Apollo 13 Mission Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Interview Transcript
ORAL HISTORY 7 TRANSCRIPT GLYNN S. LUNNEY INTERVIEWED BY CAROL BUTLER HOUSTON, TX – 18 OCTOBER 1999 BUTLER: Today is October 18, 1999. This oral history with Glynn Lunney is being conducted in the offices of the Signal Corporation in Houston, Texas, for the Johnson Space Center Oral History Project. Carol Butler is the interviewer and is assisted by Kevin Rusnak and Jason Abbey. Thank you for joining us today, again. LUNNEY: You're welcome. Glad to be here. BUTLER: We began talking the last time about Apollo-Soyuz [Test Project (ASTP)], and you told us a little bit about how you got involved with it and how Chris [Christopher C.] Kraft [Jr.] had called you up and asked you to become a part of this program, and how that was a little bit of a surprise, but you jumped into it. What did you think about working with the Soviet Union and people that had for so long been considered enemies, who you'd been in competition with on the space program, but were also enemies of the nation, to say? LUNNEY: Especially on the front end, it's a fairly foreboding and intimidating kind of an idea. Of course, I was raised and came of age in the fifties and sixties, and we went through a great deal of scare with respect to the Soviet Union. The newsreels had the marches through Red Square, you know, with the missiles and so on, tanks. A lot of things happened to reinforce that. There was, of course, the Cuban Missile Crisis early in [President] John [F.] Kennedy's administration. -

History of Rocket Technology
CHAPTER 1 History of Rockets 1. 1. INTRODUCTION Action-Reaction Principle Take any technology and you always find that its practical demonstration had been realized much before the theory was established. However, you may note that the fast and effective refinement of a technology begins only after its theory, explaining the underlying basic principles, has been established. The action-reaction principle that is fundamental to jet propulsion, which includes airbreathing- as well as rocket-propulsion, was theoretically explained only in 1687 by the English scientist Sir Isaac Newton by his famous publication “Philosophiae Naturalis Principia Mathematica (“Mathematical Principles of Natural Philosophy”). But, approximately 2100 years before this, Archytas, a Greek philosopher, mathematician, astronomer, statesman, and strategist, had demonstrated the action-reaction principle by his toy pigeon in the city of Tarentum, Fig. 1. 1. Archytas suspended on a wire his wooden pigeon that contained hot steam at an elevated pressure in its belly cavity. The other end of the wire was hooked on to the top of a tall pole. On releasing a plug, a jet of steam escaped through a hole from the rear of the pigeon to produce a thrust that made the toy pigeon fly in circles around the pole. Thus Archytas mystified and amused the citizens of Tarentum by his flying toy- pigeon and demonstrated the fundamental principle of propulsion: “every force has an equal and opposite reaction”. The second recorded-demonstration of the action-reaction principle was in the first century B.C. Hero of Alexandria, a Greek mathematician 1 and scientist, constructed a device known as aeolipile. -
PEANUTS and SPACE FOUNDATION Apollo and Beyond
Reproducible Master PEANUTS and SPACE FOUNDATION Apollo and Beyond GRADE 4 – 5 OBJECTIVES PAGE 1 Students will: ö Read Snoopy, First Beagle on the Moon! and Shoot for the Moon, Snoopy! ö Learn facts about the Apollo Moon missions. ö Use this information to complete a fill-in-the-blank fact worksheet. ö Create mission objectives for a brand new mission to the moon. SUGGESTED GRADE LEVELS 4 – 5 SUBJECT AREAS Space Science, History TIMELINE 30 – 45 minutes NEXT GENERATION SCIENCE STANDARDS ö 5-ESS1 ESS1.B Earth and the Solar System ö 3-5-ETS1 ETS1.B Developing Possible Solutions 21st CENTURY ESSENTIAL SKILLS Collaboration and Teamwork, Communication, Information Literacy, Flexibility, Leadership, Initiative, Organizing Concepts, Obtaining/Evaluating/Communicating Ideas BACKGROUND ö According to NASA.gov, NASA has proudly shared an association with Charles M. Schulz and his