And an Imatinib-Responsive Myeloproliferative Disorder1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Paxillin Binding to the Cytoplasmic Domain of CD103 Promotes Cell Adhesion and Effector
Author Manuscript Published OnlineFirst on October 11, 2017; DOI: 10.1158/0008-5472.CAN-17-1487 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Paxillin binding to the cytoplasmic domain of CD103 promotes cell adhesion and effector functions for CD8+ resident memory T cells in tumors Ludiane Gauthier1, Stéphanie Corgnac1, Marie Boutet1, Gwendoline Gros1, Pierre Validire2, Georges Bismuth3 and Fathia Mami-Chouaib1 1 INSERM UMR 1186, Integrative Tumor Immunology and Genetic Oncology, Gustave Roussy, EPHE, Fac. de médecine - Univ. Paris-Sud, Université Paris-Saclay, 94805, Villejuif, France 2 Institut Mutualiste Montsouris, Service d’Anatomie pathologique, 75014 Paris, France. 3 INSERM U1016, CNRS UMR8104, Université Paris Descartes, Institut Cochin, 75014 Paris. S Corgnac, M Boutet and G Gros contributed equally to this work. M Boutet current address: Department of Microbiology and Immunology Albert Einstein College of Medecine, NY 10461 USA. Corresponding author: Fathia Mami-Chouaib, INSERM UMR 1186, Gustave Roussy. 39, rue Camille Desmoulins, F-94805 Villejuif. Phone: +33 1 42 11 49 65, Fax: +33 1 42 11 52 88, e-mail: [email protected] and [email protected] Running title: CD103 signaling in human TRM cells Key words: TRM cells, CD103 integrin, T-cell function and signaling, paxillin. Abbreviations: IS: immune synapse; LFA: leukocyte function-associated antigen; FI: fluorescence intensity; mAb: monoclonal antibody; phospho: phosphorylated; Pyk2: proline- rich tyrosine kinase-2; NSCLC: non-small-cell lung carcinoma; r: recombinant; sh-pxn: shorthairpin RNA-paxillin; TCR: T-cell receptor; TIL: tumor-infiltrating lymphocyte; TRM: tissue-resident memory T. -

Paxillin: a Focal Adhesion-Associated Adaptor Protein
Oncogene (2001) 20, 6459 ± 6472 ã 2001 Nature Publishing Group All rights reserved 0950 ± 9232/01 $15.00 www.nature.com/onc Paxillin: a focal adhesion-associated adaptor protein Michael D Schaller*,1 1Department of Cell and Developmental Biology, Lineberger Comprehensive Cancer Center and Comprehensive Center for In¯ammatory Disorders, University of North Carolina, Chapel Hill, North Carolina, NC 27599, USA Paxillin is a focal adhesion-associated, phosphotyrosine- The molecular cloning of paxillin revealed a number containing protein that may play a role in several of motifs that are now known to function in mediating signaling pathways. Paxillin contains a number of motifs protein ± protein interactions (see Figure 1) (Turner that mediate protein ± protein interactions, including LD and Miller, 1994; Salgia et al., 1995a). The N-terminal motifs, LIM domains, an SH3 domain-binding site and half of paxillin contains a proline-rich region that SH2 domain-binding sites. These motifs serve as docking could serve as an SH3 domain-binding site. Several sites for cytoskeletal proteins, tyrosine kinases, serine/ tyrosine residues conforming to SH2 domain binding threonine kinases, GTPase activating proteins and other sites were also noted. In addition, the N-terminal adaptor proteins that recruit additional enzymes into domain of paxillin contains ®ve copies of a peptide complex with paxillin. Thus paxillin itself serves as a sequence, called the LD motif, which are now known docking protein to recruit signaling molecules to a to function as binding sites for other proteins (see speci®c cellular compartment, the focal adhesions, and/ Table 1) (Brown et al., 1998a). The C-terminal half of or to recruit speci®c combinations of signaling molecules paxillin is comprised of four LIM domains, which are into a complex to coordinate downstream signaling. -

