Download Article PDF/Slides
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

HIV-Infected Patients
New Drugs for the Treatment-Experienced Patient Joseph Eron, md Associate Professor of Medicine and Director, Clinical Core unc Center for aids Research, University of North Carolina at Chapel Hill Summary by Tim Horn Edited by Jay Dobkin, md; Michael Saag, md reatment options for antiretro- humans by adenosine deaminase into D- Deeks and his colleagues in 1998 demon- viral-experienced patients leave a dioxolane guanine (dxg), a metabolite that strated a 1 log reduction in hiv-rna in hiv- lot to be desired. According to Dr. has potent activity against hiv and hbv. infected patients—more than 50% of whom Joe Eron, patients who have treat- According to in vitro data presented at were treatment-experienced—who received ment experience in all three classes the 3rd International Workshop on hiv tenofovir df 300 mg once daily as of currently available antiretrovi- Drug Resistance and Treatment Strategies, monotherapy for 28 days (Deeks, 1998). Trals have, at best, a 30% chance of re- held in June 1999, dapd was found to in- According to in vitro data presented by ducing their viral load to levels below 400 hibit wild-type and mutant isolates resistant Gilead’s Dr. Michael Miller at the recent copies/mL upon initiating a salvage regi- to azt (Retrovir) and 3TC (Borroto-Esoda, 4th International Resistance Workshop, the men. Cross-resistance within each class of 1999). The drug was also reported to be ac- resistance pattern for tenofovir df is simi- drugs, particularly the protease inhibitors tive against strains collected from patients lar to that of its chemical predecessor adefo- (pis) and non-nucleoside reverse tran- who have failed various nrti and nnrti vir, a compound no longer in development scriptase inhibitors (nnrtis), essentially combination therapies, including those for the treatment of hiv (Miller, 2000). -

Download Article PDF/Slides
Kan Lu, PharmD New Antiretrovirals for Based on a presentation at prn by Roy M. Gulick, md, mph the Treatment of HIV: Kan Lu, PharmD | Drug Development Fellow University of North Carolina School of Pharmacy Chapel Hill, North Carolina The View in 2006 Roy M. Gulick, md, mph Reprinted from The prn Notebook® | october 2006 | Dr. James F. Braun, Editor-in-Chief Director, Cornell Clinical Trials Unit | Associate Professor of Medicine, Meri D. Pozo, PhD, Managing Editor. Published in New York City by the Physicians’ Research Network, Inc.® Weill Medical College of Cornell University | New York, New York John Graham Brown, Executive Director. For further information and other articles available online, visit http://www.prn.org | All rights reserved. ©october 2006 substantial progress continues to be made in the arena of cokinetics and a long extracellular half-life of approximately 10 hours antiretroviral drug development. prn is again proud to present its annual (Zhu, 2003). During apricitabine’s development, a serious drug interac- review of the experimental agents to watch for in the coming months and tion with lamivudine (Epivir) was noted. Although the plasma years. This year’s review is based on a lecture by Dr. Roy M. Gulick, a long- concentrations of apricitabine were unaffected by coadministration of time friend of prn, and no stranger to the antiretroviral development lamivudine, the intracellular concentrations of apricitabine were reduced pipeline. by approximately sixfold. Additionally, the 50% inhibitory concentration To date, twenty-two antiretrovirals have been approved by the Food (ic50) of apricitabine against hiv with the M184V mutation was increased and Drug Administration (fda) for the treatment of hiv infection. -

