Oxidative Damage to Dna in Alzheimer's Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Proteomic Identification of the Transcription Factors Ikaros And
European School of Molecular Medicine (SEMM) University of Milan and University of Naples “Federico II” PhD degree in Systems Medicine (curriculum in Molecular Oncology) Settore disciplinare: BIO/11 Proteomic identification of the transcription factors Ikaros and Aiolos as new Myc interactors on chromatin Chiara Veronica Locarno Matricola: R10755 Center for Genomic Science IIT@SEMM, Milan Supervisor: Bruno Amati, PhD IEO, Milan Added Supervisor: Arianna Sabò, PhD IEO, Milan Academic year 2017-2018 Table of contents List of abbreviations ........................................................................................................... 4 List of figures ....................................................................................................................... 8 List of tables ....................................................................................................................... 11 Abstract .............................................................................................................................. 12 1. INTRODUCTION ......................................................................................................... 13 1.1 Myc ........................................................................................................................................ 13 1.1.1 Myc discovery and structure ........................................................................................... 13 1.1.2. Role of Myc in physiological and pathological conditions ........................................... -

NBN Gene Analysis and It's Impact on Breast Cancer
Journal of Medical Systems (2019) 43: 270 https://doi.org/10.1007/s10916-019-1328-z IMAGE & SIGNAL PROCESSING NBN Gene Analysis and it’s Impact on Breast Cancer P. Nithya1 & A. ChandraSekar1 Received: 8 March 2019 /Accepted: 7 May 2019 /Published online: 5 July 2019 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Single Nucleotide Polymorphism (SNP) researches have become essential in finding out the congenital relationship of structural deviations with quantitative traits, heritable diseases and physical responsiveness to different medicines. NBN is a protein coding gene (Breast Cancer); Nibrin is used to fix and rebuild the body from damages caused because of strand breaks (both singular and double) associated with protein nibrin. NBN gene was retrieved from dbSNP/NCBI database and investigated using computational SNP analysis tools. The encrypted region in SNPs (exonal SNPs) were analyzed using software tools, SIFT, Provean, Polyphen, INPS, SNAP and Phd-SNP. The 3’ends of SNPs in un-translated region were also investigated to determine the impact of binding. The association of NBN gene polymorphism leads to several diseases was studied. Four SNPs were predicted to be highly damaged in coding regions which are responsible for the diseases such as, Aplastic Anemia, Nijmegan breakage syndrome, Microsephaly normal intelligence, immune deficiency and hereditary cancer predisposing syndrome (clivar). The present study will be helpful in finding the suitable drugs in future for various diseases especially for breast cancer. Keywords NBN . Single nucleotide polymorphism . Double strand breaks . nsSNP . Associated diseases Introduction NBN has a more complex structure due to its interaction with large proteins formed from the ATM gene which is NBN (Nibrin) is a protein coding gene, it is also known as highly essential in identifying damaged strands of DNA NBS1, Cell cycle regulatory Protein P95, is situated on and facilitating their repair [1]. -

Association of Gene Ontology Categories with Decay Rate for Hepg2 Experiments These Tables Show Details for All Gene Ontology Categories
Supplementary Table 1: Association of Gene Ontology Categories with Decay Rate for HepG2 Experiments These tables show details for all Gene Ontology categories. Inferences for manual classification scheme shown at the bottom. Those categories used in Figure 1A are highlighted in bold. Standard Deviations are shown in parentheses. P-values less than 1E-20 are indicated with a "0". Rate r (hour^-1) Half-life < 2hr. Decay % GO Number Category Name Probe Sets Group Non-Group Distribution p-value In-Group Non-Group Representation p-value GO:0006350 transcription 1523 0.221 (0.009) 0.127 (0.002) FASTER 0 13.1 (0.4) 4.5 (0.1) OVER 0 GO:0006351 transcription, DNA-dependent 1498 0.220 (0.009) 0.127 (0.002) FASTER 0 13.0 (0.4) 4.5 (0.1) OVER 0 GO:0006355 regulation of transcription, DNA-dependent 1163 0.230 (0.011) 0.128 (0.002) FASTER 5.00E-21 14.2 (0.5) 4.6 (0.1) OVER 0 GO:0006366 transcription from Pol II promoter 845 0.225 (0.012) 0.130 (0.002) FASTER 1.88E-14 13.0 (0.5) 4.8 (0.1) OVER 0 GO:0006139 nucleobase, nucleoside, nucleotide and nucleic acid metabolism3004 0.173 (0.006) 0.127 (0.002) FASTER 1.28E-12 8.4 (0.2) 4.5 (0.1) OVER 0 GO:0006357 regulation of transcription from Pol II promoter 487 0.231 (0.016) 0.132 (0.002) FASTER 6.05E-10 13.5 (0.6) 4.9 (0.1) OVER 0 GO:0008283 cell proliferation 625 0.189 (0.014) 0.132 (0.002) FASTER 1.95E-05 10.1 (0.6) 5.0 (0.1) OVER 1.50E-20 GO:0006513 monoubiquitination 36 0.305 (0.049) 0.134 (0.002) FASTER 2.69E-04 25.4 (4.4) 5.1 (0.1) OVER 2.04E-06 GO:0007050 cell cycle arrest 57 0.311 (0.054) 0.133 (0.002) -