American icon Snoopy since Apollo missions began in the 1960s. Schulz created comic strips depicting Snoopy on the Moon, capturing public excitement about America’s achievements in space. In May 1969, Apollo 10 astronauts traveled to the Moon for a final trial run before the lunar landings took place on later missions. Because that mission required the lunar module to skim within 50,000 feet of the Moon’s surface and “snoop around” to determine the landing site for Apollo 11, the crew named the lunar module Snoopy. The command module was named Charlie Brown, after Snoopy’s loyal owner. These books are a united effort between Peanuts Worldwide, NASA and Simon & Schuster to generate interest in space among today’s younger children. -
A Comparative Analysis of the Geology Tools Used During the Apollo Lunar Program and Their Suitability for Future Missions to the Om on Lindsay Kathleen Anderson
University of North Dakota UND Scholarly Commons Theses and Dissertations Theses, Dissertations, and Senior Projects January 2016 A Comparative Analysis Of The Geology Tools Used During The Apollo Lunar Program And Their Suitability For Future Missions To The oM on Lindsay Kathleen Anderson Follow this and additional works at: https://commons.und.edu/theses Recommended Citation Anderson, Lindsay Kathleen, "A Comparative Analysis Of The Geology Tools Used During The Apollo Lunar Program And Their Suitability For Future Missions To The oonM " (2016). Theses and Dissertations. 1860. https://commons.und.edu/theses/1860 This Thesis is brought to you for free and open access by the Theses, Dissertations, and Senior Projects at UND Scholarly Commons. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of UND Scholarly Commons. For more information, please contact [email protected]. A COMPARATIVE ANALYSIS OF THE GEOLOGY TOOLS USED DURING THE APOLLO LUNAR PROGRAM AND THEIR SUITABILITY FOR FUTURE MISSIONS TO THE MOON by Lindsay Kathleen Anderson Bachelor of Science, University of North Dakota, 2009 A Thesis Submitted to the Graduate Faculty of the University of North Dakota in partial fulfillment of the requirements for the degree of Master of Science Grand Forks, North Dakota May 2016 Copyright 2016 Lindsay Anderson ii iii PERMISSION Title A Comparative Analysis of the Geology Tools Used During the Apollo Lunar Program and Their Suitability for Future Missions to the Moon Department Space Studies Degree Master of Science In presenting this thesis in partial fulfillment of the requirements for a graduate degree from the University of North Dakota, I agree that the library of this University shall make it freely available for inspection. -
Why NASA Consistently Fails at Congress
W&M ScholarWorks Undergraduate Honors Theses Theses, Dissertations, & Master Projects 6-2013 The Wrong Right Stuff: Why NASA Consistently Fails at Congress Andrew Follett College of William and Mary Follow this and additional works at: https://scholarworks.wm.edu/honorstheses Part of the Political Science Commons Recommended Citation Follett, Andrew, "The Wrong Right Stuff: Why NASA Consistently Fails at Congress" (2013). Undergraduate Honors Theses. Paper 584. https://scholarworks.wm.edu/honorstheses/584 This Honors Thesis is brought to you for free and open access by the Theses, Dissertations, & Master Projects at W&M ScholarWorks. It has been accepted for inclusion in Undergraduate Honors Theses by an authorized administrator of W&M ScholarWorks. For more information, please contact [email protected]. The Wrong Right Stuff: Why NASA Consistently Fails at Congress A thesis submitted in partial fulfillment of the requirement for the degree of Bachelors of Arts in Government from The College of William and Mary by Andrew Follett Accepted for . John Gilmour, Director . Sophia Hart . Rowan Lockwood Williamsburg, VA May 3, 2013 1 Table of Contents: Acknowledgements 3 Part 1: Introduction and Background 4 Pre Soviet Collapse: Early American Failures in Space 13 Pre Soviet Collapse: The Successful Mercury, Gemini, and Apollo Programs 17 Pre Soviet Collapse: The Quasi-Successful Shuttle Program 22 Part 2: The Thin Years, Repeated Failure in NASA in the Post-Soviet Era 27 The Failure of the Space Exploration Initiative 28 The Failed Vision for Space Exploration 30 The Success of Unmanned Space Flight 32 Part 3: Why NASA Fails 37 Part 4: Putting this to the Test 87 Part 5: Changing the Method. -