Download PDF to Print
MOLECULAR INSIGHTS IN PATIENT CARE A Cryptic BCR-PDGFRB Fusion Resulting in a Chronic Myeloid Neoplasm With Monocytosis and Eosinophilia: A Novel Finding With Treatment Implications Sanjeev Kumar Gupta, MD1,*; Nitin Jain, MD1,*; Guilin Tang, MD, PhD2; Andrew Futreal, PhD3; Sa A. Wang, MD2; Joseph D. Khoury, MD2; Richard K. Yang, MD, PhD2; Hong Fang, MD2; Keyur P.Patel, MD, PhD2; Rajyalakshmi Luthra, PhD2; Mark Routbort, MD, PhD2; Bedia A. Barkoh, MS2; Wei Chen, MS2; Xizeng Mao, PhD3; Jianhua Zhang, PhD3; L. Jeffrey Medeiros, MD2; Carlos E. Bueso-Ramos, MD, PhD2; and Sanam Loghavi, MD2 Background ABSTRACT Myeloid and lymphoid neoplasms with eosinophilia and gene rearrangement constitute a distinct group RNA-seq was used to identify the partner gene and confirm the of hematologic neoplasms in the current WHO clas- BCR-PDGFRB fi presence of a fusion. Identi cation of this fusion sification for hematopoietic neoplasms.1 Included in product resulted in successful treatment and long-term remission of this myeloid neoplasm. Based on our results, we suggest that despite this category are neoplasms harboring abnormal current WHO recommendations, screening for PDGFRB rearrange- gene fusions involving PDGFRA, PDGFRB,andFGFR1 ment in cases of leukocytosis with eosinophilia and no other etiologic or PCM1-JAK2. These fusions result in constitutive explanation is necessary, even if the karyotype is normal. activation of respective tyrosine kinases that can J Natl Compr Canc Netw 2020;18(10):1300–1304 be targeted using specific kinase inhibitors. There doi: 10.6004/jnccn.2020.7573 are multiple recognized partner genes for PDGFRA, PDGFRB, FGFR1, and JAK2. PDGFRB located at chro- mosome 5q32 has .25knownfusionpartners,with ETV6 the most common.2–8 Although PDGFRA re- arrangements often can be cryptic and not readily observed on routine karyotyping studies,9,10 PDGFRB rearrangements are believed to be nearly always vis- ible on routine karyotype. -

S41467-020-18249-3.Pdf
ARTICLE https://doi.org/10.1038/s41467-020-18249-3 OPEN Pharmacologically reversible zonation-dependent endothelial cell transcriptomic changes with neurodegenerative disease associations in the aged brain Lei Zhao1,2,17, Zhongqi Li 1,2,17, Joaquim S. L. Vong2,3,17, Xinyi Chen1,2, Hei-Ming Lai1,2,4,5,6, Leo Y. C. Yan1,2, Junzhe Huang1,2, Samuel K. H. Sy1,2,7, Xiaoyu Tian 8, Yu Huang 8, Ho Yin Edwin Chan5,9, Hon-Cheong So6,8, ✉ ✉ Wai-Lung Ng 10, Yamei Tang11, Wei-Jye Lin12,13, Vincent C. T. Mok1,5,6,14,15 &HoKo 1,2,4,5,6,8,14,16 1234567890():,; The molecular signatures of cells in the brain have been revealed in unprecedented detail, yet the ageing-associated genome-wide expression changes that may contribute to neurovas- cular dysfunction in neurodegenerative diseases remain elusive. Here, we report zonation- dependent transcriptomic changes in aged mouse brain endothelial cells (ECs), which pro- minently implicate altered immune/cytokine signaling in ECs of all vascular segments, and functional changes impacting the blood–brain barrier (BBB) and glucose/energy metabolism especially in capillary ECs (capECs). An overrepresentation of Alzheimer disease (AD) GWAS genes is evident among the human orthologs of the differentially expressed genes of aged capECs, while comparative analysis revealed a subset of concordantly downregulated, functionally important genes in human AD brains. Treatment with exenatide, a glucagon-like peptide-1 receptor agonist, strongly reverses aged mouse brain EC transcriptomic changes and BBB leakage, with associated attenuation of microglial priming. We thus revealed tran- scriptomic alterations underlying brain EC ageing that are complex yet pharmacologically reversible. -