HSP90 Regulates DNA Repair Via the Interaction Between XRCC1 and DNA Polymerase &Beta
ARTICLE Received 30 Oct 2013 | Accepted 7 Oct 2014 | Published 26 Nov 2014 DOI: 10.1038/ncomms6513 HSP90 regulates DNA repair via the interaction between XRCC1 and DNA polymerase b Qingming Fang1,2,w, Burcu Inanc3, Sandy Schamus2, Xiao-hong Wang2, Leizhen Wei2,4, Ashley R. Brown2, David Svilar1,2, Kelsey F. Sugrue2,w, Eva M. Goellner1,2,w, Xuemei Zeng5, Nathan A. Yates2,5,6, Li Lan2,4, Conchita Vens3,7 & Robert W. Sobol1,2,8,w Cellular DNA repair processes are crucial to maintain genome stability and integrity. In DNA base excision repair, a tight heterodimer complex formed by DNA polymerase b (Polb) and XRCC1 is thought to facilitate repair by recruiting Polb to DNA damage sites. Here we show that disruption of the complex does not impact DNA damage response or DNA repair. Instead, the heterodimer formation is required to prevent ubiquitylation and degradation of Polb. In contrast, the stability of the XRCC1 monomer is protected from CHIP-mediated ubiquitylation by interaction with the binding partner HSP90. In response to cellular pro- liferation and DNA damage, proteasome and HSP90-mediated regulation of Polb and XRCC1 alters the DNA repair complex architecture. We propose that protein stability, mediated by DNA repair protein complex formation, functions as a regulatory mechanism for DNA repair pathway choice in the context of cell cycle progression and genome surveillance. 1 Department of Pharmacology & Chemical Biology, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania 15213, USA. 2 Hillman Cancer Center, University of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania 15213, USA. 3 The Netherlands Cancer Institute, Division of Biological Stress Response, Amsterdam 1006BE, The Netherlands. -

DNA Related Enzymes As Molecular Targets for Antiviral and Antitumor- Al Chemotherapy
Send Orders for Reprints to [email protected] Current Drug Targets, 2018, 19, 000-000 1 REVIEW ARTICLE DNA Related Enzymes as Molecular Targets for Antiviral and Antitumor- al Chemotherapy. A Natural Overview of the Current Perspectives Hugo A. Garro* and Carlos R. Pungitore INTEQUI-CONICET, Fac. Qca., Bioqca. y Fcia., Univ. Nac. de San Luis (U.N.S.L), Chacabuco y Pedernera, 5700 San Luis, Argentina Abstract: Background: The discovery of new chemotherapeutic agents still remains a continuous goal to achieve. DNA polymerases and topoisomerases act in nucleic acids metabolism modulating different processes like replication, mitosis, damage repair, DNA topology and transcription. It has been widely documented that Polymerases serve as molecular targets for antiviral and antitumoral chemotherapy. Furthermore, telomerase is a ribonucleoprotein with exacerbated activity in most of the tumor cell lines, becoming as an emergent target in Cancer treatment. A R T I C L E H I S T O R Y Methods: We undertook an exhaustive search of bibliographic databases for peer-reviewed research literature related to the last decade. The characteristics of screened bibliography describe structure ac- Received: February 05, 2018 Revised: April 17, 2018 tivity relationships and show the principal moieties involved. This work tries to summarize the inves- Accepted: April 19, 2018 tigation about natural and semi-synthetic products with natural origin with the faculty to inhibit key DOI: enzymes that play a crucial role in DNA metabolism. 10.2174/1389450119666180426103558 Results: Eighty-five data references were included in this review, showing natural products widely distributed throughout the plant kingdom and their bioactive properties such as tumor growing inhibi- tory effects, and anti-AIDS activity. -

