A Case Study of the Failure on Apollo 13 Based on TMX-65270, Report of Apollo 13 Review Board
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Apollo 13 Mission Review
APOLLO 13 MISSION REVIEW HEAR& BEFORE THE COMMITTEE ON AERONAUTICAL AND SPACE SCIENCES UNITED STATES SENATE NINETY-FIRST CONGRESS SECOR’D SESSION JUR’E 30, 1970 Printed for the use of the Committee on Aeronautical and Space Sciences U.S. GOVERNMENT PRINTING OFFICE 47476 0 WASHINGTON : 1970 COMMITTEE ON AEROKAUTICAL AND SPACE SCIENCES CLINTON P. ANDERSON, New Mexico, Chairman RICHARD B. RUSSELL, Georgia MARGARET CHASE SMITH, Maine WARREN G. MAGNUSON, Washington CARL T. CURTIS, Nebraska STUART SYMINGTON, bfissouri MARK 0. HATFIELD, Oregon JOHN STENNIS, Mississippi BARRY GOLDWATER, Arizona STEPHEN M.YOUNG, Ohio WILLIAM B. SAXBE, Ohio THOJfAS J. DODD, Connecticut RALPH T. SMITH, Illinois HOWARD W. CANNON, Nevada SPESSARD L. HOLLAND, Florida J4MES J. GEHRIG,Stad Director EVERARDH. SMITH, Jr., Professional staffMember Dr. GLENP. WILSOS,Professional #tad Member CRAIGVOORHEES, Professional Staff Nember WILLIAMPARKER, Professional Staff Member SAMBOUCHARD, Assistant Chief Clerk DONALDH. BRESNAS,Research Assistant (11) CONTENTS Tuesday, June 30, 1970 : Page Opening statement by the chairman, Senator Clinton P. Anderson-__- 1 Review Board Findings, Determinations and Recommendations-----_ 2 Testimony of- Dr. Thomas 0. Paine, Administrator of NASA, accompanied by Edgar M. Cortright, Director, Langley Research Center and Chairman of the dpollo 13 Review Board ; Dr. Charles D. Har- rington, Chairman, Aerospace Safety Advisory Panel ; Dr. Dale D. Myers, Associate Administrator for Manned Space Flight, and Dr. Rocco A. Petrone, hpollo Director -___________ 21, 30 Edgar 11. Cortright, Chairman, hpollo 13 Review Board-------- 21,27 Dr. Dale D. Mvers. Associate Administrator for Manned SDace 68 69 105 109 LIST OF ILLUSTRATIOSS 1. Internal coinponents of oxygen tank So. 2 ---_____-_________________ 22 2. -
Apollo 13--200,000Miles from Earth
Apollo13"Houston,we'vegota problem." EP-76,ProducedbytheO fficeofPublicA ffairs NationalAeronauticsandSpaceAdministration W ashington,D.C.20546 U.S.GOVERNM ENT PRINTING OFFICE,1970384-459 NOTE:Nolongerinprint. .pdf version by Jerry Woodfill of the Automation, Robotics, and Simulation Division, Johnson Space Center, Houston, Texas 77058 . James A. Lovell, Jr., Commander... Fred W. Haise, Jr., Lunar Module Pilot... John L. Swigeft, Jr., Command Module Pilot. SPACECRAFT--Hey, we've got a problem here. Thus, calmly, Command Module Pilot JackSwigert gave the first intimation of serious trouble for Apollo 13--200,000miles from Earth. CAPSULECOMMUNICATOR--ThisisHouston;say again, please. SC--Houston, we've hada problem. We've hada MainBbusundervolt. By "undervolt"Swigert meant a drop in power in one of the Command/Service Module's two main electrical circuits. His report to the ground began the most grippingepisode in man's venture into space. One newspaper reporter called it the most public emergency and the most dramatic rescue in the history of exploration. SC--Andwe hada pretty large bang associatedwith the cautionandwarning here. Lunar Module Pilot Fred Haise was now on the voice channel from the spacecraft to the Mission Control Center at the National Aeronautics and Space Administration's Manned Spacecraft Center in Texas. Commander Jim Lovell would shortly be heard, then again Swigert--the backup crewman who had been thrust onto the first team only two days before launch when doctors feared that Tom Mattingly of the primary crew might come down with German measles. Equally cool, the men in Mission Control acknowledged the report and began the emergency procedures that grew into an effort by hundreds of ground controllers and thousands of technicians and scientists in NaSA contractor plants and On university campuses to solve the most complexand urgent problem yet encountered in space flight. -

