2020 Amendment to the Comprehensive Master Plan NIH Bethesda Campus January 13, 2020 Need for Projects
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Project Specifications
FOR BIDDING PURPOSES ONLY Project Specifications Fashion Institute of Technology Student Housing Corporation PROJECT: # C1331 PROJECT TITLE: ALUMNI RESIDENCE HALL CONCRETE ENCASED CONDUIT BANK OF IT AND RECONSTRUCTION OF EXTERIOR RAMP 210 WEST 27TH STREET NEW YORK, NY FIT STUDENT HOUSING CORPORATION PROJECT #C ALUMNI HALL CONCRETE ENCASED CONDUIT BANK OF IT AND RECONSTRUCTION OF EXTERIOR RAMP SPECIFICATION TABLE OF CONTENTS GENERAL CONSTRUCTION DIVISION 1 – GENERAL REQUIREMENTS 01 10 00 - SUMMARY OF WORK 01 33 00 - SUBMITTALS 01 73 29 - REMOVALS, CUTTING, AND PATCHING 01 74 19 - CONSTRUCTION WASTE MANAGEMENT DIVISION 2 – EXISTING CONDITIONS 02 08 30 - REMOVAL OF UNIVERSAL WASTE AND MISCELLANEOUS HAZARDOUS MATERIALS 02 33 13 – UNDERGROUND UTILITY LOCATOR SERVICE 02 41 13 - SELECTIVE REMOVALS & DEMOLITION DIVISION 3 – CONCRETE 03 11 00 – CONCRETE FORMWORK 03 20 00 – CONRETE REINFORCMENT 03 30 00 – CAST IN PLACE CONCRETE 03 45 00 – ARCHITECTURAL PRECAST CONCRETE TRIM DIVISION 4 – MASONRY 04 01 20 – UNIT MASONRY RESTORATION 04 01 21 – MASONRY RESTORATION 04 01 23 – MASONRY CLEANING 04 05 13 – MORTAR AND MASONRY GROUT 04 21 13 – BRICK MASONRY DIVISION 5 – METALS 05 51 20 - STRUCTURAL STEEL 05 52 00 – STRUCTURAL GLASS RAILING SYSTEM DIVISON 7 – THERMAL AND MOISTURE PROTECTION 07 60 00 – FLASHING & SHEET METAL DIVISON 26 – ELECTRICAL 26 05 29 – FASTENERS, ATTACHMENTS & SUPPORTING DEVICES 26 05 33 – RACEWAYS AND BOXES FOR ELECTRICAL SYSTEMS 26 05 43 – UNDERGROUND DUCTS AND RACEWAYS FOR ELECTRICAL SYSTEMS 26 05 44 – SLEEVES AND SLEEVE SEALS FOR ELECTRICAL RACEWAYS AND CABLING TABLE OF CONTENTS - 1 FIT STUDENT HOUSING CORPORATION PROJECT #C ALUMNI HALL CONCRETE ENCASED CONDUIT BANK OF IT AND RECONSTRUCTION OF EXTERIOR RAMP DIVISION 31 – EARTHWORK 31 00 00 – EARTHWORK 31 25 13 – EROSION AND SEDIMENT CONTROL 31 40 00 – SHORING AND UNDERPINNING DIVISON 32 – EXTERIOR IMPROVEMENTS 32 13 01 – CONCRETE WALKS 32 13 73 – CONCRETE PAVING JOINT SEALANTS DRAWING LIST ARCHITECTURAL 1. -

Public Realm Design Manual Version 2.1 March 2019
Public Realm Design Manual A Summary of District of Columbia Regulations and Specifications for the Design of Public Space Elements Government of the District of Columbia Version 2.1 - March 2019 Muriel Bowser, Mayor II Majestic views of national monuments, leafy residential streets, and wide sidewalks in commercial areas... these are iconic images of Washington, DC. Much of the daily routine of District residents, workers, and visitors takes place in settings like these. This is where we walk to school, wait for the bus, talk to neighbors, walk the dog, window shop, or sit outside in a café to drink a cup of coffee. Having such an extensive network of public space enhances the quality of life for our residents and visitors, and ensures that the city has the foundation to become a more walkable and sustainable city. The District’s public space is a valuable asset worthy of our stewardship and - with the help of all residents and property owners – is one if the unique features that makes our city great. The Guide to the District of Columbia’s Public Space Regulations is a resource for learning about the importance of the District’s public space, the regulations that guide its use and form, and the rationale behind them. Property owners are required to maintain the public space adjacent to their property, so it is important that these ideas are understood clearly. Beginning with the L’Enfant Plan and continuing to today, Washington, DC has a notable history of using public space to define the city and give character and grace to neighborhoods. -

Port of Tacoma Tacoma, Washington Washington United Terminal Utility Vault Upgrades
