Motor Systems Basal Ganglia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
(Mpfc-Lpmc) Affects Subjective Beauty but Not Ugliness
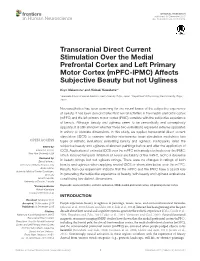
ORIGINAL RESEARCH published: 08 December 2015 doi: 10.3389/fnhum.2015.00654 Transcranial Direct Current Stimulation Over the Medial Prefrontal Cortex and Left Primary Motor Cortex (mPFC-lPMC) Affects Subjective Beauty but not Ugliness Koyo Nakamura1 and Hideaki Kawabata2* 1 Graduate School of Human Relations, Keio University, Tokyo, Japan, 2 Department of Psychology, Keio University, Tokyo, Japan Neuroaesthetics has been searching for the neural bases of the subjective experience of beauty. It has been demonstrated that neural activities in the medial prefrontal cortex (mPFC) and the left primary motor cortex (lPMC) correlate with the subjective experience of beauty. Although beauty and ugliness seem to be semantically and conceptually opposite, it is still unknown whether these two evaluations represent extreme opposites in unitary or bivariate dimensions. In this study, we applied transcranial direct current stimulation (tDCS) to examine whether non-invasive brain stimulation modulates two types of esthetic evaluation; evaluating beauty and ugliness. Participants rated the Edited by: subjective beauty and ugliness of abstract paintings before and after the application of Edward A. Vessel, tDCS. Application of cathodal tDCS over the mPFC with anode electrode over the lPMC, New York University, USA which induced temporal inhibition of neural excitability of the mPFC, led to a decrease Reviewed by: Zaira Cattaneo, in beauty ratings but not ugliness ratings. There were no changes in ratings of both University of Milano-Bicocca, Italy beauty and ugliness when applying anodal tDCS or sham stimulation over the mPFC. Andrea Antal, Results from our experiment indicate that the mPFC and the lPMC have a causal role University Medical Center Goettingen, Germany in generating the subjective experience of beauty, with beauty and ugliness evaluations Gerald Cupchik, constituting two distinct dimensions. -

Basal Ganglia & Cerebellum
1/2/2019 This power point is made available as an educational resource or study aid for your use only. This presentation may not be duplicated for others and should not be redistributed or posted anywhere on the internet or on any personal websites. Your use of this resource is with the acknowledgment and acceptance of those restrictions. Basal Ganglia & Cerebellum – a quick overview MHD-Neuroanatomy – Neuroscience Block Gregory Gruener, MD, MBA, MHPE Vice Dean for Education, SSOM Professor, Department of Neurology LUHS a member of Trinity Health Outcomes you want to accomplish Basal ganglia review Define and identify the major divisions of the basal ganglia List the major basal ganglia functional loops and roles List the components of the basal ganglia functional “circuitry” and associated neurotransmitters Describe the direct and indirect motor pathways and relevance/role of the substantia nigra compacta 1 1/2/2019 Basal Ganglia Terminology Striatum Caudate nucleus Nucleus accumbens Putamen Globus pallidus (pallidum) internal segment (GPi) external segment (GPe) Subthalamic nucleus Substantia nigra compact part (SNc) reticular part (SNr) Basal ganglia “circuitry” • BG have no major outputs to LMNs – Influence LMNs via the cerebral cortex • Input to striatum from cortex is excitatory – Glutamate is the neurotransmitter • Principal output from BG is via GPi + SNr – Output to thalamus, GABA is the neurotransmitter • Thalamocortical projections are excitatory – Concerned with motor “intention” • Balance of excitatory & inhibitory inputs to striatum, determine whether thalamus is suppressed BG circuits are parallel loops • Motor loop – Concerned with learned movements • Cognitive loop – Concerned with motor “intention” • Limbic loop – Emotional aspects of movements • Oculomotor loop – Concerned with voluntary saccades (fast eye-movements) 2 1/2/2019 Basal ganglia “circuitry” Cortex Striatum Thalamus GPi + SNr Nolte. -