Apollo Over the Moon: a View from Orbit (Nasa Sp-362)
chl APOLLO OVER THE MOON: A VIEW FROM ORBIT (NASA SP-362) Chapter 1 - Introduction Harold Masursky, Farouk El-Baz, Frederick J. Doyle, and Leon J. Kosofsky [For a high resolution picture- click here] Objectives [1] Photography of the lunar surface was considered an important goal of the Apollo program by the National Aeronautics and Space Administration. The important objectives of Apollo photography were (1) to gather data pertaining to the topography and specific landmarks along the approach paths to the early Apollo landing sites; (2) to obtain high-resolution photographs of the landing sites and surrounding areas to plan lunar surface exploration, and to provide a basis for extrapolating the concentrated observations at the landing sites to nearby areas; and (3) to obtain photographs suitable for regional studies of the lunar geologic environment and the processes that act upon it. Through study of the photographs and all other arrays of information gathered by the Apollo and earlier lunar programs, we may develop an understanding of the evolution of the lunar crust. In this introductory chapter we describe how the Apollo photographic systems were selected and used; how the photographic mission plans were formulated and conducted; how part of the great mass of data is being analyzed and published; and, finally, we describe some of the scientific results. Historically most lunar atlases have used photointerpretive techniques to discuss the possible origins of the Moon's crust and its surface features. The ideas presented in this volume also rely on photointerpretation. However, many ideas are substantiated or expanded by information obtained from the huge arrays of supporting data gathered by Earth-based and orbital sensors, from experiments deployed on the lunar surface, and from studies made of the returned samples. -

Endless Possibilities at NASA Congestion, and Evaluating New Aircraft Designs
National Aeronautics and Space Administration National Aeronautics and Space Administration Langley Research Center Hampton, VA 23681 NP-2014-12-579-LaRC www.nasa.gov LANGLEY RESEARCH CENTER 2014 iv 1 With the launch of Orion in December, NASA took the first steps toward the future of human space exploration. Langley contributed critical elements to the mission: a launch abort system, structural impact testing, recovery testing, heat shield validation, and wind tunnel testing. The flight test went flawlessly and met NASA’s key objectives. NASA/George Homich A D8 airliner concept from a team led by the Massachusetts Institute of Technology is tested in Langley’s 14 by-22-Foot Subsonic Tunnel. NASA is working with industry and university partners to develop technologies and systems for aircraft that will reduce noise, emissions and fuel consumption. NASA Photos in this publication are by David C. Bowman of NASA Langley unless otherwise credited. 2 3 t’s time once again to recognize many of the past That work includes reducing aircraft noise around year’s accomplishments while looking ahead to airports, boosting fuel efficiency, relieving air traffic another year of endless possibilities at NASA congestion, and evaluating new aircraft designs. ILangley Research Center. In 2014, NASA’s Environmentally Responsible The pages of this report highlight steps we’ve Aviation program used an innovative manu- At right: Space Launch System taken and progress toward enabling human models have been tested in several facturing process to build a 10,000-pound Langley wind tunnels, including exploration of the solar system, as well as our composite aircraft structure for testing at this one in the Transonic Dynamics work helping improve the air travel system and Langley. -