DIVISION 00 - PROCUREMENT AND CONTRACTING REQUIREMENTS SECTION 00 01 01 - PROJECT TITLE PAGE PORT OF TACOMA TACOMA, WASHINGTON WASHINGTON UNITED TERMINAL UTILITY VAULT UPGRADES PROJECT NO. 201090.01 CONTRACT NO. 071347 Trevor Thornsley, PE Director, Engineering Elly Bulega, PE Project Manager END OF PROJECT TITLE PAGE Project No. 201090.01 00 01 01 - 1 Contract No. 071347 • 02 41 10 Site Preparation • 03 30 00 Cast-In-Place Concrete • 33 01 00 Maintenance of Utilities DIVISION 00 - PROCUREMENT AND CONTRACTING REQUIREMENTS SECTION 00 01 10 - TABLE OF CONTENTS PROCUREMENT AND CONTRACTING REQUIREMENTS DIVISION 00 -- PROCUREMENT AND CONTRACTING REQUIREMENTS 00 01 01 - Project Title Page 00 01 07 - Seals Page 00 01 10 - Table of Contents 00 01 15 - List of Drawing Sheets 00 11 13 - Advertisement for Bids 00 21 00 - Instructions to Bidders 00 26 00 - Substitution Procedures 00 31 26 - Existing Hazardous Material Information 00 41 00 - Bid Form 00 43 13 - Bid Security Form 00 45 13 - Responsibility Detail Form 00 52 00 - Agreement Form 00 61 13.13 - Performance Bond 00 61 13.16 - Payment Bond 00 61 23 - Retainage Bond 00 61 23.13 - Retainage Escrow Agreement 00 72 00 - General Conditions 00 73 16 - Insurance Requirements 00 73 46 - Washington State Prevailing Wage Rates 00 73 63 - Security Requirements SPECIFICATIONS DIVISION 01 -- GENERAL REQUIREMENTS 01 10 00 - Summary 01 20 00 - Price and Payment Procedures 01 26 00 - Change Management Procedures 01 29 73 - Schedule of Values 01 30 00 - Administrative Requirements 01 31 23 - Web-based Construction Management 01 32 16 - Construction Progress Schedule 01 33 00 - Submittal Procedures 01 35 29 - Health, Safety, and Emergency Response Procedures Project No. -

Templeton Community Services District
PRELIMARY – NOT FOR CONSTRUCTION CITY OF MORRO BAY LIFT STATION #2 UPGRADE PROJECT NO. MB 2011 WWC-__ TECHNICAL SPECIFICATIONS PREPARED BY: WALLACE GROUP 612 CLARION COURT SAN LUIS OBISPO, CALIFORNIA 93401 THOMA ELECTRIC 3562 EMPLEO, SUITE C SAN LUIS OBISPO, CALIFORNIA 93401 JOB NO. 0032-0008 March 2011 TECHNICAL SPECIFICATIONS TABLE OF CONTENTS CITY OF MORRO BAY LIFT STATION 2 SPECIFICATIONS GROUP GENERAL REQUIREMENTS SUBGROUP Division 01 – General Requirements 01 11 00 Summary of Work 01 11 16 Work by Owner (Owner-Furnished/Contractor-Installed Equipment) 01 20 00 Price and Payment Procedures 01 30 00 Administrative Requirements 01 32 16 Construction Progress Schedule 01 33 00 Submittal Procedures 01 35 00 Special Project Procedures 01 50 00 Temporary Facilities and Controls 01 57 19 Construction Site Management 01 60 00 Product Requirements 01 70 00 Execution and Closeout Requirements 01 75 00 Starting and Adjusting FACILITY CONSTRUCTION SUBGROUP Division 02 – Existing Conditions 02 21 00 Surveys 02 42 00 Removal and Salvage of Construction Materials Division 03 – Concrete 03 30 00 Cast-in-Place Concrete 03 40 00 Precast Concrete Divisions 04, 06 and 07 – Not Used Division 05 Metals 05 52 00 Metal Safety Railing Division 08 Openings 08 31 13 Access Doors and Frames Division 09 – Finishes 09 90 00 Painting and Coating 09 97 23 Concrete and Masonry Coatings Divisions 10 to 12, 14 – Not Used Division 13 – Special Construction Section 13 34 00 Fabricated Engineered Structures Section 13 75 00 Chemical Storage Tanks WG 0032-0008 TABLE OF -

P Sol Winter 2012.Pdf
BOOTH 1736 WINTER 2012 A Magazine for Specifiers and Engineers VOLUME 10 | NUMBER 1 ON THE COVER: Designed by a team of architectural students for the New Jersey coast, this precast concrete solar home is not only energy efficient and technologically advanced, but will stand up to severe weather. 4 I PRECASTER’S NOTEBOOK: Photo by Ron Hyink. ANATOMY OF A DOGHOUSE MANHOLE Precast Solutions (ISSN 1934-4066 print, ISSN BY GARY K. MUNKELT, P.E. 1934-4074 online) is published quarterly by NPCA, the association of the manufactured concrete products industry. 6 I TAKING MOTHER Material in this publication may not be reproduced without written permission from NATURE’S WORST NPCA. Requests for permission should be Precast concrete evacuation building designs directed to the editor. stand up to tsunamis and tornados. DEBORAH R. HUSO © Copyright 2012 by NPCA. Publisher: Ty Gable Executive Editor: Bob Whitmore XTREME RECAST 10 I E P : Managing Editor: Ron Hyink FREEZING OUT THE COMPETITION Editor: Sue McCraven Five proud precasters reflect on their favorite cold-weather projects. Associate Editor: Kirk Stelsel BY SUE McCRAVEN Graphic Designer: Deborah Templeton Advertising: Brenda C. Ibitz Vice President of Development & Member Services (317) 571-9500 • (317) 571-9941 (fax) 16 I NOT YOUR TYPICAL [email protected] BEACH HOUSE NPCA A safe haven from the storm, this precast concrete solar home Precast Solutions exemplifies energy savings and modern architecture. 1320 City Center Dr., Suite 200 BY RON HYINK Carmel, IN 46032 (800) 366-7731 (317) 571-9500 (International) Fax: (317) 571-0041 22 I PRECAST BUILDINGS: E-mail: [email protected] INSTALL FAST AND BUILT TO LAST This publication is designed to provide accurate and authoritative information in regard to the subject matter covered; however, BY KIRK STELSEL National Precast Concrete Association and Precast Solutions act as mediators without approving, disapproving or guaranteeing the validity or accuracy of any data, claim or opinion appearing herein. -