Substance P and Antagonists of the Neurokinin-1 Receptor In
Martinez AN and Philipp MT, J Neurol Neuromed (2016) 1(2): 29-36 Neuromedicine www.jneurology.com www.jneurology.com Journal of Neurology & Neuromedicine Mini Review Article Open Access Substance P and Antagonists of the Neurokinin-1 Receptor in Neuroinflammation Associated with Infectious and Neurodegenerative Diseases of the Central Nervous System Alejandra N. Martinez1 and Mario T. Philipp1,2* 1Division of Bacteriology & Parasitology, Tulane National Primate Research Center, Covington, LA, USA 2Department of Microbiology and Immunology, Tulane University Medical School, New Orleans, LA, USA Article Info ABSTRACT Article Notes This review addresses the role that substance P (SP) and its preferred receptor Received: May 03, 2016 neurokinin-1 (NK1R) play in neuroinflammation associated with select bacterial, Accepted: May 18, 2016 viral, parasitic, and neurodegenerative diseases of the central nervous system. *Correspondence: The SP/NK1R complex is a key player in the interaction between the immune Division of Bacteriology and Parasitology and nervous systems. A common effect of this interaction is inflammation. For Tulane National Primate Research Center this reason and because of the predominance in the human brain of the NK1R, Covington, LA, USA its antagonists are attractive potential therapeutic agents. Preventing the Email: [email protected] deleterious effects of SP through the use of NK1R antagonists has been shown © 2016 Philipp MT. This article is distributed under the terms of to be a promising therapeutic strategy, as these antagonists are selective, the Creative Commons Attribution 4.0 International License potent, and safe. Here we evaluate their utility in the treatment of different neuroinfectious and neuroinflammatory diseases, as a novel approach to Keywords clinical management of CNS inflammation. -
Basal Ganglia Anatomy, Physiology, and Function Ns201c
Basal Ganglia Anatomy, Physiology, and Function NS201c Human Basal Ganglia Anatomy Basal Ganglia Circuits: The ‘Classical’ Model of Direct and Indirect Pathway Function Motor Cortex Premotor Cortex + Glutamate Striatum GPe GPi/SNr Dopamine + - GABA - Motor Thalamus SNc STN Analagous rodent basal ganglia nuclei Gross anatomy of the striatum: gateway to the basal ganglia rodent Dorsomedial striatum: -Inputs predominantly from mPFC, thalamus, VTA Dorsolateral striatum: -Inputs from sensorimotor cortex, thalamus, SNc Ventral striatum: Striatal subregions: Dorsomedial (caudate) -Inputs from vPFC, hippocampus, amygdala, Dorsolateral (putamen) thalamus, VTA Ventral (nucleus accumbens) Gross anatomy of the striatum: patch and matrix compartments Patch/Striosome: -substance P -mu-opioid receptor Matrix: -ChAT and AChE -somatostatin Microanatomy of the striatum: cell types Projection neurons: MSN: medium spiny neuron (GABA) •striatonigral projecting – ‘direct pathway’ •striatopallidal projecting – ‘indirect pathway’ Interneurons: FS: fast-spiking interneuron (GABA) LTS: low-threshold spiking interneuron (GABA) LA: large aspiny neuron (ACh) 30 um Cellular properties of striatal neurons Microanatomy of the striatum: striatal microcircuits • Feedforward inhibition (mediated by fast-spiking interneurons) • Lateral feedback inhibition (mediated by MSN collaterals) Basal Ganglia Circuits: The ‘Classical’ Model of Direct and Indirect Pathway Function Motor Cortex Premotor Cortex + Glutamate Striatum GPe GPi/SNr Dopamine + - GABA - Motor Thalamus SNc STN The simplified ‘classical’ model of basal ganglia circuit function • Information encoded as firing rate • Basal ganglia circuit is linear and unidirectional • Dopamine exerts opposing effects on direct and indirect pathway MSNs Basal ganglia motor circuit: direct pathway Motor Cortex Premotor Cortex Glutamate Striatum GPe GPi/SNr Dopamine + GABA Motor Thalamus SNc STN Direct pathway MSNs express: D1, M4 receptors, Sub. -