Interviews with the Apollo Lunar Surface Astronauts in Support of Planning for EVA Systems Design
NASA Technical Memorandum 108846 Interviews with the Apollo Lunar Surface Astronauts in Support of Planning for EVA Systems Design Mary M. Connors, Ames Research Center, Moffett Field, California Dean B. Eppler, SAIC, Houston, Texas Daniel G. Morrow, Decision Systems, Los Altos, California September 1994 NASA National Aeronautics and Space Administration Ames Research Center Moffett Field, California 94035-1000 Interviews with the Apollo Lunar Surface Astronauts in Support of Planning for EVA Systems Design MARY M. CONNORS, DEAN B. EPPLER,* AND DANIEL G. MORROW** Ames Research Center Summary was to explicate any other insights that could help further the planning process. Focused interviews were conducted with the Apollo astronauts who landed on the Moon. The purpose of The intended primary audience for this study is mission these interviews was to help define extravehicular activity planners and scientists and engineers responsible for (EVA) system requirements for future lunar and planetary EVA system design. However, we anticipate that various missions. Information from the interviews was examined aspects of the report may also be of interest to a wider with particular attention to identifying areas of consensus, readership and it is written to be accessible to anyone since some commonality of experience is necessary to aid with a general interest in EVA. the design of advanced systems. Results are presented This study followed a request made by the Office of under the following categories: mission approach; Exploration, NASA Headquarters, to the New Initiatives mission structure; suits; portable life support systems; Office at Johnson Space Center (JSC). The study team dust control; gloves; automation; information, displays, was headed by Robert Callaway of the New Initiative and controls; rovers and remotes; tools; operations; Office and included members of the Crew and Thermal training; and general comments. -

Download Chapter 457KB
Memorial Tributes: Volume 17 Copyright National Academy of Sciences. All rights reserved. Memorial Tributes: Volume 17 ABE SILVERSTEIN 1908–2001 Elected in 1967 “For aeronautical and space systems.” BY ROBERT S. ARRIGHI SUBMITTED BY THE NAE HOME SECRETARY ABE SILVERSTEIN was a visionary engineer and leader whose accomplishments during his 40-year career continue to impact the aerospace community. He was instrumental in the design of a massive subsonic wind tunnel (the Full-Scale Tunnel), study of complete engine systems, development of the nation’s early jet engines and ramjets, creation of large supersonic wind tunnels, use of liquid hydrogen as a propellant, the foundation of NASA, formation of the Mercury and Apollo Programs, the success of the Centaur second- stage rocket, and a great deal more. He excelled at instantly grasping the essence of a problem, proposing a likely solution, and delegating the task to the experts to resolve. His off-the- cuff acumen and decisiveness inspired both fear and intense loyalty from staff and colleagues. Abe Silverstein died on June 1, 2001, at the age of 92. Abe was born on September 15, 1908, in Terre Haute, Indiana, to Joseph and Eva Silverstein. His father advised him at a young age to pursue engineering, and Abe claimed that his mother’s insistence on perfection in his school work provided him with the mindset required for future space engineering. Abe graduated from Terre Haute’s Rose Polytechnic Institute in 1929 with a BS in mechanical engineering. He returned to earn a degree as a mechanical engineering professional in 1934. -
