HOXA9 in B-LINEAGE ALL PROMOTES SURVIVAL and PROLIFERATION of LEUKEMIC CELLS by Jarrett Thomas Whelan March, 2009 Director: Fred E
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Homeobox Gene Expression Profile in Human Hematopoietic Multipotent
Leukemia (2003) 17, 1157–1163 & 2003 Nature Publishing Group All rights reserved 0887-6924/03 $25.00 www.nature.com/leu Homeobox gene expression profile in human hematopoietic multipotent stem cells and T-cell progenitors: implications for human T-cell development T Taghon1, K Thys1, M De Smedt1, F Weerkamp2, FJT Staal2, J Plum1 and G Leclercq1 1Department of Clinical Chemistry, Microbiology and Immunology, Ghent University Hospital, Ghent, Belgium; and 2Department of Immunology, Erasmus Medical Center, Rotterdam, The Netherlands Class I homeobox (HOX) genes comprise a large family of implicated in this transformation proces.14 The HOX-C locus transcription factors that have been implicated in normal and has been primarily implicated in lymphomas.15 malignant hematopoiesis. However, data on their expression or function during T-cell development is limited. Using degener- Hematopoietic cells are derived from stem cells that reside in ated RT-PCR and Affymetrix microarray analysis, we analyzed fetal liver (FL) in the embryo and in the adult bone marrow the expression pattern of this gene family in human multipotent (ABM), which have the unique ability to self-renew and thereby stem cells from fetal liver (FL) and adult bone marrow (ABM), provide a life-long supply of blood cells. T lymphocytes are a and in T-cell progenitors from child thymus. We show that FL specific type of hematopoietic cells that play a major role in the and ABM stem cells are similar in terms of HOX gene immune system. They develop through a well-defined order of expression, but significant differences were observed between differentiation steps in the thymus.16 Several transcription these two cell types and child thymocytes. -

Geminin Deletion Increases the Number of Fetal Hematopoietic Stem Cells by Affecting the Expression of Key Transcription Factors Dimitris Karamitros1,*, Alexandra L
© 2015. Published by The Company of Biologists Ltd | Development (2015) 142, 70-81 doi:10.1242/dev.109454 RESEARCH ARTICLE STEM CELLS AND REGENERATION Geminin deletion increases the number of fetal hematopoietic stem cells by affecting the expression of key transcription factors Dimitris Karamitros1,*, Alexandra L. Patmanidi1,*, Panoraia Kotantaki1, Alexandre J. Potocnik2, Tomi Bähr-Ivacevic3, Vladimir Benes3, Zoi Lygerou4, Dimitris Kioussis2,‡ and Stavros Taraviras1,‡ ABSTRACT hematological stress and challenges (Beerman et al., 2010; Balancing stem cell self-renewal and initiation of lineage specification Cheshier et al., 2007). The prevailing model of hematopoiesis programs is essential for the development and homeostasis of the supports the existence of long-term hematopoietic stem cells (LT- hematopoietic system. We have specifically ablated geminin in the HSCs), which can provide long-term multipotent reconstitution of developing murine hematopoietic system and observed profound the hematopoietic system, and of short-term hematopoietic stem defects in the generation of mature blood cells, leading to embryonic cells (ST-HSCs) or multipotent progenitors (MPPs), with the lethality. Hematopoietic stem cells (HSCs) accumulated in the fetal potential to generate all blood lineages but with reduced self- liver following geminin ablation, while committed progenitors were renewal capacity (Luc et al., 2007; Mebius et al., 2001; Morrison reduced. Genome-wide transcriptome analysis identified key HSC et al., 1995; Randall et al., 1996; Traver et al., 2001). transcription factors as being upregulated upon geminin deletion, Even though it remains unclear how the balance between self- revealing a gene network linked with geminin that controls fetal renewal of HSCs and fate commitment is controlled and how a hematopoiesis. -