Apollo 14 Press
NATIONAL AERONAUTICS AND SPACE ADMINISTRATION WO 2-4155 WASHINGT0N.D.C. 20546 lELS.wo 36925 RELEASE NO: 71-3K FOR RELEASE: THURSDAY A. M . January 21, 1971 P R E S S K I T -more - 1/11/71 2 -0- NATIONAL AERONAUTICS AND SPACE ADMINISTRATION (m2) 962-4155 N E w s WASHINGTON,D.C. 20546 mu: (202) 963-6925 FOR RELEASE: THURSDAY A..M. January 21:, 1971 RELEASE NO: 71-3 APOLLO 14 LAUNCH JAN. 31 Apollo 14, the sixth United States manned flight to the Moon and fourth Apollo mission with an objective of landing men on the Moon, is scheduled for launch Jan. 31 at 3:23 p.m. EST from Kennedy Space Center, Fla. The Apollo 14 lunar module is to land in the hilly upland region north of the Fra Mauro crater for a stay of about 33 hours, during whick, the landing crew will leave the spacecraft twice to set up scientific experiments on the lunar surface and to continue geological explorations. The two earlier Apollo lunar landings were Apollo 11 at Tranquillity Base and Apollo 12 at Surveyor 3 crater in the Ocean of Storms. Apollo 14 prime crewmen are Spacecraft Commander Alan B. Shepard, Jr., Command Module Pilot Stuart A. Roosa, and Lunar Module Pilot Edgar I). Mitchell. Shepard is a Navy car-sain Roosa an Air Force major and Mitchell a Navy commander. -more- 1/8/71 -2- Lunar materials brought- back from the Fra Mauro formation are expected to yield information on the early history of the Moon, the Earth and the solar system--perhaps as long ago as five billion years. -
Apollo 14 Lunar Landing Feb. 5
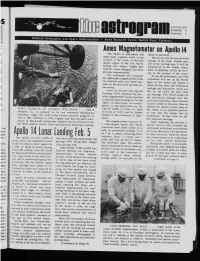
,$ VOLUME XIII NUMBER 8 February 4 National Aeronaulics and Sp :e Administration ,, Ames Research Center. Moffeft Field. California AmesMagnetometer on Apollo 14 The Apollo 14 astronauts will hours of operation. chart local magneticfields on the The devicewill be carriedon the surface of the moon, in the hilly outside of the Lunar Module near upland region of the Fra Mauro one of the landinglegs. It will be landing site, using a highly spe- transferredto the Mobile Equip- cialized,Ames designedand built, meat Transporter (MET) for mov- portablemagnetometer. ing on the surface of the moon. The astronautswill transport To use the instrument,one of the the lightweightmagnetometer on the astronautswill set up the sensor two-wheeledpush cart which car- head on the tripod and deploy it ries all the mission’sportable ex- about 40 feet from the electronics periments. package and indicators,which are Ames’ Dr. Palmer Dyal, Special left on the MET. He then calls ProjectsOffice, proposed the por- out readings from three meters on table magnetometerexperimentand the electronicspackage over the is the principalinvestigator for the voice communicationlink to Mission Apollo 14 experiment.Co-investi- ControlCenter at Houston.Then he gators on the experiment are Dr. rotates the cubical sensor head on FIRST AMERICAN TO JOURNEY INTO SPACE . Al.an B. Charles Sonett of Ames, Dr. Gene the tripodto an oppositeposition Shepard, Jr., is pictured as he was recovered following his Simmons of M.S.C. and Dr. Robert to fine tune the sensor and its suborbitalflight, the first in the Project Mercury program,on DuBois of the Universityof Okla- electronics.Be then calls out the May 5, t961. -

PEENEMUENDE, NATIONAL SOCIALISM, and the V-2 MISSILE, 1924-1945 Michael
ABSTRACT Title of Dissertation: ENGINEERING CONSENT: PEENEMUENDE, NATIONAL SOCIALISM, AND THE V-2 MISSILE, 1924-1945 Michael Brian Petersen, Doctor of Philosophy, 2005 Dissertation Directed By: Professor Jeffrey Herf Departmen t of History This dissertation is the story of the German scientists and engineers who developed, tested, and produced the V-2 missile, the world’s first liquid -fueled ballistic missile. It examines the social, political, and cultural roots of the prog ram in the Weimar Republic, the professional world of the Peenemünde missile base, and the results of the specialists’ decision to use concentration camp slave labor to produce the missile. Previous studies