agency). (2019). Guidelines for Human Exposure Assessment. (EPA/100/B-19/001). Washington, D.C.: Risk Assessment Forum, U.S. EPA. Page | ii TABLE OF CONTENTS DISCLAIMER ..................................................................................................................................... ii LIST OF TABLES.............................................................................................................................. vii LIST OF FIGURES ........................................................................................................................... viii LIST OF BOXES ................................................................................................................................ ix ABBREVIATIONS AND ACRONYMS .............................................................................................. x PREFACE ........................................................................................................................................... xi AUTHORS, CONTRIBUTORS AND -
Personal Protective Equipment (PPE) Guide
Personal Protective Equipment (PPE) Guide Volume 1: General PPE February 2003 F417-207-000 This guide is designed to be used by supervisors, lead workers, managers, employers, and anyone responsible for the safety and health of employees. Employees are also encouraged to use information in this guide to analyze their own jobs, be aware of work place hazards, and take active responsibility for their own safety. Photos and graphic illustrations contained within this document were provided courtesy of the Occupational Safety and Health Administration (OSHA), Oregon OSHA, United States Coast Guard, EnviroWin Safety, Microsoft Clip Gallery (Online), and the Washington State Department of Labor and Industries. TABLE OF CONTENTS (If viewing this pdf document on the computer, you can place the cursor over the section headings below until a hand appears and then click. You can also use the Adobe Acrobat Navigation Pane to jump directly to the sections.) How To Use This Guide.......................................................................................... 4 A. Introduction.........................................................................................6 B. What you are required to do ..............................................................8 1. Do a Hazard Assessment for PPE and document it ........................................... 8 2. Select and provide appropriate PPE to your employees................................... 10 3. Provide training to your employees and document it ........................................ 11 -
7. Tasks/Procedures 8. Hazards 9. Abatement
FS-6700-7 (11/99) 1. WORK PROJECT/ 2. LOCATION 3. UNIT(S) U.S. Department of Agriculture ACTIVITY Coconino National Forest All Districts Forest Service Trail Maintenance JOB HAZARD ANALYSIS (JHA) 4. NAME OF ANALYST 5. JOB TITLE 6. DATE PREPARED References-FSH 6709.11 and 12 Amy Racki Partnership Coordinator 10/28/2013 9. ABATEMENT ACTIONS 7. TASKS/PROCEDURES 8. HAZARDS Engineering Controls * Substitution * Administrative Controls * PPE Personal Protective Equipment Wear helmet, work gloves, boots with slip-resistant heels and soles with firm, flexible support, eye protection, long sleeve shirts, long pants, hearing protection where appropriate Carry first aid kit Vehicle Operation Fatigue Drive defensively and slow. Watch for animals Narrow, rough roads Always wear seatbelts and turn lights on Poor visibility Mechanical failure Ensure that you have reliable communication Vehicle Accients Obey speed limits Weather Keep vehicles maintained. Keep windows and windshield clean Animals on Road Anticipate careless actions by other drivers Use spotter when backing up Stay clear of gullies and trenches, drive slowly over rocks. Carry and use chock blocks, use parking brake, and do not leave vehicle while it is running Inform someone of your destination and estimated time of return, call in if plans change Carry extra food, water, and clothing Stop and rest if fatigued Hiking on the Trail Dehydration Drink 12-15 quarts of water per day, increase fluid on hotter days or during extremely strenuous activity Contaminated water Drink -
Controlling Hazardous Energy: De-Energization and Lockout Iii Trapped-Key Interlock Systems