DNA Polymerase Beta Overexpression Correlates with Poor Prognosis in Esophageal Cancer Patients
Article Preclinical Medicine September 2013 Vol.58 No.26: 32743279 doi: 10.1007/s11434-013-5956-2 DNA polymerase beta overexpression correlates with poor prognosis in esophageal cancer patients ZHENG Hong1†, XUE Peng1†, LI Min2, ZHAO JiMin2, DONG ZiMing2* & ZHAO GuoQiang2* 1 Department of Pathophysiology, Medical College of Henan University, Kaifeng 475004, China; 2 School of Basic Medical Sciences, Zhengzhou University, Zhengzhou 450001, China Received March 26, 2013; accepted May 17, 2013; published online July 17, 2013 Gene of DNA polymerase beta (pol) plays an important role in base excision repair, DNA replication and translesion synthesis. This study aims to investigate the expression and prognostic significance of DNA pol in esophageal cancer. DNA pol expres- sion was analyzed using real-time quantitative PCR (RT-qPCR) and immunohistochemical staining on tissue samples from a consecutive series of 114 esophageal squamous carcinoma patients who underwent resections between 2002 and 2006. Pol ex- pression was investigated on its correlation to clinico-pathological factors and survival. RT-qPCR results showed higher expres- sion of DNA pol mRNA in tumor tissue than in its matched adjacent non-tumor tissue sample, different expression of DNA pol mRNA was noticed with significance between tumors with and without lymph node metastasis. Immunohistochemistry staining results indicated the pol strong-positive rate was 44.73% (51/114) in tumor tissue samples and 0.00% in matched adjacent non-tumor tissue samples, with significant difference. Kaplan-Meier survival curves revealed that high expression of pol was associated with tumor metastasis and poor prognosis in esophageal cancer patients. Our data suggests that pol plays an important role in tumor progression and that high pol expression predicts an unfavorable prognosis in esophageal squamous carcinoma patients. -
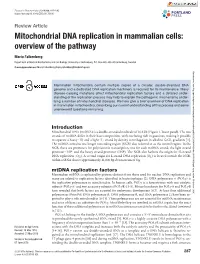
Mitochondrial DNA Replication in Mammalian Cells: Overview of the Pathway
Essays in Biochemistry (2018) 62 287–296 https://doi.org/10.1042/EBC20170100 Review Article Mitochondrial DNA replication in mammalian cells: overview of the pathway Maria Falkenberg Department of Medical Biochemistry and Cell Biology, University of Gothenburg, P.O. Box 440, 405 30 Gothenburg, Sweden Correspondence: Maria Falkenberg ([email protected]) Downloaded from http://portlandpress.com/essaysbiochem/article-pdf/62/3/287/486690/ebc-2017-0100c.pdf by guest on 05 October 2020 Mammalian mitochondria contain multiple copies of a circular, double-stranded DNA genome and a dedicated DNA replication machinery is required for its maintenance. Many disease-causing mutations affect mitochondrial replication factors and a detailed under- standing of the replication process may help to explain the pathogenic mechanisms under- lying a number of mitochondrial diseases. We here give a brief overview of DNA replication in mammalian mitochondria, describing our current understanding of this process and some unanswered questions remaining. Introduction MitochondrialDNA (mtDNA) is a double-stranded moleculeof16.6 kb (Figure 1, lower panel). The two strandsofmtDNA differ in their base composition, with one being rich in guanines, making it possible to separate a heavy (H)and a light (L) strand by density centrifugation in alkaline CsCl2 gradients [1]. The mtDNA contains one longer noncoding region (NCR) also referred to as the control region. Inthe NCR, there are promoters for polycistronic transcription, one for each mtDNA strand; the light strand promoter (LSP) and the heavy strand promoter (HSP). The NCRalso harbors the origin for H-strand DNA replication (OH). A second origin for L-strandDNA replication (OL)islocated outsidetheNCR, withinatRNAcluster approximately 11,000 bp downstream of OH. -