Real-Time Quantification of BCR-ABL Mrna Transcripts Using the Lightcycler-T(9;22) Quantification Kit
real-time-quantification 09.05.2000 19:18 Uhr Seite 8 Real-time Quantification of BCR-ABL mRNA Transcripts Using the LightCycler-t(9;22) Quantification Kit Heiko Wittor 1, Hermann Leying 1, Andreas Hochhaus 2, and Rob van Miltenburg 1 1 Roche Molecular Biochemicals, Penzberg, Germany 2 III. Medizinische Universitätsklinik, Fakultät für Klinische Medizin Mannheim der Universität Heidelberg, Mannheim, Germany ly different starting concentrations, so that the initial Introduction target concentration can be determined in a single PCR. The concentration of BCR-ABL transcripts is determi- Literature indicates that in 95 % of all subjects with ned relative to the number of transcripts of a control chronic myeloid leukemia (CML) and in 25-30 % of gene, glucose-6-phosphate dehydrogenase (G6PDH). subjects with acute lymphoblastic leukemia (ALL) a The entire procedure from sample preparation to reciprocal translocation between the long arms of quantitative result is performed in 4.5 hours. chromosome 9 and chromosome 22 [t(9;22)] can be found. This translocation or the resulting fusion pro- duct can be detected by a number of techniques, CLER including fluorescent in situ hybridization, Southern CY blotting, western blotting and reverse transcriptase TThe LightCycler System polymerase chain reaction (RT-PCR). Of these techni- The LightCycler System is based on the amplification LIGHT ques, RT-PCR for the chimeric fusion transcript BCR- of target sequences using alternating heated and ABL has received most attention in relation to the ambient temperature cycles. Samples are contained in detection of minimal residual disease because of its glass capillaries with high surface-to-volume ratio, high sensitivity (1). -

Regulation of B Cell Receptor-Dependent NF-Κb Signaling by the Tumor Suppressor KLHL14
Regulation of B cell receptor-dependent NF-κB signaling by the tumor suppressor KLHL14 Jaewoo Choia, James D. Phelana, George W. Wrightb, Björn Häuplc,d,e, Da Wei Huanga, Arthur L. Shaffer IIIa, Ryan M. Younga, Zhuo Wanga, Hong Zhaoa, Xin Yua, Thomas Oellerichc,d,e, and Louis M. Staudta,1 aLymphoid Malignancies Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892; bBiometric Research Branch, Division of Cancer Diagnosis and Treatment, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892; cDepartment of Medicine II, Hematology/Oncology, Goethe University, 60590 Frankfurt, Germany; dGerman Cancer Consortium/German Cancer Research Center, 69120 Heidelberg, Germany; and eDepartment of Molecular Diagnostics and Translational Proteomics, Frankfurt Cancer Institute, 60596 Frankfurt, Germany Contributed by Louis M. Staudt, January 29, 2020 (sent for review December 4, 2019; reviewed by Shiv Pillai and Michael Reth) The KLHL14 gene acquires frequent inactivating mutations in ma- by ibrutinib, suggesting that it may be a critical target of this ture B cell malignancies, especially in the MYD88L265P, CD79B mu- drug (8). tant (MCD) genetic subtype of diffuse large B cell lymphoma Genetic analysis revealed recurrent mutations of the KLHL14 (DLBCL), which relies on B cell receptor (BCR) signaling for survival. gene in DLBCL, often in ABC tumors of the MCD genetic However, the pathogenic role of KLHL14 in DLBCL and its molec- subtype (2) and in PCNSL (6, 9). KLHL14 (also known as ular function are largely unknown. Here, we report that KLHL14 is in Printor) (10) belongs to the Kelch-like family of proteins that can close proximity to the BCR in the endoplasmic reticulum of MCD cell serve as subunits of Cullin-RING ubiquitin ligase (CRL) com- line models and promotes the turnover of immature glycoforms of plex (reviewed in ref. -