(12) Patent Application Publication (10) Pub. No.: US 2016/0058872 A1 Crew Et Al
US 2016.0058872A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2016/0058872 A1 Crew et al. (43) Pub. Date: Mar. 3, 2016 (54) IMIDE-BASED MODULATORS OF A613 L/426 (2006.01) PROTEOLYSIS AND ASSOCATED METHODS A 6LX3 L/505 (2006.01) OF USE A613 L/454 (2006.01) A613 L/55 (2006.01) (71) Applicant: Arvinas, Inc., New Haven, CT (US) C07D40 L/4 (2006.01) A6II 45/06 (2006.01) (72) Inventors: Andrew P. Crew, Guilford, CT (US); (52) U.S. Cl. Craig Crews, New Haven, CT (US), CPC ............ A61K 47/481 (2013.01); C07D401/14 Hanging Dong, Madison, CT (US); Jing (2013.01); C07D 495/14 (2013.01); C07D Wang, Milford, CT (US); Yimin Qian, 417/14 (2013.01); A61K 45/06 (2013.01); Plainsboro, NJ (US); Kam Siu Milford, A6 IK3I/505 (2013.01); A61 K3I/454 CT (US); Meizhong Jin, East Northport, (2013.01); A61 K3I/551 (2013.01); A61 K NY (US) 3 1/426 (2013.01) (21) Appl. No.: 14/792,414 (57) ABSTRACT (22) Filed: Jul. 6, 2015 The description relates to imide-based compounds, including Related U.S. Application Data bifunctional compounds comprising the same, which find utility as modulators of targeted ubiquitination, especially (63) Continuation-in-part of application No. 14/686.640, inhibitors of a variety of polypeptides and other proteins filed on Apr. 14, 2015. which are degraded and/or otherwise inhibited by bifunc (60) Provisional application No. 61/979,351, filed on Apr. tional compounds according to the present invention. In par 14, 2014, provisional application No. -

Tim Horn Deputy Executive Director, HIV & HCV Programs Treatment
Tim Horn Deputy Executive Director, HIV & HCV Programs Treatment Action Group NASTAD Prevention and Care Technical Assistance Meeting Washington, DC July 19, 2017 ▪ Pipeline is robust! ▪ Several drugs, coformulations, and biologics in late-stage development and Phase I trials ▪ Trends are clear ▪ Maximizing safety and efficacy of three-drug regimens ▪ Validating two-drug regimens as durable maintenance therapy and, potentially, for PLWHIV starting treatment for the first time ▪ Advancing long-acting and extended release products ▪ Development new drugs and biologics for multi-drug/class-resistant HIV ▪ Cost considerations in high- and middle-income countries Compound Class/Type Company Status DRUGS Isentress HD INSTI Merck FDA Approved 5/30/17 Bictegravir plus TAF/FTC INSTI plus NtRTI & NRTI Gilead Phase III; mid-2018 approval Doravirine (plus TDF/3TC) NNRTI (plus NtRTI & NRTI) Merck Phase III; mid-2018 approval Darunavir plus cobicistat, PI plus PK booster, NtRTI & Janssen Phase III; mid-2018 approval TAF & FTC NRTI Dolutegravir plus rilpivirine INSTI plus NNRTI ViiV/Jansse Phase III; early 2018 approval n Dolutegravir plus lamivudine INSTI plus NRTI ViiV Phase III; late 2018 approval BIOLOGICS Ibalizumab Entry Inhibitor TaiMed Phase III; late 2017 or early Biologics 2018 Compound Class/Type Company Status DRUGS LA Cabotegravir + INSTI + NNRTI ViiV/ Phase III LA Rilpivirine Janssen Albuvirtide Fusion Inhibitor Frontier Phase III; China is primary Biologics launch target Fostemsavir CD4 attachment inhibitor ViiV Phase III Elsulfavirine -

Modifications to the Harmonized Tariff Schedule of the United States To
U.S. International Trade Commission COMMISSIONERS Shara L. Aranoff, Chairman Daniel R. Pearson, Vice Chairman Deanna Tanner Okun Charlotte R. Lane Irving A. Williamson Dean A. Pinkert Address all communications to Secretary to the Commission United States International Trade Commission Washington, DC 20436 U.S. International Trade Commission Washington, DC 20436 www.usitc.gov Modifications to the Harmonized Tariff Schedule of the United States to Implement the Dominican Republic- Central America-United States Free Trade Agreement With Respect to Costa Rica Publication 4038 December 2008 (This page is intentionally blank) Pursuant to the letter of request from the United States Trade Representative of December 18, 2008, set forth in the Appendix hereto, and pursuant to section 1207(a) of the Omnibus Trade and Competitiveness Act, the Commission is publishing the following modifications to the Harmonized Tariff Schedule of the United States (HTS) to implement the Dominican Republic- Central America-United States Free Trade Agreement, as approved in the Dominican Republic-Central America- United States Free Trade Agreement Implementation Act, with respect to Costa Rica. (This page is intentionally blank) Annex I Effective with respect to goods that are entered, or withdrawn from warehouse for consumption, on or after January 1, 2009, the Harmonized Tariff Schedule of the United States (HTS) is modified as provided herein, with bracketed matter included to assist in the understanding of proclaimed modifications. The following supersedes matter now in the HTS. (1). General note 4 is modified as follows: (a). by deleting from subdivision (a) the following country from the enumeration of independent beneficiary developing countries: Costa Rica (b). -