C/Ebpα Is an Essential Collaborator in Hoxa9/Meis1-Mediated Leukemogenesis
C/EBPα is an essential collaborator in Hoxa9/Meis1-mediated leukemogenesis Cailin Collinsa, Jingya Wanga, Hongzhi Miaoa, Joel Bronsteina, Humaira Nawera, Tao Xua, Maria Figueroaa, Andrew G. Munteana, and Jay L. Hessa,b,1 aDepartment of Pathology, University of Michigan, Ann Arbor, MI 48109; and bIndiana University School of Medicine, Indianapolis, IN 46202 Edited* by Louis M. Staudt, National Institutes of Health, Bethesda, MD, and approved May 19, 2014 (received for review February 12, 2014) Homeobox A9 (HOXA9) is a homeodomain-containing transcrip- with Hoxa9. In addition, C/EBP recognition motifs are enriched tion factor that plays a key role in hematopoietic stem cell expan- at Hoxa9 binding sites. sion and is commonly deregulated in human acute leukemias. A C/EBPα is a basic leucine-zipper transcription factor that plays variety of upstream genetic alterations in acute myeloid leukemia a critical role in lineage commitment during hematopoietic dif- −/− (AML) lead to overexpression of HOXA9, almost always in associ- ferentiation (18). Whereas Cebpa mice show complete loss of ation with overexpression of its cofactor meis homeobox 1 (MEIS1). the granulocytic compartment, recent work shows that loss of α A wide range of data suggests that HOXA9 and MEIS1 play a syn- C/EBP in adult HSCs leads to both an increase in the number ergistic causative role in AML, although the molecular mechanisms of functional HSCs and an increase in their proliferative and leading to transformation by HOXA9 and MEIS1 remain elusive. In repopulating capacity (19, 20). Conversely, CEBPA overexpression can promote transdifferentiation of a variety of fibroblastic cells to this study, we identify CCAAT/enhancer binding protein alpha (C/ the myeloid lineage and can induce monocytic differentiation in EBPα) as a critical collaborator required for Hoxa9/Meis1-mediated α MLL-fusion protein-mediated leukemias (21, 22). -

Supplementary Materials
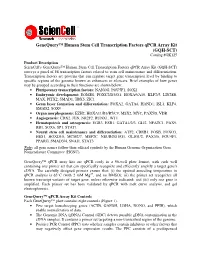
Supplementary Materials + - NUMB E2F2 PCBP2 CDKN1B MTOR AKT3 HOXA9 HNRNPA1 HNRNPA2B1 HNRNPA2B1 HNRNPK HNRNPA3 PCBP2 AICDA FLT3 SLAMF1 BIC CD34 TAL1 SPI1 GATA1 CD48 PIK3CG RUNX1 PIK3CD SLAMF1 CDKN2B CDKN2A CD34 RUNX1 E2F3 KMT2A RUNX1 T MIXL1 +++ +++ ++++ ++++ +++ 0 0 0 0 hematopoietic potential H1 H1 PB7 PB6 PB6 PB6.1 PB6.1 PB12.1 PB12.1 Figure S1. Unsupervised hierarchical clustering of hPSC-derived EBs according to the mRNA expression of hematopoietic lineage genes (microarray analysis). Hematopoietic-competent cells (H1, PB6.1, PB7) were separated from hematopoietic-deficient ones (PB6, PB12.1). In this experiment, all hPSCs were tested in duplicate, except PB7. Genes under-expressed or over-expressed in blood-deficient hPSCs are indicated in blue and red respectively (related to Table S1). 1 C) Mesoderm B) Endoderm + - KDR HAND1 GATA6 MEF2C DKK1 MSX1 GATA4 WNT3A GATA4 COL2A1 HNF1B ZFPM2 A) Ectoderm GATA4 GATA4 GSC GATA4 T ISL1 NCAM1 FOXH1 NCAM1 MESP1 CER1 WNT3A MIXL1 GATA4 PAX6 CDX2 T PAX6 SOX17 HBB NES GATA6 WT1 SOX1 FN1 ACTC1 ZIC1 FOXA2 MYF5 ZIC1 CXCR4 TBX5 PAX6 NCAM1 TBX20 PAX6 KRT18 DDX4 TUBB3 EPCAM TBX5 SOX2 KRT18 NKX2-5 NES AFP COL1A1 +++ +++ 0 0 0 0 ++++ +++ ++++ +++ +++ ++++ +++ ++++ 0 0 0 0 +++ +++ ++++ +++ ++++ 0 0 0 0 hematopoietic potential H1 H1 H1 H1 H1 H1 PB6 PB6 PB7 PB7 PB6 PB6 PB7 PB6 PB6 PB6.1 PB6.1 PB6.1 PB6.1 PB6.1 PB6.1 PB12.1 PB12.1 PB12.1 PB12.1 PB12.1 PB12.1 Figure S2. Unsupervised hierarchical clustering of hPSC-derived EBs according to the mRNA expression of germ layer differentiation genes (microarray analysis) Selected ectoderm (A), endoderm (B) and mesoderm (C) related genes differentially expressed between hematopoietic-competent (H1, PB6.1, PB7) and -deficient cells (PB6, PB12.1) are shown (related to Table S1). -