Shallow SEM Tunneling with Limited Clearance to Existing Structures: Design, Construction and Observations
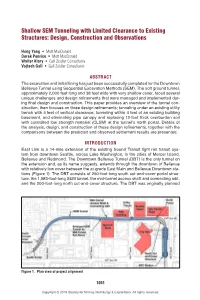
Shallow SEM Tunneling with Limited Clearance to Existing Structures: Design, Construction and Observations Hong Yang . Mott MacDonald Derek Penrice . Mott MacDonald Walter Klary . Gall Zeidler Consultants Vojtech Gall . Gall Zeidler Consultants ABSTRACT The excavation and initial lining has just been successfully completed for the Downtown Bellevue Tunnel using Sequential Excavation Methods (SEM). The soft ground tunnel, approximately 2,000 feet long and 38 feet wide with very shallow cover, faced several unique challenges and design refinements that were managed and implemented dur- ing final design and construction. This paper provides an overview of the tunnel con- struction, then focuses on three design refinements; tunneling under an existing utility trench with 4 feet of vertical clearance, tunneling within 4 feet of an existing building basement, and eliminating pipe canopy and replacing 12-foot thick overburden soil with controlled low strength material (CLSM) at the tunnel’s north portal. Details of the analysis, design, and construction of these design refinements, together with the comparisons between the predicted and observed settlement results are presented. INTRODUCTION East Link is a 14-mile extension of the existing Sound Transit light rail transit sys- tem from downtown Seattle, across Lake Washington, to the cities of Mercer Island, Bellevue and Redmond. The Downtown Bellevue Tunnel (DBT) is the only tunnel on the extension and, as its name suggests, extends through the downtown of Bellevue with relatively low cover between the at-grade East Main and Bellevue Downtown sta- tions (Figure 1). The DBT consists of 250-foot-long south cut-and-cover portal struc- ture, the 1,983-foot-long SEM tunnel, the mid-tunnel access shaft and connecting adit, and the 200-foot-long north cut-and-cover structure. -

St. Elizabeth's West Campus
St. Elizabeth’s West Campus Consulting Party Meeting November 9, 2010 Meeting Notes GSA ROB Room 7023 1:30 – 5:30pm I. Welcome and Introductions (CI International) Marc Gravallese (CI): Welcomed the group to the meeting. Group: (Participants introduced themselves. Attendance list attached.) II. Project Updates- Global Project Updates (GSA) Jim Fortinsky - GSA – Pile work is being done to support the U.S. Coast Guard Building and foundation work is being done throughout the building. Soil excavation has been completed and garages are being excavated. Slab and foundation work has been started on the north side of garage. The first six adaptive reuse buildings are being abated right now and upon completion will be turned over to Grunley Construction to start construction. Building abatement for the Phase 1 adaptive reuse buildings is anticipated to take 90 days. Utility tunnel work NTP is anticipated to occur in December and the Perimeter Security Fence NTP has been given to Balfour Beatty. We continue to coordinate work between Clark and Grunley. GSA has been directed not to open Gate 3 at this point, therefore, we are not moving forward with this piece at this time. As soon as the project team receives further guidance on this item we will discuss with the Consulting Parties. Pepco has begun bringing in their new electrical line right now. There is a lot of crossing of work in that area which requires a great deal of coordination. We are fencing up the protected landscape areas. We are also trying not to have too much activity on the site as we will be crowded in a very short period of time. -
Network Vault Design Guide