![Changing the Name of the NBPF/DUF1220 Domain to the Olduvai Domain [Version 2; Peer Review: 3 Approved]](https://docslib.b-cdn.net/cover/7813/changing-the-name-of-the-nbpf-duf1220-domain-to-the-olduvai-domain-version-2-peer-review-3-approved-767813.webp)
Changing the Name of the NBPF/DUF1220 Domain to the Olduvai Domain [Version 2; Peer Review: 3 Approved]
F1000Research 2018, 6:2185 Last updated: 31 AUG 2021 OPINION ARTICLE Changing the name of the NBPF/DUF1220 domain to the Olduvai domain [version 2; peer review: 3 approved] Previously titled: A proposal to change the name of the NBPF/DUF1220 domain to the Olduvai domain James M. Sikela 1, Frans van Roy2,3 1Department of Biochemistry and Molecular Genetics, Human Medical Genetics and Neuroscience Programs, University of Colorado School of Medicine, Aurora, CO, 80045, USA 2Department of Biomedical Molecular Biology, Ghent University, Ghent, 9052, Belgium 3VIB-UGent Center for Inflammation Research, Ghent, 9052, Belgium v2 First published: 28 Dec 2017, 6:2185 Open Peer Review https://doi.org/10.12688/f1000research.13586.1 Latest published: 17 Jul 2018, 6:2185 https://doi.org/10.12688/f1000research.13586.2 Reviewer Status Invited Reviewers Abstract We are jointly proposing a new name for a protein domain of 1 2 3 approximately 65 amino acids that has been previously termed NBPF or DUF1220. Our two labs independently reported the initial studies of version 2 this domain, which is encoded almost entirely within a single gene (revision) report report family. The name Neuroblastoma Breakpoint Family (NBPF) was 17 Jul 2018 applied to this gene family when the first identified member of the family was found to be interrupted in an individual with version 1 neuroblastoma. 28 Dec 2017 report report report Prior to this discovery, the Pfam database had termed the domain DUF1220, denoting it as one of many protein domains of unknown f unction. It has been Pfam’s intention to use “DUF” nomenclature to 1. -

The BCR Gene and Philadelphia Chromosome-Positive Leukemogenesis
[CANCER RESEARCH 61, 2343–2355, March 15, 2001] Review The BCR Gene and Philadelphia Chromosome-positive Leukemogenesis Eunice Laurent, Moshe Talpaz, Hagop Kantarjian, and Razelle Kurzrock1 Departments of Bioimmunotherapy [E. L., M. T., R. K.] and Leukemia [H. K., R. K.], University of Texas M. D. Anderson Cancer Center, Houston, Texas 77030 Introduction Recent investigations have rapidly added crucial new insights into BCR-related Genes the complex functions of the normal BCR gene and of the BCR-ABL Several BCR-related pseudogenes (BCR2, BCR3, and BCR4) have chimera and are yielding potential therapeutic breakthroughs in the also been described (34). They are not translated into proteins. All of treatment of Philadelphia (Ph) chromosome-positive leukemias. The these genes have been mapped to chromosome 22q11 by in situ term “breakpoint cluster region (bcr)” was first applied to a 5.8-kb hybridization. The orientation is such that BCR2 is the most centro- span of DNA on the long arm of chromosome 22 (22q11), which is 2 meric, followed by BCR4, then BCR1 (the functional gene) and BCR3. disrupted in patients with CML bearing the Ph translocation [t(9; BCR2 and BCR4 are retained on chromosome 22 during the t(9;22) 22)(q34;q11); Refs. 1–3]. Subsequent studies demonstrated that the translocation. The BCR-related genes all contain 3Ј sequences iden- 5.8-kb fragment resided within a central region of a gene designated tical to those encompassing the last seven exons of the BCR1 gene BCR (4). It is now well established that the breakpoint within BCR can (34, 36). -