Controlling Hazardous Energy De-Energization and Lockout About WorkSafeBC At WorkSafeBC, we’re dedicated to promoting safe and healthy workplaces across B.C. We partner with workers and employers to save lives and prevent injury, disease, and disability. When work-related injuries or diseases occur, we provide compensation and support injured workers in their recovery, rehabilitation, and safe return to work. We also provide no-fault insurance and work diligently to sustain our workers’ compensation system for today and future generations. We’re honoured to serve the workers and employers in our province. Prevention Information Line We provide information and assistance with health and safety issues in the workplace. Call the information line 24 hours a day, 7 days a week to report unsafe working conditions, a serious incident, or a major chemical release. Your call can be made anonymously. We can provide assistance in almost any language. If you have questions about workplace health and safety or the Occupational Health and Safety Regulation, call during our office hours (8:05 a.m. to 4:30 p.m.) to speak to a WorkSafeBC officer. If you’re in the Lower Mainland, call 604.276.3100. Elsewhere in Canada, call toll-free at 1.888.621.7233 (621.SAFE). Health and safety resources You can find our health and safety resources on worksafebc.com, and many of them can be ordered from the WorkSafeBC Store at worksafebcstore.com. In addition to books, you’ll find other types of resources at the WorkSafeBC Store, including DVDs, posters, and brochures. If you have any questions about placing an order online, please contact a customer service representative at 604.232.9704 or toll-free at 1.866.319.9704. -

Safety Manual
Eastern Elevator Safety and Health Manual January 2017 Page 1 of 125 SAFETY AND HEALTH MANUAL Index by Section Number Safety Policy ................................................................................................................. …4 Section 1: General Health and Safety Policies ............................................................. …5 Section 2: Hazard Communication ................................................................................ ..13 Section 3: Personal Protective Equipment (PPE) ......................................................... ..18 Section 4: Emergency Action Plan ................................................................................ ..31 Section 5: Fall Protection .............................................................................................. ..34 Section 6: Ladder Safety ............................................................................................... ..38 Section 7: Bloodborne Pathogens ................................................................................ ..42 Section 8: Motor Vehicle / Fleet Safety ......................................................................... ..47 Section 9: Hearing Conservation .................................................................................. ..50 Section 10: Lockout / Tagout ........................................................................................ ..53 Section 11: Fire Prevention .......................................................................................... -

A PRACTICAL GUIDE for USE of REAL TIME DETECTION SYSTEMS for WORKER PROTECTION and COMPLIANCE with OCCUPATIONAL EXPOSURE LIMITS May 2019
A PRACTICAL GUIDE FOR USE OF REAL TIME DETECTION SYSTEMS FOR WORKER PROTECTION AND COMPLIANCE WITH OCCUPATIONAL EXPOSURE LIMITS May 2019 WHITE PAPER May 2019 A PRACTICAL GUIDE FOR USE OF REAL TIME DETECTION SYSTEMS FOR WORKER PROTECTION AND COMPLIANCE WITH OCCUPATIONAL EXPOSURE LIMITS Prepared by: Energy Facility Contractor’s Group (EFCOG) Industrial Hygiene and Safety Task Group and Members of the American Industrial Hygiene Association (AIHA) Exposure Assessment Strategies Group Dina Siegel1, David Abrams 2, John Hill3, Steven Jahn2, Phil Smith2, Kayla Thomas4 1 Los Alamos National Laboratory 2 AIHA Exposure Assessment Strategies Committee 3 Savannah River Site 4 Kansas City National Security Campus A PRACTICAL GUIDE FOR USE OF REAL TIME DETECTION SYSTEMS FOR WORKER PROTECTION AND COMPLIANCE WITH OCCUPATIONAL EXPOSURE LIMITS May 2019 Table of Contents 1.0 Executive Summary 2.0 Introduction 3.0 Discussion 3.1 Occupational Exposure Assessment 3.2 Regulatory Compliance 3.3 Occupational Exposure Limits 3.4 Traditional Use of Real Time Detection Systems 3.5 Use and Limitations of Real Time Detection Systems 3.6 Use of Real Time Detection Systems for Compliance 3.7 Documentation/Reporting of Real Time Detection Systems Results 3.8 Peak Exposures Data Interpretations 3.9 Conclusions 4.0 Matrices 5.0 References 6.0 Attachments Page | 2 A PRACTICAL GUIDE FOR USE OF REAL TIME DETECTION SYSTEMS FOR WORKER PROTECTION AND COMPLIANCE WITH OCCUPATIONAL EXPOSURE LIMITS May 2019 1.0 Executive Summary This white paper presents practical guidance for field industrial hygiene personnel in the use and application of real time detection systems (RTDS) for exposure monitoring. -