NASHVILLE ELECTRIC SERVICE VAULT DESIGN GUIDE (NETWORK) AUGUST 2021 0 NETWORK VAULT DESIGN GUIDE TABLE OF CONTENTS 1. PURPOSE ........................................................................................................................................................................................... 2 2. CUSTOMER RESPONSIBILITY..................................................................................................................................................... 2 3. DRAWINGS ........................................................................................................................................................................................ 3 PRELIMINARY DESIGN DRAWINGS .......................................................................................................................................................... 3 CONSTRUCTION/APPROVAL DRAWINGS .................................................................................................................................................. 3 AS-BUILT RECORD DRAWINGS .............................................................................................................................................................. 3 4. ARCHITECTURAL REQUIREMENTS ......................................................................................................................................... 4 VAULT INSPECTION AND ACCEPTANCE .................................................................................................................................................... -
A Case Study for Up-Down Design and Construction Methodology for a High-Rise Development in Los Angeles, California
SEAOC 2008 CONVENTION PROCEEDINGS A Case Study for Up-Down Design and Construction Methodology for a High-Rise Development in Los Angeles, California Jason Thompson, Associate KPFF Consulting Engineers Portland, Oregon Chris Zadoorian, Principal GeoDesign, Inc. Anaheim, California Abstract 60,000 square feet. It is anticipated for completion in 2008. The building footprint occupies the entire site and is rectangular in Over the past few years, numerous high-rise projects have been shape. It is bounded on the south and east sides by 12th Street initiated in downtown Los Angeles. In most cases, at least one and Grand Avenue, respectively; by an alleyway on the west and often two or more subterranean levels are constructed. side; and by a recently completed 11-story residential tower Conventional construction sequencing would consist of with one subterranean level, immediately to the north. See shoring installation, mass excavation, and construction of the Figure 1 below. below-grade structure all prior to construction of the building superstructure. For a high-rise project currently under construction in downtown Los Angeles, an alternative sequence, referred to as ‘up-down’ (or ‘top-down’) was used to reduce the duration of the overall construction schedule. Up-down sequencing typically allows the construction of the building superstructure in tandem with mass excavation and construction of the below-grade levels. The subject project includes a 23-story tower over three subterranean levels and has a building footprint of approximately 60,000 square feet. A modified up- down sequence was implemented in which the installation of basement walls and below-grade foundations and the initiation of superstructure preceded mass excavation and basement floor construction. -

Spokane Park Board Riverfront Park Committee Meeting Agenda of April
Meeting Notice/Agenda City of Spokane Park Board Riverfront Park Committee Monday, April 9, 2018, 8:05 am Conference Room 5A, 5th Floor City Hall 808 W. Spokane Falls Blvd., Spokane WA 99201 Riverfront Park Director Jonathan Moog Committee Members Other Park Board members: Ted McGregor – Chair Chris Wright Rick Chase Steve Salvatori Jennifer Ogden Gerry Sperling Jamie SiJohn A special meeting of the City of Spokane Riverfront Park Committee will be held at 8:05 a.m. Monday, April 9, 2018, Conference Room 5A, 5th floor City Hall, 808 W. Spokane Falls Blvd., Spokane, Washington. The meeting will be conducted in a standing committee format for the Riverfront Park Committee of the City of Spokane Park Board. Because a quorum of the Park Board may be present, the standing committee meeting will be conducted as a committee of the whole board. The meeting will be open to the public, with the possibility of moving into executive session