HOXA10 Controls Osteoblastogenesis by Directly Activating Bone Regulatory and Phenotypic Genes
University of Massachusetts Medical School eScholarship@UMMS Open Access Articles Open Access Publications by UMMS Authors 2007-02-28 HOXA10 controls osteoblastogenesis by directly activating bone regulatory and phenotypic genes Mohammad Q. Hassan University of Massachusetts Medical School Et al. Let us know how access to this document benefits ou.y Follow this and additional works at: https://escholarship.umassmed.edu/oapubs Part of the Life Sciences Commons, and the Medicine and Health Sciences Commons Repository Citation Hassan MQ, Tare RS, Lee SH, Mandeville M, Weiner B, Montecino MA, Van Wijnen AJ, Stein JL, Stein GS, Lian JB. (2007). HOXA10 controls osteoblastogenesis by directly activating bone regulatory and phenotypic genes. Open Access Articles. https://doi.org/10.1128/MCB.01544-06. Retrieved from https://escholarship.umassmed.edu/oapubs/1334 This material is brought to you by eScholarship@UMMS. It has been accepted for inclusion in Open Access Articles by an authorized administrator of eScholarship@UMMS. For more information, please contact [email protected]. MOLECULAR AND CELLULAR BIOLOGY, May 2007, p. 3337–3352 Vol. 27, No. 9 0270-7306/07/$08.00ϩ0 doi:10.1128/MCB.01544-06 Copyright © 2007, American Society for Microbiology. All Rights Reserved. HOXA10 Controls Osteoblastogenesis by Directly Activating Bone Regulatory and Phenotypic Genesᰔ Mohammad Q. Hassan,1 Rahul Tare,1† Suk Hee Lee,1 Matthew Mandeville,1 Brian Weiner,1 Martin Montecino,2 Andre J. van Wijnen,1 Janet L. Stein,1 Gary S. Stein,1 and Jane B. Lian1* Department of Cell Biology and Cancer Center, University of Massachusetts Medical School, Worcester, Massachusetts 01655,1 and Departamento de Bioquimica y Biologia Molecular, Facultad de Ciencias Biologicas, Universidad de Concepcion, Concepcion, Chile2 Received 18 August 2006/Returned for modification 4 October 2006/Accepted 9 February 2007 HOXA10 is necessary for embryonic patterning of skeletal elements, but its function in bone formation beyond this early developmental stage is unknown. -
Genequery™ Human Stem Cell Transcription Factors Qpcr Array
GeneQuery™ Human Stem Cell Transcription Factors qPCR Array Kit (GQH-SCT) Catalog #GK125 Product Description ScienCell's GeneQuery™ Human Stem Cell Transcription Factors qPCR Array Kit (GQH-SCT) surveys a panel of 88 transcription factors related to stem cell maintenance and differentiation. Transcription factors are proteins that can regulate target gene transcription level by binding to specific regions of the genome known as enhancers or silencers. Brief examples of how genes may be grouped according to their functions are shown below: • Pluripotency transcription factors: NANOG, POU5F1, SOX2 • Embryonic development: EOMES, FOXC2/D3/O1, HOXA9/A10, KLF2/5, LIN28B, MAX, PITX2, SMAD1, TBX5, ZIC1 • Germ layer formation and differentiation: FOXA2, GATA6, HAND1, ISL1, KLF4, SMAD2, SOX9 • Organ morphogenesis: EZH2, HOXA11/B3/B5/C9, MSX2, MYC, PAX5/8, VDR • Angiogenesis: CDX2, JUN, NR2F2, RUNX1, WT1 • Hematopoiesis and osteogenesis: EGR3, ESR1, GATA1/2/3, GLI2, NFATC1, PAX9, RB1, SOX6, SP1, STAT1 • Neural stem cell maintenance and differentiation: ATF2, CREB1, FOSB, FOXO3, HES1, HOXD10, MCM2/7, MEF2C, NEUROD1/G1, OLIG1/2, PAX3/6, POU4F1, PPARG, SMAD3/4, SNAI1, STAT3 Note : all gene names follow their official symbols by the Human Genome Organization Gene Nomenclature Committee (HGNC). GeneQuery™ qPCR array kits are qPCR ready in a 96-well plate format, with each well containing one primer set that can specifically recognize and efficiently amplify a target gene's cDNA. The carefully designed primers ensure that: (i) the optimal annealing temperature in qPCR analysis is 65°C (with 2 mM Mg 2+ , and no DMSO); (ii) the primer set recognizes all known transcript variants of target gene, unless otherwise indicated; and (iii) only one gene is amplified. -