Supplementary File 2: Assessment of Quality and Bias
Supplementary File 2: Assessment of quality and bias In preparing the tool, it was not possible to identify a dominant factor for which studies should be controlled for, instead recognising several key variables. Comparability was therefore scored against a single criterion of ‘effectively controlling for relevant factors’, meaning a maximum of eight points, rather than nine, were available. Where a nested cohort or matched case group was identified within an interventional study, it was agreed that the quality of the study as applied to impact of ETS would be appraised, and not the main interventional study outcomes. This acknowledged that high quality trials not relevant to the impact of ETS exposure could contain poor quality cohorts that were appropriate for inclusion, or vice versa. A point was awarded for satisfactory response on each question, indicated by a tick in the relevant table. Cohort Outcome Measures Domain and outcomes Point Representativeness of the exposed cohort A Truly representative of the paediatric population undergoing surgery B Somewhat representative of the paediatric population undergoing surgery C Selected subgroup of the population undergoing surgery D No description of the cohort selection process Selection of the non-exposed cohort A Drawn from the same community as the exposed cohort B Drawn from a different source C No description of the derivation of the non-exposed cohort Ascertainment of exposure A Secure record (e.g. surgical record, biological test) B Structured interview C Written self-report of self-completed questionnaire D No description Demonstration that outcome of interest was not present at start of the study A Yes B No Comparability of cohorts on the basis of the design or analysis A Study controls for reasonable factors (e.g. -
![NIOSH [2015]. Best Practices: Engineering Controls, Work Practices and Exposure Monitor- Ing for Occupational Exposures to Diacetyl and 2,3-Pentanedione](https://docslib.b-cdn.net/cover/1780/niosh-2015-best-practices-engineering-controls-work-practices-and-exposure-monitor-ing-for-occupational-exposures-to-diacetyl-and-%C2%AD2-3-pentanedione-751780.webp)
NIOSH [2015]. Best Practices: Engineering Controls, Work Practices and Exposure Monitor- Ing for Occupational Exposures to Diacetyl and 2,3-Pentanedione
BEST PRACTICES Engineering Controls, Work Practices, and Exposure Monitoring for Occupational Exposures to Diacetyl and 2,3-Pentanedione DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Institute for Occupational Safety and Health BEST PRACTICES Engineering Controls, Work Practices, and Exposure Monitoring for Occupational Exposures to Diacetyl and 2,3-Pentanedione By Kevin H. Dunn, Lauralynn Taylor McKernan, and Alberto Garcia DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Institute for Occupational Safety and Health This document is in the public domain and may be freely copied or reprinted. DISCLAIMER Mention of any company or product does not constitute endorsement by the National Insti- tute for Occupational Safety and Health (NIOSH). In addition, citations to websites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their pro- grams or products. Furthermore, NIOSH is not responsible for the content of these websites. All Web addresses referenced in this document were accessible as of the publication date. ORDERING INFORMATION To receive documents or other information about occupational safety and health topics, contact NIOSH: Telephone: 1-800-CDC-INFO (1-800-232-4636) TTY: 1-888-232-6348 CDC INFO: www.cdc.gov/info or visit the NIOSH website at www.cdc.gov/niosh. For a monthly update on news at NIOSH, subscribe to NIOSH eNews by visiting www.cdc.gov/niosh/eNews. SUGGESTED CITATION NIOSH [2015]. Best practices: engineering controls, work practices and exposure monitor- ing for occupational exposures to diacetyl and 2,3-pentanedione. By Dunn KH, McKernan LT, Garcia A. -
Exposure Assessment Concepts