The Rigid Form of Huntington's Disease U
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.24.1.71 on 1 February 1961. Downloaded from J. Neurol. Neurosurg. Psychiat., 1961, 24, 71. THE RIGID FORM OF HUNTINGTON'S DISEASE BY A. M. G. CAMPBELL, BERYL CORNER, R. M. NORMAN, and H. URICH From the Department ofNeurosurgery and Child Health, Bristol Royal Hospital, and the Burden Neuropathological Laboratory, Frenchay Hospital, Bristol Although the majority of cases of hereditary genetic study of Entres (1925) to belong to a typical chorea correspond accurately to the classical pattern Huntington family. More recent contributions are described by Huntington (1872), a number of those of Rotter (1932), Hempel (1938), and atypical forms have been recorded in children and Lindenberg (1960). Bielschowsky (1922) gave a adults which are characterized by rigidity rather detailed account of the pathological findings in a than by hyperkinesia. Most of these have been patient who was choreic at the age of 6 years and reported in the continental literature and we thought from the age of 9 gradually developed Parkinsonian it was of interest to draw attention to two atypical rigidity. Our own juvenile case is remarkable in juvenile cases occurring in an English family. From Reisner's (1944) review of these juvenile U cases the fact emerges that although the majority A present with typical choreiform movements, two Protected by copyright. atypical variants also occur: one in which the clinical picture is that of progressive extrapyramidal BC rigidity without involuntary movements, the other in which the disease starts as a hyperkinetic syn- drome and gradually changes into a hypokinetic one with progressive rigidity. -

Clinical Manifestation of Juvenile and Pediatric HD Patients: a Retrospective Case Series
brain sciences Article Clinical Manifestation of Juvenile and Pediatric HD Patients: A Retrospective Case Series 1, , 2, 2 1 Jannis Achenbach * y, Charlotte Thiels y, Thomas Lücke and Carsten Saft 1 Department of Neurology, Huntington Centre North Rhine-Westphalia, St. Josef-Hospital Bochum, Ruhr-University Bochum, 44791 Bochum, Germany; [email protected] 2 Department of Neuropaediatrics and Social Paediatrics, University Children’s Hospital, Ruhr-University Bochum, 44791 Bochum, Germany; [email protected] (C.T.); [email protected] (T.L.) * Correspondence: [email protected] These two authors contribute to this paper equally. y Received: 30 April 2020; Accepted: 1 June 2020; Published: 3 June 2020 Abstract: Background: Studies on the clinical manifestation and course of disease in children suffering from Huntington’s disease (HD) are rare. Case reports of juvenile HD (onset 20 years) describe ≤ heterogeneous motoric and non-motoric symptoms, often accompanied with a delay in diagnosis. We aimed to describe this rare group of patients, especially with regard to socio-medical aspects and individual or common treatment strategies. In addition, we differentiated between juvenile and the recently defined pediatric HD population (onset < 18 years). Methods: Out of 2593 individual HD patients treated within the last 25 years in the Huntington Centre, North Rhine-Westphalia (NRW), 32 subjects were analyzed with an early onset younger than 21 years (1.23%, juvenile) and 18 of them younger than 18 years of age (0.69%, pediatric). Results: Beside a high degree of school problems, irritability or aggressive behavior (62.5% of pediatric and 31.2% of juvenile cases), serious problems concerning the social and family background were reported in 25% of the pediatric cohort. -

Restless Legs Syndrome: Keys to Recognition and Treatment
REVIEW JAIME F. AVECILLAS, MD JOSEPH A. GOLISH, MD CARMEN GIANNINI, RN, BSN JOSÉ C. YATACO, MD Department of Pulmonary and Critical Department of Pulmonary and Critical Department of Pulmonary and Critical Care Department of Pulmonary and Critical Care Care Medicine, The Cleveland Clinic Care Medicine and Department of Medicine, The Cleveland Clinic Foundation Medicine, The Cleveland Clinic Foundation Foundation Neurology, The Cleveland Clinic Foundation Restless legs syndrome: Keys to recognition and treatment ■ ABSTRACT ESTLESS LEGS SYNDROME (RLS) is not a R new diagnosis: it was first described com- Restless legs syndrome (RLS) is a common and clinically prehensively 60 years ago.1 However, it con- significant motor disorder increasingly recognized by tinues to be underdiagnosed, underreported, physicians and the general public, yet still and undertreated. Effective therapies for this underdiagnosed, underreported, and undertreated. motor disorder are available, but a high index Effective therapies are available, but a high index of of suspicion is necessary to identify the condi- suspicion is required to make the diagnosis and start tion and start treatment in a timely fashion. treatment quickly. We now have enough data to support Evidence from clinical trials supports the the use of dopaminergic agents, benzodiazepines, use of dopaminergic agents, benzodiazepines, antiepileptics, and opioids in these patients. antiepileptics, and opioids in these patients. The clinician must be familiar with the benefits ■ KEY POINTS and risks of these therapies to be able to provide optimal treatment in patients with RLS. RLS is characterized by paresthesias, usually in the lower extremities. Patients often describe them as “achy” or ■ CLINICAL DEFINITION: “crawling” sensations. -