Post-Translational Modification of MRE11: Its Implication in DDR And
G C A T T A C G G C A T genes Review Post-Translational Modification of MRE11: Its Implication in DDR and Diseases Ruiqing Lu 1,† , Han Zhang 2,† , Yi-Nan Jiang 1, Zhao-Qi Wang 3,4, Litao Sun 5,* and Zhong-Wei Zhou 1,* 1 School of Medicine, Sun Yat-Sen University, Shenzhen 518107, China; [email protected] (R.L.); [email protected] (Y.-N.J.) 2 Institute of Medical Biology, Chinese Academy of Medical Sciences and Peking Union Medical College; Kunming 650118, China; [email protected] 3 Leibniz Institute on Aging–Fritz Lipmann Institute (FLI), 07745 Jena, Germany; zhao-qi.wang@leibniz-fli.de 4 Faculty of Biological Sciences, Friedrich-Schiller-University of Jena, 07745 Jena, Germany 5 School of Public Health (Shenzhen), Sun Yat-Sen University, Shenzhen 518107, China * Correspondence: [email protected] (L.S.); [email protected] (Z.-W.Z.) † These authors contributed equally to this work. Abstract: Maintaining genomic stability is vital for cells as well as individual organisms. The meiotic recombination-related gene MRE11 (meiotic recombination 11) is essential for preserving genomic stability through its important roles in the resection of broken DNA ends, DNA damage response (DDR), DNA double-strand breaks (DSBs) repair, and telomere maintenance. The post-translational modifications (PTMs), such as phosphorylation, ubiquitination, and methylation, regulate directly the function of MRE11 and endow MRE11 with capabilities to respond to cellular processes in promptly, precisely, and with more diversified manners. Here in this paper, we focus primarily on the PTMs of MRE11 and their roles in DNA response and repair, maintenance of genomic stability, as well as their Citation: Lu, R.; Zhang, H.; Jiang, association with diseases such as cancer. -

Transcriptome-Guided Characterization of Genomic Rearrangements in a Breast Cancer Cell Line
Transcriptome-guided characterization of genomic rearrangements in a breast cancer cell line Qi Zhaoa,1, Otavia L. Caballerob,1, Samuel Levya, Brian J. Stevensonc, Christian Iselic, Sandro J. de Souzad, Pedro A. Galanted, Dana Busama, Margaret A. Levershae, Kalyani Chadalavadae, Yu-Hui Rogersa, J. Craig Ventera,2, Andrew J. G. Simpsonb,2, and Robert L. Strausberga,2 aJ. Craig Venter Institute, 9704 Medical Center Drive, Rockville, MD 20850; bLudwig Institute for Cancer Research, New York, NY 10021; cLudwig Institute for Cancer Research, 1015 Lausanne, Switzerland; dLudwig Institute for Cancer Research, CEP 01509-010 Sao Paulo, Brazil; and eMemorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10065 Contributed by J. Craig Venter, December 22, 2008 (sent for review December 1, 2008) We have identified new genomic alterations in the breast cancer per cell (see Fig. 2A). The SKY analysis also reveals a large cell line HCC1954, using high-throughput transcriptome sequenc- number of translocations involving most or all chromosomes. ing. With 120 Mb of cDNA sequences, we were able to identify Using 454-FLX pyrosequencing we generated 510,703 cDNA genomic rearrangement events leading to fusions or truncations of sequences of average length 245 bp from the HCC1954 cell line. genes including MRE11 and NSD1, genes already implicated in (See Methods and Fig. S1). We then initially aligned all cDNA oncogenesis, and 7 rearrangements involving other additional sequences to RefSeq mRNAs (GenBank dataset available on genes. This approach demonstrates that high-throughput tran- March 28, 2008), revealing that Ͼ384,900 reads were uniquely scriptome sequencing is an effective strategy for the characteriza- associated well with 9,221 RefSeq genes. -