Epigenetic Therapy Restores Normal Hematopoiesis in a Zebrafish Model
Leukemia (2015) 29, 2086–2097 © 2015 Macmillan Publishers Limited All rights reserved 0887-6924/15 www.nature.com/leu ORIGINAL ARTICLE Epigenetic therapy restores normal hematopoiesis in a zebrafish model of NUP98–HOXA9-induced myeloid disease AP Deveau1,2,15, AM Forrester1,2,15, AJ Coombs2,3, GS Wagner2,3, C Grabher4,5, IC Chute6, D Léger6, M Mingay7, G Alexe4,8, V Rajan1,2, R Liwski9,10, M Hirst7,11, K Steigmaier4,8, SM Lewis1,6,12,13, AT Look4 and JN Berman1,2,10,14 Acute myeloid leukemia (AML) occurs when multiple genetic aberrations alter white blood cell development, leading to hyperproliferation and arrest of cell differentiation. Pertinent animal models link in vitro studies with the use of new agents in clinical trials. We generated a transgenic zebrafish expressing human NUP98–HOXA9 (NHA9), a fusion oncogene found in high-risk AML. Embryos developed a preleukemic state with anemia and myeloid cell expansion, and adult fish developed a myeloproliferative neoplasm (MPN). We leveraged this model to show that NHA9 increases the number of hematopoietic stem cells, and that oncogenic function of NHA9 depends on downstream activation of meis1, the PTGS/COX pathway and genome hypermethylation through the DNA methyltransferase, dnmt1. We restored normal hematopoiesis in NHA9 embryos with knockdown of meis1 or dnmt1, as well as pharmacologic treatment with DNA (cytosine-5)-methyltransferase (DNMT) inhibitors or cyclo-oxygenase (COX) inhibitors. DNMT inhibitors reduced genome methylation to near normal levels. Strikingly, we discovered synergy when we combined sub-monotherapeutic doses of a histone deacetylase inhibitor plus either a DNMT inhibitor or COX inhibitor to block the effects of NHA9 on zebrafish blood development. -

Cell-Extrinsic Differentiation Block Mediated by Epha3 in Pre-Leukaemic Thymus Contributes to Disease Progression
cancers Article Cell-Extrinsic Differentiation Block Mediated by EphA3 in Pre-Leukaemic Thymus Contributes to Disease Progression Adriana C. Pliego Zamora 1 , Hansini Ranasinghe 1, Jessica E. Lisle 1, Chun Ki Ng 1, Stephen Huang 1, Racheal Wadlow 1, Andrew M. Scott 2,3, Andrew W. Boyd 4 and Christopher I. Slape 1,* 1 The University of Queensland Diamantina Institute, The University of Queensland, Brisbane 4102, Australia; [email protected] (A.C.P.Z.); [email protected] (H.R.); [email protected] (J.E.L.); [email protected] (C.K.N.); [email protected] (S.H.); [email protected] (R.W.) 2 Olivia Newton-John Cancer Research Institute and La Trobe University, Heidelberg 3084, Australia; [email protected] 3 Faculty of Medicine, University of Melbourne, Melbourne 3000, Australia 4 Department of Medicine, The University of Queensland, Brisbane 4072, Australia; [email protected] * Correspondence: [email protected] Simple Summary: The NUP98-HOXD13 (NHD13) mouse is a model of T-cell leukaemia (T-ALL) featuring a pre-leukemic phase, in which T-cell progenitors from the thymus of an NHD13 mouse can engraft into the thymus of a recipient mouse—an ability that normal T-cell progenitors do not possess. However, loss of this engraftment ability (by deletion of the Lyl1 gene) did not result in any loss of leukemogenesis activity, indicating the activity of redundant oncogenic pathways in this NHD13 model. Having observed an overexpression of the EphA3 protein in the thymocytes, we hypothesized that this gene might be involved in a redundant leukaemogenic pathway. -