of this subject have been the domain of either of sensationalistic journalists or the unabashed admirers of the German missile pioneers. Only rarely have historians ventured into this area of inquiry, fruitfully examining the history of the German missile program from the top down while noting its admi nistrative battles and technical development. However, this work has been done at the expense of a detailed examination of the mid and lower -level employees who formed the backbone of the research and production effort. This work addresses that shortcomi ng by investigating the daily lives of these employees and the social, cultural, and political environment in which they existed. It focuses on the key questions of dedication, motivation, and criminality in the Nazi regime by asking “How did Nazi authori ties in charge of the missile program enlist the support of their employees in their effort?” “How did their work translate into political consent for the regime?” “How did these employees come to view slave labor as a viable option for completing their work?” This study is informed by traditions in European intellectual and social history while borrowing from different methods of sociology and anthropology. -
Apollo Soyuz Test Project
https://ntrs.nasa.gov/search.jsp?R=20190025708 2019-08-31T11:45:11+00:00Z Karol J. Bobko Background • Soviet –American cooperation in space had been discussed as early as 1962 by NASA’s Hugh Dryden and Academician Blagonrovov. • The major objectives for a cooperative space mission were: – 1) Demonstration in space of the new androgynous docking system, and – 2) Improvement of communication and reduction of Cold War tensions between East and West • In October 1970 R. Gilruth headed a small NASA delegation for a visit to Moscow to promote space cooperation. That visit was successful. • Following additional meetings, when President Nixon visited Moscow in May 1972, he and Alexei Kosygin signed an agreement providing for cooperation and the peaceful uses of space – The leaders specifically approved the Apollo-Soyuz flight being planned and they agreed on a 1975 launch. • Dr. Glynn Lunney was appointed as the U.S. technical director of the project • The US crew was announced in January; the USSR crew in May of 1973 • The first training visit was cosmonauts visiting JSC in July of 1973 System Changes • A Docking Module was developed to: – Act as an airlock between the two spacecraft • The Apollo operated with a 100% oxygen but at .34 atmospheres • The Soyuz normally operated at 1.0 atmospheres but for this flight it operated at .68 atmospheres • Since the difference between the modules was only .34 atmospheres it was felt the danger of going from one pressure to the other, without pre-breathe, was minimal. – The Docking Module had extra oxygen and nitrogen and executed the change in pressures to allow passage back and forth between the modules – The docking module had no capability to remove CO2 Docking Module (Cont.) • The front end of the Docking Module had the APDS, which was used to dock with the Soyuz • The rear part of the Docking Module had the probe and drogue system which was used to dock with the Apollo Command Module. -

Space Sector Brochure
SPACE SPACE REVOLUTIONIZING THE WAY TO SPACE SPACECRAFT TECHNOLOGIES PROPULSION Moog provides components and subsystems for cold gas, chemical, and electric Moog is a proven leader in components, subsystems, and systems propulsion and designs, develops, and manufactures complete chemical propulsion for spacecraft of all sizes, from smallsats to GEO spacecraft. systems, including tanks, to accelerate the spacecraft for orbit-insertion, station Moog has been successfully providing spacecraft controls, in- keeping, or attitude control. Moog makes thrusters from <1N to 500N to support the space propulsion, and major subsystems for science, military, propulsion requirements for small to large spacecraft. and commercial operations for more than 60 years. AVIONICS Moog is a proven provider of high performance and reliable space-rated avionics hardware and software for command and data handling, power distribution, payload processing, memory, GPS receivers, motor controllers, and