only with the members of the Park Board and appropriate staff. Discussion will be limited to appropriate officials and staff. Public testimony may be taken at the discretion of the committee chair. Agenda Action Items: 1. Riverfront Park Committee Chair pro-tem selection – Chris Wright 2. Riverfront Park art plan, signature artwork design and siting recommendation – Meejin Yoon 3. Pavilion and Promenade GMP and design development – Clancy Welsh and Keith Comes 4. Visit Spokane Memorandum of Understanding/regional information center – Jonathan Moog 5. Historic Carousels, Inc., contract amendment and sole source resolution/Looff Carrousel ($25,000) – Jonathan Moog 6. Budget reallocation/North Butterfly design and construction ($117,500) – Berry Ellison 7. -
Right of Way Improvement Standards
RIGHT OF WAY IMPROVEMENT STANDARDS PHILADELPHIA STREETS DEPARTMENT Carlton Williams Commissioner Richard J. Montanez, P.E. Deputy Commissioner of Transportation Stephen Lorenz Chief Highway Engineer June 2015 Last Rev: N/A Forward Over the past several years, the Streets Department has undergone some transformative changes. From the Great Recession of 2008, we have entered into a time of major construction and development. With this “New Boom”, demands for a better understanding of the technical and regulatory requirements of the Department have grown dramatically. These demands have occurred concurrently with an increasing need for enforcement of Federal, and State laws, as well as a series of laws and initiatives adopted by the City of Philadelphia. In addition to seeking to fulfill the obligations defined within the Philadelphia Home Rule Charter, and the Philadelphia Code, the Streets Department has recognized the need to ensure compliance with the Americans with Disabilities Act (1990), and the Underground Utility Line Protection Act, PA Act 287 (1974, and as revised), all within a framework defined greatly by Philadelphia Code §11-900 (Complete Streets). The purpose of these Right of Way Improvement Standards is to gather the standard requirements of the Streets Department into a single source. Much of the content of this publication derive from established Streets Department resources, as well as standards established, or influenced, by our sister departments, and partners with the Commonwealth of Pennsylvania and the U.S. Government. As a living document, this Standard is subject to periodic revision, as the needs of this great City continue to grow, and new practices and technologies within our street network become available. -

Krs 278.042 Case No. 2013-00373
COMMONWEALTH OF KENTUCKY BEFORE THE PUBLIC SERVICE COMMISSION In the Matter of: LOUISVILLE GAS AND ELECTRIC ) COMPANY ) ) CASE NO. 2013-00373 ) ALLEGED FAILURE TO COMPLY WITH ) KRS 278.042 ) ORDER Louisville Gas and Electric Company ("LG&E"), a Kentucky corporation which engages in the distribution for compensation of gas and electricity to the public for heat, light, power, and other uses, is a utility subject to Commission jurisdiction." KRS 278.042 requires the Commission to ensure that each electric utility constructs and maintains its plant and facilities in accordance with accepted engineering practices as set forth in the Commission's administrative regulations and orders and in the most recent edition of the National Electrical Safety Code ("NESC"). KRS 278.030 requires every utility to furnish adequate, efficient, and reasonable service. KRS 278.260 permits the Commission, upon its own motion, to investigate any act or practice of a utility that affects or is related to the service of a utility. KRS 278.280(1) further permits the Commission, after conducting such investigation and finding that a practice is unreasonable, unsafe, improper, or inadequate to determine the reasonable, safe, proper, or adequate practice or methods to be observed and to fix same by Order. Pursuant to 278.280(2}, which directs the Commission to prescribe rules and regulations for the performance of services by utilities, the Commission has promulgated Administrative Regulation 807 KAR 5:006, Section 25, which requires all utilities to adopt and execute a safety program. 807 KAR 5:006, Section 25(1} requires each utility to establish a safety manual with written guidelines for safe working practices and procedures to be followed by utility employees.