View the Apollo 13 Chart
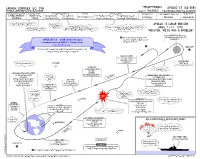
APOLLO 13 (AS-508) LC-39A JULY 2015 JOHN F. KENNEDY SPACE CENTER AS-508-2 3rd LUNAR LANDING MISSION MISSION FACTS & HIGHLIGHTS Apollo 13 was to be NASA’s third mission to land on the Moon. The spacecraft launched from the Kennedy Space Center in Florida. Midway to the moon, an explosion in one of the oxygen tanks of the service module crippled the spacecraft. After the in-flight emergency, for safety reasons, the crew was forced to temporarily power down and evacuate the command module, taking refuge in the lunar module. The spacecraft then orbited the Moon without landing. Later in the flight, heading back toward Earth, the crew returned to the command module, restored power, jettisoned the damaged service module, then the lunar module and, after an anxious re- entry blackout period, returned safely to the Earth. The command module and its crew slasheddown in the South Pacific Ocean and were recovered by the U.S.S. Iwo Jima (LPH-2). FACTS • Apollo XIII Mission Motto: Ex Luna, Scientia • Lunar Module: Aquarius • Command and Service Module: Odyssey • Crew: • James A. Lovell, Jr. - Commander • John L. Swigert, Jr. - Command Module Pilot ( * ) • Fred W. Haise, Jr. - Lunar Module Pilot • NASA Flight Directors • Milt Windler - Flight Director Shift #1 • Gerald Griffin - Flight Director Shift #2 • Gene Kranz - Flight Director Shift #3 • Glynn Lunney - Flight Director Shift #4 • William Reeves - Systems • Launch Site: John F. Kennedy Space Center, Florida • Launch Complex: Pad 39A • Launch: 2:13 pm EST, April 11, 1970 •Orbit: • Altitude: 118.99 miles • Inclination 32.547 degrees • Earth orbits: 1.5 • Lunar Landing Site: Intended to be Fra Mauro (later became landing site for Apollo 14) • Return to Earth: April 17, 1970 • Splashdown: 18:07:41 UTC (1:07:41 pm EST) • Recovery site location: South Pacific Ocean (near Samoa) S21 38.6 W165 21.7 • Recovery ship: U.S.S. -

2003 Astronomy Magazine Index
2003 astronomy magazine index Catchall (Martian crater), 11:30 observing Mars from, 7:32 hydrogen, 10:28 Subject index CCD (charge-coupled device) cameras, planets like, 6:48–53 Hydrus (constellation), 10:72–75 3:84–87, 5:84–87 seasons of, 3:72–73 A CCD techniques, 9:100–105 tilt of axis, 2:68, 5:72–73 I accidents, space-related, 7:42–47 Celestron C6-R (refractor), 11:84 EarthExplorer web site, 4:30 Achernar (star), 10:30 iceball, found beyond Pluto, 1:24 Celestron C8-N (reflector), 11:86 eclipses India, plans to visit Moon, 10:29 Advanced Camera for Surveys, 4:28 Celestron CGE-1100 (amateur telescope), in Australia (2003), 4:80–83 ALMA (Atacama Large Millimeter Array), infrared survey, 8:31 11:88 lunar integrating wavelengths, 4:24 3:36 Celestron NexStar 8 GPS (amateur telescope), of 2003, 5:18 Amalthea (Jupiter’s moon), 4:28 interferometry 1:84–87 of May 15, 2003, 5:60, 80–83, 88–89 techniques for, 7:48–53 Amateur Achievement Award, 9:32 Celestron NexStar 8i (amateur telescope), solar Andromeda Galaxy VLT interferometer, 2:32 11:89 of May 31, 2003, 5:80–83, 88–89 International Space Station, 3:31 picture of, 2:12–13 Centaurus A (NGC 5128) galaxy Edgar Wilson Award, 11:30 young stars in, 9:86–89 Internet, virtual observatories on, 9:80–85 1,000 Mira stars discovered in, 10:28 Egg Nebula, 8:36 Intes MK67 (amateur telescope), 11:89 Annefrank (asteroid), 2:32 picture of, 10:12–13 elliptical