onboard computing. POWER SYSTEMS Moog leverages its proven spacecraft avionics and high-power control systems to supply hardware for telemetry, as well as solar array and battery power management and switching. Applications include bus line power to valves, motors, torque rods, and other end effectors. Moog has developed products for Power Management and Distribution (PMAD) Systems, such as high power DC converters, switching, and power stabilization. MECHANISMS Moog has produced spacecraft motion control products for more than 50 years, dating back to the historic Apollo and Pioneer programs. Today, we offer rotary, linear, and specialized mechanisms for spacecraft motion control needs. Moog is a world-class manufacturer of solar array drives, propulsion positioning gimbals, electric propulsion gimbals, antenna positioner mechanisms, docking and release mechanisms, and specialty payload positioners. -
Waltham on the Moon, Apollo 15 and the Search for the Holy Grail
Waltham on the Moon, Apollo 15 and the Search for the Holy Grail. Post contains Pict... Page 1 of 3 [ View Thread ] [ Return to Index ] [ Read Prev Msg ] [ Read Next Msg ] 'Poor Man's' Watch Forum ARCHIVE Waltham on the Moon, Apollo 15 and the Search for the Holy Grail. Posted By: Kelly M. Rayburn <[email protected]> Date: Wednesday, 27 August 2003, at 2:21 a.m. (Reto was kind enough to ask me to repost my earlier post on the above topic for the archives on the new server. It contains nothing new except the post script. If you have already read the post, please disregard.) Hi all: In preparation for purchasing an Omega Speedmaster Professional, I have done the obligatory research on the use of the Speedmaster in the NASA space program. Chuck Maddox's excellent article on Omega's history with the Apollo program revealed some interesting facts that I did not know. In brief: The cal. 321 Speedmasters were purchased by NASA for the astronauts' use prior to the introduction of the cal. 861 movement in 1968. Apparently it is generally accepted that only the cal. 321 Speedmasters were worn on the moon during the various moon missions, as the initial procurement of these watches around 1965 was distributed to all astonauts at that time (two each) with as many as twenty still left in inventory and never used following the final Apollo 17 mission in 1972. Apparently, there is no evidence that a cal. 861 Speedmaster was worn by any of the moonwalkers or that NASA had procured any cal. -

Appendix a Apollo 15: “The Problem We Brought Back from the Moon”
Appendix A Apollo 15: “The Problem We Brought Back From the Moon” Postal Covers Carried on Apollo 151 Among the best known collectables from the Apollo Era are the covers flown onboard the Apollo 15 mission in 1971, mainly because of what the mission’s Lunar Module Pilot, Jim Irwin, called “the problem we brought back from the Moon.” [1] The crew of Apollo 15 carried out one of the most complete scientific explorations of the Moon and accomplished several firsts, including the first lunar roving vehicle that was operated on the Moon to extend the range of exploration. Some 81 kilograms (180 pounds) of lunar surface samples were returned for anal- ysis, and a battery of very productive lunar surface and orbital experiments were conducted, including the first EVA in deep space. [2] Yet the Apollo 15 crew are best remembered for carrying envelopes to the Moon, and the mission is remem- bered for the “great postal caper.” [3] As noted in Chapter 7, Apollo 15 was not the first mission to carry covers. Dozens were carried on each flight from Apollo 11 onwards (see Table 1 for the complete list) and, as Apollo 15 Commander Dave Scott recalled in his book, the whole business had probably been building since Mercury, through Gemini and into Apollo. [4] People had a fascination with objects that had been carried into space, and that became more and more popular – and valuable – as the programs progressed. Right from the start of the Mercury program, each astronaut had been allowed to carry a certain number of personal items onboard, with NASA’s permission, in 1 A first version of this material was issued as Apollo 15 Cover Scandal in Orbit No.