A Synthetic CPP33-Conjugated HOXA9 Active Domain Peptide Inhibits Invasion Ability of Non-Small Lung Cancer Cells
biomolecules Article A Synthetic CPP33-Conjugated HOXA9 Active Domain Peptide Inhibits Invasion Ability of Non-Small Lung Cancer Cells 1, , 2,3, 1 1,4 1 Seong-Lan Yu * y, Han Koo y , Se-In Lee , JaeKu Kang , Young-Hyun Han , Young Il Yeom 2,3 and Dong Chul Lee 2,* 1 Priority Research Center, Myunggok Medical Research Institute, College of Medicine, Konyang University, Daejeon 35365, Korea; [email protected] (S.-I.L.); [email protected] (J.K.); [email protected] (Y.-H.H.) 2 Personalized Genomic Medicine Research Center, Korea Research Institute of Bioscience and Biotechnology (KRIBB), Daejeon 34141, Korea; [email protected] (H.K.); [email protected] (Y.I.Y.) 3 Department of Functional Genomics, University of Science and Technology (UST), Daejeon 34113, Korea 4 Department of Pharmacology, College of Medicine, Konyang University, Daejeon 35365, Korea * Correspondence: [email protected] (S.-L.Y.); [email protected] (D.C.L.) These authors contributed equally to this work. y Received: 7 October 2020; Accepted: 19 November 2020; Published: 23 November 2020 Abstract: Homeobox A9 (HOXA9) expression is associated with the aggressive growth of cancer cells and poor prognosis in lung cancer. Previously, we showed that HOXA9 can serve as a potential therapeutic target for the treatment of metastatic non-small cell lung cancer (NSCLC). In the present study, we have carried out additional studies toward the development of a peptide-based therapeutic agent. Vectors expressing partial DNA fragments of HOXA9 were used to identify a unique domain involved in the inhibition of NSCLC cell invasion. -

Frequent Co-Expression of the HOXA9 and MEIS1 Homeobox Genes in Human Myeloid Leukemias
Leukemia (1999) 13, 1993–1999 1999 Stockton Press All rights reserved 0887-6924/99 $15.00 http://www.stockton-press.co.uk/leu Frequent co-expression of the HOXA9 and MEIS1 homeobox genes in human myeloid leukemias HJ Lawrence1, S Rozenfeld1, C Cruz1, K Matsukuma1, A Kwong1,LKo¨mu¨ves1, AM Buchberg2 and C Largman1 1Division of Hematology and Medical Oncology, Department of Medicine, University of California VA Medical Center, San Francisco, CA; and 2Kimmel Cancer Center, Jefferson Medical College, Philadelphia, PA, USA There is increasing evidence that HOX homeobox genes play these leukemias.12 Recent work has shown that the engine- a role in leukemogenesis. Recent studies have demonstrated ered co-expression of the Hoxa-9 and Meis1 genes in murine that enforced co-expression of HOXA9 and MEIS1 in murine 13 marrow leads to rapid development of myeloid leukemia, and hematopoietic cells leads to rapid development of AML, that these proteins exhibit cooperative DNA binding. However, indicating a synergy between the two genes and suggesting it is unclear whether co-activation of HOXA9 and MEIS genes that co-activation of these genes is sufficient for transform- is a common occurrence in human leukemias. We surveyed ation. expression of HOXA9 and MEIS1 in 24 leukemic cell lines and We have recently demonstrated that HOXA9 and HOXA10 80 patient samples, using RNase protection analyses and proteins can interact with the MEIS1 protein and stabilize immunohistochemistry. We demonstrate that the expression of 14 HOXA9 and MEIS1 in leukemia cells is uniquely myeloid, and MEIS1-DNA interactions on consensus binding sites. These that these genes are commonly co-expressed in myeloid cell data support the notion that the leukemogenicity of the lines and in samples of acute myelogenous leukemia (AML) of HOXA9 and MEIS1 genes is related to the concerted actions all subtypes except in promyelocytic leukemia. -