(NCCN V1.2020) RAD50 Mutations Cancer Risks and General
Updated December 2019 (NCCN v1.2020) RAD50 Mutations Cancer Risks and General Management Recommendations There are currently no national consensus guidelines outlining specific clinical management recommendations for individuals who carry a RAD50 gene mutation. Additionally, exact lifetime cancer risks associated with RAD50 mutations are unknown at this time. Some studies have proposed an increased risk for breast cancer in females with a RAD50 mutation (lifetime risk of ~24-36%).1-4 However, others have found no increased risk for breast cancer.5-7 Additionally, some studies have proposed an increased ovarian cancer risk in individuals with a RAD50 mutation.8,9 However, the studies are small, and data remains limited. At this time, it is unknown if individuals with RAD50 gene mutations are at increased risk for other cancers. Current NCCN guidelines assert that there is insufficient evidence to make any recommendations for breast MRI, risk-reducing mastectomy (RRM), or risk-reducing salpingo-oophorectomy (RRSO) based on RAD50 mutation status alone.10 An individual’s personal and family history should be considered in developing an appropriate surveillance plan. Implications for Family Members/Reproductive Considerations First-degree relatives (i.e., parents, siblings, and children) have a 50% chance to have the familial RAD50 mutation. Second-degree relatives (i.e., nieces/nephews, aunts/uncles, and grandparents) have a 25% chance to have the familial mutation. It has been proposed that individuals who inherit two pathogenic RAD50 mutations, one from each parent, are at risk for a rare genetic condition known as Nijmegen breakage syndrome-like disorder (NBSLD). o NBSLD is characterized by chromosomal instability, radiosensitivity, neurodevelopmental disease, and immunodeficiency11. -
Epigenetic Mechanisms Involved in the Cellular Response to DNA Damage Processed by Base Excision Repair
Epigenetic mechanisms involved in the cellular response to DNA damage processed by Base Excision Repair Thesis submitted in accordance with the requirements of the University of Liverpool for the degree of Doctor in Philosophy by Laura Gail Bennett November 2017 i Abstract Chromatin remodelling is required for access to occluded sequences of DNA by proteins involved in important biological processes, including DNA replication and transcription. There is an increasing amount of evidence for chromatin remodelling during DNA repair, although this has been mostly focused towards DNA double strand break and nucleotide excision repair. At this time there is little evidence for chromatin remodelling in base excision repair (BER). BER is a highly conserved DNA repair pathway which processes spontaneous endogenous DNA base damages generated by oxidative metabolism, but also those induced by exogenous agents (eg. ionising radiation), to maintain genome stability. The mechanism in which the BER repairs damaged bases has been extensively studied and the repair proteins involved are well known. However in terms of chromatin, BER is poorly understood. It is thought that chromatin remodelling occurs due to accumulating evidence indicating that certain BER enzymes are significantly less efficient at acting on sterically occluded sites and near the nucleosome dyad axis. At this time the mechanisms and enzymes involved to facilitate BER are unknown. Therefore, the study presented in this thesis aimed to identify specific histone modification enzymes and/or chromatin remodellers that are involved in the processing of DNA base damage during BER. A method to generate two mononucleosome substrates with a site specific synthetic AP site (tetrahydrofuran; THF) was used to measure recombinant AP endonuclease 1 (APE1) activity alone, and APE1 in HeLa whole cell extract (WCE) that contained chromatin modifiers. -

Structural and Functional Analysis of the Eukaryotic DNA Repair Proteins Mre11 and Nbs1
Dissertation zur Erlangung des Doktorgrades der Fakultät für Chemie und Pharmazie der Ludwig-Maximilians-Universität München Structural and functional analysis of the eukaryotic DNA repair proteins Mre11 and Nbs1 Christian Bernd Schiller aus Kassel 2011 Erklärung Diese Dissertation wurde im Sinne von § 13 Abs. 3 bzw. 4 der Promotionsordnung vom 29. Januar 1998 (in der Fassung der sechsten Änderungssatzung vom 16. August 2010) von Herrn Prof. Dr. Karl-Peter Hopfner betreut. Ehrenwörtliche Versicherung Diese Dissertation wurde selbständig, ohne unerlaubte Hilfe erarbeitet. München, am 07.06.2011 .................................................... (Christian Bernd Schiller) Dissertation eingereicht am 07.06.2011 1. Gutachter: Herr Prof. Dr. Karl-Peter Hopfner 2. Gutachter: Herr Prof. Dr. Dietmar Martin Mündliche Prüfung am 21.07.2011 During the work of this thesis, the following publication was published: Lammens K., Bemeleit D. J., Möckel C., Clausing E., Schele A., Hartung S., Schiller C. B., Lucas M., Angermüller C., Soding J., Strässer K. and K. P. Hopfner (2011). "The Mre11:Rad50 Structure Shows an ATP-Dependent Molecular Clamp in DNA Double-Strand Break Repair." Cell 145(1): 54-66. Parts of the present thesis will be submitted for publication: Schiller C.B., Lammens K., Guerini I., Coordes B., Schlauderer F., Möckel C., Schele A., Sträßer K., Jackson S. P., Hopfner K.-P.: “Insights into DNA double-strand break repair and ataxia-telangiectasia like disease from the structure of an Mre11-Nbs1 complex“, manuscript in preparation. Parts of this thesis have been presented at international conferences and workshops: Talk and poster at the Biannual International Meeting of the German Society of DNA Repair Research (DGDR) - Repair meets Replication, September 7-10, 2010 in Jena, Germany Poster presentation at the Gordon Research Conference on Mutagenesis - Consequences of Mutation and Repair for Human Disease, August 1-6, 2010 in Waterville, Maine, USA.