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site. Copyright 2006, The Johns Hopkins University, Patrick Breysse, and Peter S. J. Lees. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed. Exposure Assessment Concepts Patrick N. Breysse, PhD, CIH Peter S.J. Lees, PhD, CIH Johns Hopkins University Section A Introduction Origin of Hygiene Hygeia was the Greek goddess of health Rene Dubos wrote: “For the worshippers of Hygeia, health is … a positive attribute to which men are entitled if they govern their lives wisely” Prevention is key 4 Exposure—Definition Contact between the outer boundary of the human body (skin, nose, lungs, GI tract) and a contaminant Requires the simultaneous presence of a contaminant and the contact between the person and that medium Quantified by concentration of contaminant and time and frequency of contact 5 Route of Exposure Inhalation Ingestion Dermal Direct injection Inhalation is most common in workplace—but not in general environment Moving towards concept of total exposure 6 Exposure Assessment Magnitude – Concentration in media (ppm, f/cc) Duration – Minutes, hours, days, working life, lifetime Frequency – Daily, weekly, seasonally 7 Types of Air Sampling: Time Source: U.S. -

Community Exposure Assessment (Excluding Health
(excluding health Community Exposure Assessment care providers) Physical distance >2 Duration of interaction1 Ventilation3 Source control and PPE Risk assessment metres maintained2 Case and contact are both wearing masks (cloth or medical); OR Case is wearing both a mask (cloth or Low risk medical) and a face shield4 regardless of PPE worn by (self-monitor)5 <15 minutes (except No Regardless of contact; OR Contact is wearing both a mask and eye for very brief ventilation protection regardless of PPE worn by case interactions such as High risk passing by someone) Either case or contact is not wearing a mask (self-isolate)6 Regardless of Low risk Yes Regardless of PPE worn by either case or contact ventilation (self-monitor) Case and contact are both wearing masks (cloth or medical); OR Case is wearing both a mask (cloth or Low risk medical) and a face shield regardless of PPE worn (self-monitor) Well by contact; OR Contact is wearing both a mask and ventilated eye protection regardless of PPE worn by case No High risk Either case or contact is not wearing a mask (self-isolate) Poorly High risk Regardless of PPE worn by either case or contact ventilated (self-isolate) 15 minutes – 1 hour Well Low risk Regardless of PPE worn by either case or contact ventilated (self-monitor) Case and contact are both wearing masks (cloth or medical); OR Case is wearing both a mask (cloth or Low risk Yes medical) and a face shield regardless of PPE worn (self-monitor) Poorly by contact; OR Contact is wearing both a mask and ventilated eye protection regardless of PPE worn by case High risk Either case or contact is not wearing a mask (self-isolate) COVID-19 Info-Line 905-688-8248 press 7 Toll-free: 1-888-505-6074 niagararegion.ca/COVID19 Created December 2020. -

Controlling Chemical Exposure Industrial Hygiene Fact Sheets
Controlling Chemical Exposure Industrial Hygiene Fact Sheets Concise guidance on 16 components of industrial hygiene controls New Jersey Department of Health and Senior Services Division of Epidemiology, Environmental and Occupational Health Occupational Health Service PO Box 360 Trenton, NJ 08625-0360 609-984-1863 October 2000 James E. McGreevey Clifton R. Lacy, M.D. Governor Commissioner Written by: Eileen Senn, MS, CIH Occupational Health Surveillance Program James S. Blumenstock Senior Assistant Commissioner Public Health Protection and Prevention Programs Eddy Bresnitz, MD, MS State Epidemiologist/Assistant Commissioner Division of Epidemiology, Environmental and Occupational Health Kathleen O’Leary, MS Director Occupational Health Service David Valiante, MS, CIH Acting Program Manager Occupational Health Surveillance Program Funding: This project was supported in part by a cooperative agreement from the U.S. Department of Health and Human Services, National Institute for Occupational Safety and Health (NIOSH). Reproduction: The NJDHSS encourages the copying and distribution of all or parts of this booklet. All materials are in the public domain and may be reproduced or copied without permission. Cita- tion as to the source is appreciated. This document is available on the Internet at: www.state.nj.us/health/eoh/survweb/ihfs.pdf Citation: Senn, E., Controlling Chemical Exposure; Industrial Hygiene Fact Sheets, Trenton, NJ: New Jersey Department of Health and Senior Services, October 2000. Table of Contents Methods for Controlling