Hippocampal–Caudate Nucleus Interactions Support Exceptional Memory Performance
Brain Struct Funct DOI 10.1007/s00429-017-1556-2 ORIGINAL ARTICLE Hippocampal–caudate nucleus interactions support exceptional memory performance Nils C. J. Müller1 · Boris N. Konrad1,2 · Nils Kohn1 · Monica Muñoz-López3 · Michael Czisch2 · Guillén Fernández1 · Martin Dresler1,2 Received: 1 December 2016 / Accepted: 24 October 2017 © The Author(s) 2017. This article is an open access publication Abstract Participants of the annual World Memory competitive interaction between hippocampus and caudate Championships regularly demonstrate extraordinary mem- nucleus is often observed in normal memory function, our ory feats, such as memorising the order of 52 playing cards findings suggest that a hippocampal–caudate nucleus in 20 s or 1000 binary digits in 5 min. On a cognitive level, cooperation may enable exceptional memory performance. memory athletes use well-known mnemonic strategies, We speculate that this cooperation reflects an integration of such as the method of loci. However, whether these feats the two memory systems at issue-enabling optimal com- are enabled solely through the use of mnemonic strategies bination of stimulus-response learning and map-based or whether they benefit additionally from optimised neural learning when using mnemonic strategies as for example circuits is still not fully clarified. Investigating 23 leading the method of loci. memory athletes, we found volumes of their right hip- pocampus and caudate nucleus were stronger correlated Keywords Memory athletes · Method of loci · Stimulus with each other compared to matched controls; both these response learning · Cognitive map · Hippocampus · volumes positively correlated with their position in the Caudate nucleus memory sports world ranking. Furthermore, we observed larger volumes of the right anterior hippocampus in ath- letes. -

Gene Expression of Prohormone and Proprotein Convertases in the Rat CNS: a Comparative in Situ Hybridization Analysis
The Journal of Neuroscience, March 1993. 73(3): 1258-1279 Gene Expression of Prohormone and Proprotein Convertases in the Rat CNS: A Comparative in situ Hybridization Analysis Martin K.-H. Schafer,i-a Robert Day,* William E. Cullinan,’ Michel Chri?tien,3 Nabil G. Seidah,* and Stanley J. Watson’ ‘Mental Health Research Institute, University of Michigan, Ann Arbor, Michigan 48109-0720 and J. A. DeSeve Laboratory of *Biochemical and 3Molecular Neuroendocrinology, Clinical Research Institute of Montreal, Montreal, Quebec, Canada H2W lR7 Posttranslational processing of proproteins and prohor- The participation of neuropeptides in the modulation of a va- mones is an essential step in the formation of bioactive riety of CNS functions is well established. Many neuropeptides peptides, which is of particular importance in the nervous are synthesized as inactive precursor proteins, which undergo system. Following a long search for the enzymes responsible an enzymatic cascade of posttranslational processing and mod- for protein precursor cleavage, a family of Kexin/subtilisin- ification events during their intracellular transport before the like convertases known as PCl, PC2, and furin have recently final bioactive products are secreted and act at either pre- or been characterized in mammalian species. Their presence postsynaptic receptors. Initial endoproteolytic cleavage occurs in endocrine and neuroendocrine tissues has been dem- C-terminal to pairs of basic amino acids such as lysine-arginine onstrated. This study examines the mRNA distribution of (Docherty and Steiner, 1982) and is followed by the removal these convertases in the rat CNS and compares their ex- of the basic residues by exopeptidases. Further modifications pression with the previously characterized processing en- can occur in the form of N-terminal acetylation or C-terminal zymes carboxypeptidase E (CPE) and peptidylglycine a-am- amidation, which is essential for the bioactivity of many neu- idating monooxygenase (PAM) using in situ hybridization ropeptides. -