Supplemental Information Jmjd1c Is Required for MLL-AF9 and HOXA9
Supplemental Information Jmjd1c is Required for MLL-AF9 and HOXA9 Mediated AML Stem Cell Self- Renewal Nan Zhu, Mo Chen, Rowena Eng, Joshua DeJong, Amit U. Sinha, Noushin F. Rahnamay, Richard Koche, Fatima Al-Shahrour, Janna C. Minehart, Chun-Wei Chen, Aniruddha J. Deshpande, Haiming Xu, S. Haihua Chu, Benjamin L. Ebert, Robert G. Roeder, Scott A. Armstrong Inventory of Supplemental Information Supplemental Figure Legends Supplemental Figures Figure S1. Related to Figure 1. Figure S2. Related to Figure 2&4. Figure S3. Related to Figure 3&5. Figure S4. Related to Figure 6. Figure S5. Related to Figure 7. Figure S6. Related to Figure 7. Supplemental Tables Table S1. Related to Figure 1. Table S2. Related to Figure 1. Table S3. Related to Figure S2 Table S4. Related to Figure 3. Table S5. Related to Figure 5. Table S6. Related to Figure 7. Figure S1 A B Number of Illumina reads C Log2(Median Fold Change Bone Marrow vs. T0) Spleen vs. T0) Spleen vs. (Median Fold Change (Median Fold 2 Relative R2=0.89 Log Row min Row max D HOXA9 HOXA10 MLL t (8;21) t (15;17) Adult Inv 16 M7 other T_MLL JMJD1C MEIS1 SENP6 TSC22D2 HIPK3 HOXA7 CDK6 RDX WNK1 PHIP CHD2 PDE3B -2.5 +3 RUNX2 Hoxa9 probe 1 Hoxa9 probe 2 Row relative Figure S1. In vivo shRNA screen of MLL-AF9 targets. Related to Figure 1. (A) Number of reads obtained from Illumina sequencing of eight experimental replicates. (B) Unsupervised hierarchical clustering of normalized reads of all hairpins in eight replicates. Hairpins are ranked by their depletion level in the bone marrow using log2 median fold- change. -

Down-Regulation of Homeobox Genes MEIS1 and HOXA in MLL-Rearranged Acute Leukemia Impairs Engraftment and Reduces Proliferation
Down-regulation of homeobox genes MEIS1 and HOXA in MLL-rearranged acute leukemia impairs engraftment and reduces proliferation Kira Orlovskya, Alexander Kalinkovichb,1, Tanya Rozovskaiaa,1, Elias Shezenb, Tomer Itkinb, Hansjuerg Alderc, Hatice Gulcin Ozerd, Letizia Carramusaa, Abraham Avigdore, Stefano Voliniac, Arthur Buchbergf, Alex Mazog, Orit Kolletb, Corey Largmanh,2, Carlo M. Crocec,3, Tatsuya Nakamurac, Tsvee Lapidotb, and Eli Canaania,3 Departments of aMolecular Cell Biology and bImmunology, Weizmann Institute of Science, Rehovot, 76100 Israel; Departments of cMolecular Virology, Immunology and Medical Genetics and dBiomedical Informatics, Comprehensive Cancer Center, Ohio State University, Columbus, OH 43210; eHematology Division, Sheba Medical Center, Tel-Hashomer, 52621, Israel; Departments of fMicrobiology and Immunology and gBiochemistry and Molecular Biology, Thomas Jefferson University, Philadelphia, PA 19107; and hVeteran Affairs Medical Center, San Francisco, CA 94121 Contributed by Carlo M. Croce, March 24, 2011 (sent for review January 31, 2011) Rearrangements of the MLL (ALL1) gene are very common in acute some translocation and MLL-AF4 (12). Subsequent gene ex- infant and therapy-associated leukemias. The rearrangements un- pression profiling of leukemic cells with MLL rearrangements derlie the generation of MLL fusion proteins acting as potent on- from patients showed up-regulation of MEIS1 and HOXA5– cogenes. Several most consistently up-regulated targets of MLL HOXA10, as well as other genes (13–15). Recently, application fusions, MEIS1, HOXA7, HOXA9, and HOXA10 are functionally re- of ChIP-seq determined that MEIS1, HOXA7, HOXA9, and lated and have been implicated in other types of leukemias. Each HOXA10 are among the 226 primary targets of MLL-AF4 in a of the four genes was knocked down separately in the human human ALL cell line (8).