galaxies, 8:31 antineutrinos, 4:26 Io (Jupiter’s moon), 3:30 ripped apart satellite galaxy, 2:32 Eta Carinae (nebula), 5:29 ISAAC multi-mode instrument, 4:32 antisolar point, 10:18 Centaurus (constellation), 4:74–77 ETX-90EC (amateur telescope), 11:89 Antlia (constellation), 4:74–77 cepheid variable stars, 9:90–91 Europa (Jupiter’s moon), 12:30, 77 aphelion, 6:68–69 Challenger (space shuttle), 7:42–47 exoplanet magnetosphere, 11:28 J Apollo 1 (spacecraft), 7:42–47 J002E3 satellite, 1:30 Chamaeleon (constellation), 12:80–83 extrasolar planets. -

NEWSLETTER Apollo 13
P LANETARY S CIENCE I NSTITUTE NEWSLETTER SUMMER 2010 Vol. 11, No. 2 Est. 1972 www.psi.edu Apollo 13: Forty Years Later Don Davis recalls his role in the mission By April 1970, even the Apollo program was getting a bit humdrum for many of us who had been involved in NASA’s space program for years. Hard to believe, but going to the moon was just routine follow- ing the stunning successes of the previous 16 months:C. Holmberg Apollo 8, breaking the bonds of Earth gravity with the first human C. Holmberg spaceflight, sending astronauts to orbit the moon at Christmastime, 1968; Apollo 10, the dress rehearsal mission; Apollo 11, the first lunar landing, thereby meeting Presi- dent Kennedy’s 1961 challenge to the na- tion to put a man on the moon; and Apollo In 1970, Don Davis (center) working at mission control along- 12, struck by a tremendous bolt of light- side Poppy Northcutt, a member of the software team through- Everyone needed a badge to out the project. During Apollo 11, a Paris Match reporter ning at lift-off yet still completed a suc- get into mission control. featured her in an article, dubbing her the “Venus of Apollo.” cessful mission. So, everything was going smoothly in the program, and the big worry within the project was the American public’s growing disenchantment with space as Vietnam con- tinued to splinter the country. However, there were seven more missions planned (Apollo 20 was can- celed in January, 1970), so NASA continued on, expanding the capabili- ties of the astronauts on the moon with more stay time, a buggy to drive, and a host of other improvements that led to a scientific treasure trove. -

Apollo 16 Press
.. Arii . cLyI( ’ JOHN F . KENNEDY Si ACE GENTEb @@C€ i!AM LIB XRY cJ- / NATIONAL AERONAUTICS AND SPACE ADMINISTRATION Washington, D . C . 20546 202-755-8370 I FOR RELEASE: THURSDAY A .M . RELEASE NO: 12-64X April 6. 1972 PRO IFCT. APOLLO 16 (To be launched no earlier than April 16) E GENERAL RELEASE ..................... .1-5 COUNTDOWN ........................ 6-10 Launch Windows ................... .9 Ground Elapsed Time Update ............. .10 LAUNCH AND MISSION PROFILE ............... 11-39 Launch Events .................... 15-16 Mission Events .............. ..... 19-24 EVA Mission Events ................. 29-39 APOLLO 16 MISSION OBJECTIVES .............. 40-41 SCIENTIFIC RESULTS OF APOLLO 11, 12. 14 AND 15 MISSIONS . 42-44 APOLLO 16 LANDING SITE ................. 45-47 LUNAR SURFACE SCIENCE .................. 48-85 Passive Seismic Experiment ............. 48-52 ALSEP to Impact Distance Table ...... ..... 52-55 Lunar Surface Magnetometer ............. 55-58 Magnetic Lunar sample Returned to the Moon ..... .59 K Lunar Heat Flow Experiment ............. 60-65 ALSEP Central Station ................ .65 SNAP-27 .. Power Source for ALSEP .......... 66-67 Soil Mechanics ................... .68 I Lunar Portable Magnetometer ............. 68-71 Far Ultraviolet Camera/Spectroscope ......... 71-73 Solar Wind Composition Experiment .......... .73 Cosmic Ray Detector ................. .74 T Lunar Geology Investigation........ ..... 75-78 Apollo Lunar Geology Hand Tools ........... 79-85 LUNAR ORBITAL SCIENCE ............. ...... 86-98 Gamma-Ray -