Abnormality of C-Kit Oncoprotein in Certain Patients with Chronic
Leukemia (2002) 16, 170–177 2002 Nature Publishing Group All rights reserved 0887-6924/02 $25.00 www.nature.com/leu Abnormality of c-kit oncoprotein in certain patients with chronic myelogenous leukemia – potential clinical significance K Inokuchi, H Yamaguchi, M Tarusawa, M Futaki, H Hanawa, S Tanosaki and K Dan Division of Hematology, Department of Internal Medicine, Nippon Medical School, Tokyo, Japan Chronic myelogenous leukemia (CML) is characterized by the patients, there are two bcr/abl mRNAs for P210BCR/ABL, one Philadelphia (Ph) chromosome and bcr/abl gene rearrangement with and one without exon b3 (b3-a2 type and b2-a2 type).4 which occurs in pluripotent hematopoietic progenitor cells expressing the c-kit receptor tyrosine kinase (KIT). To elucidate In a smaller number of CML patients, there are two other types the biological properties of KIT in CML leukemogenesis, we of bcr/abl mRNAs based on the breakpoint positions of the performed analysis of alterations of the c-kit gene and func- bcr gene, ie m-bcr and -bcr for P190BCR/ABL and P230BCR/ABL, tional analysis of altered KIT proteins. Gene alterations in the respectively.5,6 Extensive studies have been performed on the c-kit juxtamembrane domain of 80 CML cases were analyzed subtypes of the bcr/abl gene and their relation to the prognosis by reverse transcriptase and polymerase chain reaction-single and clinical features.7,8 The established findings regarding the strand conformation polymorphism (RT-PCR-SSCP). One case had an abnormality at codon 564 (AAT→AAG, Asn→Lys), and influence of the subtype of the bcr/abl gene (b3-a2 or b2-a2) six cases had the same base abnormality at codon 541 on the clinical characteristics have been similar for each sub- (ATG→CTG, Met→Leu) in the juxtamembrane domain. -

A Newly Identified Myomegalin Isoform Functions in Golgi Microtubule Organization and ER–Golgi Transport
ß 2014. Published by The Company of Biologists Ltd | Journal of Cell Science (2014) 127, 4904–4917 doi:10.1242/jcs.155408 RESEARCH ARTICLE A newly identified myomegalin isoform functions in Golgi microtubule organization and ER–Golgi transport Zhe Wang, Chao Zhang and Robert Z. Qi* ABSTRACT the formation of ER–Golgi cargo carriers that associate with dynein–dynactin to move along microtubules towards the Golgi The Golgi of mammalian cells is known to be a major microtubule- (Presley et al., 1997; Scales et al., 1997; Watson et al., 2005). organizing site that requires microtubules for its organization and The Golgi serves as a major microtubule-organizing center protein trafficking. However, the mechanisms underlying the (Chabin-Brion et al., 2001; Efimov et al., 2007; Miller et al., 2009; microtubule organization of the Golgi remain obscure. We used Rivero et al., 2009). For example, almost half of all cellular immunoprecipitation coupled with mass spectrometry to identify a microtubules originate from the Golgi in human retinal pigment widely expressed isoform of the poorly characterized muscle protein epithelial RPE1 cells (Efimov et al., 2007). Moreover, microtubule myomegalin. This newly identified isoform, myomegalin variant 8 nucleation at the Golgi does not require centrosomes, and it (MMG8), localized predominantly to cis-Golgi networks by interacting depends instead on c-tubulin (Efimov et al., 2007), the principal with AKAP450 (also known as AKAP9), and this interaction with microtubule nucleator in cells, which exists in the form of c-tubulin AKAP450 was required for the stability of both proteins. Disrupting complexes (cTuCs). The cis-Golgi proteins AKAP450 (also known MMG8 expression affected endoplasmic reticulum (ER)-to-Golgi as AKAP9, AKAP350, CG-NAP and hyperion) and GMAP210 trafficking and caused Golgi fragmentation. -