Imaging of the Confused Patient: Toxic Metabolic Disorders Dara G
Imaging of the Confused Patient: Toxic Metabolic Disorders Dara G. Jamieson, M.D. Weill Cornell Medicine, New York, NY The patient who presents with either acute or subacute confusion, in the absence of a clearly defined speech disorder and focality on neurological examination that would indicate an underlying mass lesion, needs to be evaluated for a multitude of neurological conditions. Many of the conditions that produce the recent onset of alteration in mental status, that ranges from mild confusion to florid delirium, may be due to infectious or inflammatory conditions that warrant acute intervention such as antimicrobial drugs, steroids or plasma exchange. However, some patients with recent onset of confusion have an underlying toxic-metabolic disorders indicating a specific diagnosis with need for appropriate treatment. The clinical presentations of some patients may indicate the diagnosis (e.g. hypoglycemia, chronic alcoholism) while the imaging patterns must be recognized to make the diagnosis in other patients. Toxic-metabolic disorders constitute a group of diseases and syndromes with diverse causes and clinical presentations. Many toxic-metabolic disorders have no specific neuroimaging correlates, either at early clinical stages or when florid symptoms develop. However, some toxic-metabolic disorders have characteristic abnormalities on neuroimaging, as certain areas of the central nervous system appear particularly vulnerable to specific toxins and metabolic perturbations. Areas of particular vulnerability in the brain include: 1) areas of high-oxygen demand (e.g. basal ganglia, cerebellum, hippocampus), 2) the cerebral white matter and 3) the mid-brain. Brain areas of high-oxygen demand are particularly vulnerable to toxins that interfere with cellular respiratory metabolism. -

Conditional Ablation of Brain-Derived Neurotrophic Factor-Trkb Signaling Impairs Striatal Neuron Development
Conditional ablation of brain-derived neurotrophic factor-TrkB signaling impairs striatal neuron development Yun Lia,1, Daishi Yuia, Bryan W. Luikarta,2, Renée M. McKaya, Yanjiao Lia, John L. Rubensteinb, and Luis F. Paradaa,3 aDepartment of Developmental Biology and Kent Waldrep Center for Basic Research on Nerve Growth and Regeneration, University of Texas Southwestern Medical Center, Dallas, TX 75390; and bNina Ireland Laboratory of Developmental Neurobiology, Department of Psychiatry, University of California, San Francisco, CA 94143 Contributed by Luis F. Parada, August 2, 2012 (sent for review June 21, 2012) Neurotrophic factors, such as brain-derived neurotrophic factor cascades pertaining to development, maturation, and function of (BDNF), are associated with the physiology of the striatum and the striatum remains to be delineated. the loss of its normal functioning under pathological conditions. In this study, we conditionally ablated BDNF or its receptor The role of BDNF and its downstream signaling in regulating the TrkB in corticostriatal and nigrostriatal neuronal circuits. We development of the striatum has not been fully investigated, found that Bdnf deletion in both cortex and substantia nigra led to Bdnf complete depletion of BDNF protein in the striatum. Mutant mice however. Here we report that ablation of in both the cortex displayed dramatic developmental abnormalities and neurological and substantia nigra depletes BDNF in the striatum, and leads to impairments. Furthermore, specific deletion of TrkB from striatal fi impaired striatal development, severe motor de cits, and postnatal neurons was sufficient to produce this wide range of developmental lethality. Furthermore, striatal-specific ablation of TrkB, the gene deficits. Thus, our results demonstrate that BDNF and TrkB play encoding the high-affinity receptor for BDNF, is sufficient to elicit critical paracrine and cell-autonomous roles, respectively, in the an array of striatal developmental abnormalities, including de- development and maintenance of striatal neurons. -

MRI Atlas of the Human Deep Brain Jean-Jacques Lemaire
MRI Atlas of the Human Deep Brain Jean-Jacques Lemaire To cite this version: Jean-Jacques Lemaire. MRI Atlas of the Human Deep Brain. 2019. hal-02116633 HAL Id: hal-02116633 https://hal.uca.fr/hal-02116633 Preprint submitted on 1 May 2019 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution - NonCommercial - NoDerivatives| 4.0 International License MRI ATLAS of the HUMAN DEEP BRAIN Jean-Jacques Lemaire, MD, PhD, neurosurgeon, University Hospital of Clermont-Ferrand, Université Clermont Auvergne, CNRS, SIGMA, France This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ or send a letter to Creative Commons, PO Box 1866, Mountain View, CA 94042, USA. Terminologia Foundational Model Terminologia MRI Deep Brain Atlas NeuroNames (ID) neuroanatomica usages, classical and french terminologies of Anatomy (ID) Anatomica 1998 (ID) 2017 http://fipat.library.dal.ca In