Small Satellite Earth-To-Moon Direct Transfer Trajectories Using the CR3BP
Scholars' Mine Masters Theses Student Theses and Dissertations Fall 2019 Small satellite earth-to-moon direct transfer trajectories using the CR3BP Garrett Levi McMillan Follow this and additional works at: https://scholarsmine.mst.edu/masters_theses Part of the Aerospace Engineering Commons Department: Recommended Citation McMillan, Garrett Levi, "Small satellite earth-to-moon direct transfer trajectories using the CR3BP" (2019). Masters Theses. 7920. https://scholarsmine.mst.edu/masters_theses/7920 This thesis is brought to you by Scholars' Mine, a service of the Missouri S&T Library and Learning Resources. This work is protected by U. S. Copyright Law. Unauthorized use including reproduction for redistribution requires the permission of the copyright holder. For more information, please contact [email protected]. SMALL SATELLITE EARTH-TO-MOON DIRECT TRANSFER TRAJECTORIES USING THE CR3BP by GARRETT LEVI MCMILLAN A THESIS Presented to the Graduate Faculty of the MISSOURI UNIVERSITY OF SCIENCE AND TECHNOLOGY In Partial Fulfillment of the Requirements for the Degree MASTER OF SCIENCE in AEROSPACE ENGINEERING 2019 Approved by: Dr. Henry Pernicka, Advisor Dr. David Riggins Dr. Serhat Hosder Copyright 2019 GARRETT LEVI MCMILLAN All Rights Reserved iii ABSTRACT The CubeSat/small satellite field is one of the fastest growing means of space exploration, with applications continuing to expand for component development, commu- nication, and scientific research. This thesis study focuses on establishing suitable small satellite Earth-to-Moon direct-transfer trajectories, providing a baseline understanding of their propulsive demands, determining currently available off-the-shelf propulsive technol- ogy capable of meeting these demands, as well as demonstrating the effectiveness of the Circular Restricted Three Body Problem (CR3BP) for preliminary mission design. -

Flight to the Moon Spacecraft Attitude Control, MIT IAP 16.S585
1/17/21 Earth-Moon Orbit Orbital Period: 27-1/2 days One side of Moon always faces Earth Flight to the Moon Spacecraft Attitude Control, MIT IAP 16.S585 Robert Stengel Princeton University There is no “Dark Side” January 14, 2021 1 ALL SIDES are dark once a month 2 1 2 The Earth and the Moon December 17, 1958 Earth mass = 81.4 x Moon mass Orbit eccentricity = 0.05 1st Cosmonaut Mercury 7, 1959 Class, 1959 3 4 3 4 1 1/17/21 April 12, 1961 February 20, 1962 John Glenn Vostok 1 Friendship 7 Mercury-Atlas Yuri Gagarin 5 6 5 6 Project Gemini [1965-66] Lunar Missions 10 crewed Titan II missions June 1961 Competition among contractors for the spacecraft and launch rockets US takes Space Race Lead 7 8 7 8 2 1/17/21 First Apollo Program Contract MIT Instrumentation Laboratory August 9, 1961 HOWEVER … Lunar landing technique had not been decided 9 10 9 10 Alternative Landers Saturn 3rd Stage 11 12 11 12 3 1/17/21 Proposed Saturn Launch Vehicles July 1962 Two Saturn 5s One or One Saturn 5 Nova Ten Saturn 1s Saturn 1 Saturn 5 Nova (Saturn 8) 13 14 13 14 Saturn Launch Vehicles Saturn 1B Saturn 5 The Apollo Modules Earth Orbit Missions Lunar Missions Service Command Lunar Module Module Module North American Grumman 15 16 15 16 4 1/17/21 First Manned Flight, Apollo 7 Apollo 8, December 21-27, 1968 October 11, 1968 • Earth-orbit mission to test LM planned • More ambitious mission was pursued st Eisele Schirra Cunningham • Repurposed to 1 manned flight to the Moon • 6-day mission, no Lunar Module Coast Reentry Trans- Moon’s Lunar Coast Injection “Sphere