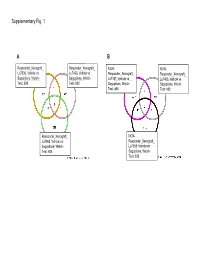
Supplementary Data
Supplementary Fig. 1 A B Responder_Xenograft_ Responder_Xenograft_ NON- NON- Lu7336, Vehicle vs Lu7466, Vehicle vs Responder_Xenograft_ Responder_Xenograft_ Sagopilone, Welch- Sagopilone, Welch- Lu7187, Vehicle vs Lu7406, Vehicle vs Test: 638 Test: 600 Sagopilone, Welch- Sagopilone, Welch- Test: 468 Test: 482 Responder_Xenograft_ NON- Lu7860, Vehicle vs Responder_Xenograft_ Sagopilone, Welch - Lu7558, Vehicle vs Test: 605 Sagopilone, Welch- Test: 333 Supplementary Fig. 2 Supplementary Fig. 3 Supplementary Figure S1. Venn diagrams comparing probe sets regulated by Sagopilone treatment (10mg/kg for 24h) between individual models (Welsh Test ellipse p-value<0.001 or 5-fold change). A Sagopilone responder models, B Sagopilone non-responder models. Supplementary Figure S2. Pathway analysis of genes regulated by Sagopilone treatment in responder xenograft models 24h after Sagopilone treatment by GeneGo Metacore; the most significant pathway map representing cell cycle/spindle assembly and chromosome separation is shown, genes upregulated by Sagopilone treatment are marked with red thermometers. Supplementary Figure S3. GeneGo Metacore pathway analysis of genes differentially expressed between Sagopilone Responder and Non-Responder models displaying –log(p-Values) of most significant pathway maps. Supplementary Tables Supplementary Table 1. Response and activity in 22 non-small-cell lung cancer (NSCLC) xenograft models after treatment with Sagopilone and other cytotoxic agents commonly used in the management of NSCLC Tumor Model Response type -

A Thyroid Hormone Receptor Coactivator Negatively Regulated by the Retinoblastoma Protein
Proc. Natl. Acad. Sci. USA Vol. 94, pp. 9040–9045, August 1997 Biochemistry A thyroid hormone receptor coactivator negatively regulated by the retinoblastoma protein KAI-HSUAN CHANG*†,YUMAY CHEN*†,TUNG-TI CHEN*†,WEN-HAI CHOU*†,PHANG-LANG CHEN*, YEN-YING MA‡,TERESA L. YANG-FENG‡,XIAOHUA LENG§,MING-JER TSAI§,BERT W. O’MALLEY§, AND WEN-HWA LEE*¶ *Department of Molecular Medicine and Institute of Biotechnology, University of Texas Health Science Center at San Antonio, 15355 Lambda Drive, San Antonio, TX 78245; ‡Department of Genetics, Obstetrics, and Gynecology, Yale University School of Medicine, New Haven, CT 06510; and §Department of Cell Biology, Baylor College of Medicine, Houston, TX 77030 Contributed by Bert W. O’Malley, June 9, 1997 ABSTRACT The retinoblastoma protein (Rb) plays a E2F-1, a transcription factor important for the expression of critical role in cell proliferation, differentiation, and devel- several genes involved in cell cycle progression from G1 to S opment. To decipher the mechanism of Rb function at the (18). Rb inhibits E2F-1 activity by blocking its transactivation molecular level, we have systematically characterized a num- region (19–21). In contrast, Rb has been shown to have the ber of Rb-interacting proteins, among which is the clone C5 ability to increase the transactivating activity of the members described here, which encodes a protein of 1,978 amino acids of the CCAATyenhancer binding protein (CyEBP) family, and with an estimated molecular mass of 230 kDa. The corre- to be required for CyEBPs-dependent adipocyte and mono- sponding gene was assigned to chromosome 14q31, the same cytes differentiation (16–17).