Reviewing HIV-1 Gag Mutations in Protease Inhibitors Resistance: Insights for Possible Novel Gag Inhibitor Designs
molecules Review Reviewing HIV-1 Gag Mutations in Protease Inhibitors Resistance: Insights for Possible Novel Gag Inhibitor Designs Chinh Tran-To Su 1, Darius Wen-Shuo Koh 1 and Samuel Ken-En Gan 1,2,* 1 Antibody & Product Development Lab, Bioinformatics Institute, A*STAR, Singapore 138671, Singapore 2 p53 Laboratory, A*STAR, Singapore 138648, Singapore * Correspondence: [email protected]; Tel.: +65-6478-8417; Fax: +65-6478-9047 Academic Editor: Keykavous Parang Received: 23 August 2019; Accepted: 4 September 2019; Published: 6 September 2019 Abstract: HIV protease inhibitors against the viral protease are often hampered by drug resistance mutations in protease and in the viral substrate Gag. To overcome this drug resistance and inhibit viral maturation, targeting Gag alongside protease rather than targeting protease alone may be more efficient. In order to successfully inhibit Gag, understanding of its drug resistance mutations and the elicited structural changes on protease binding needs to be investigated. While mutations on Gag have already been mapped to protease inhibitor resistance, there remain many mutations, particularly the non-cleavage mutations, that are not characterized. Through structural studies to unravel how Gag mutations contributes to protease drug resistance synergistically, it is thus possible to glean insights to design novel Gag inhibitors. In this review, we discuss the structural role of both novel and previously reported Gag mutations in PI resistance, and how new Gag inhibitors can be designed. Keywords: HIV-1 Gag; Gag inhibitors; protease; protease inhibitors; drug resistance mutations; drug design 1. Introduction Many anti-HIV drugs interfere directly with the viral life cycle by targeting key viral enzymes [1], e.g., reverse transcriptase inhibitors [2,3], integrase inhibitors [4,5], and protease inhibitors [6,7]. -
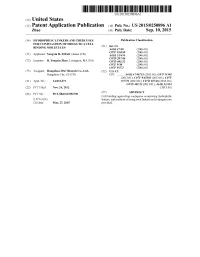
(12) Patent Application Publication (10) Pub. No.: US 2015/0250896 A1 Zhao (43) Pub
US 20150250896A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2015/0250896 A1 Zhao (43) Pub. Date: Sep. 10, 2015 (54) HYDROPHILIC LINKERS AND THEIR USES Publication Classification FOR CONUGATION OF DRUGS TO A CELL (51) Int. Cl BNDING MOLECULES A647/48 (2006.01) (71) Applicant: Yongxin R. ZHAO, Henan (CN) Ek E. 30.8 C07D 207/216 (2006.01) (72) Inventor: R. Yongxin Zhao, Lexington, MA (US) C07D 40/12 (2006.01) C07F 9/30 (2006.01) C07F 9/572 (2006.01) (73) Assignee: Hangzhou DAC Biotech Co., Ltd., (52) U.S. Cl. Hangzhou City, ZJ (CN) CPC ........... A61K47/48715 (2013.01); C07F 9/301 (2013.01); C07F 9/65583 (2013.01); C07F (21) Appl. No.: 14/432,073 9/5721 (2013.01); C07D 207/46 (2013.01); C07D 401/12 (2013.01); A61 K3I/454 (22) PCT Filed: Nov. 24, 2012 (2013.01) (86). PCT No.: PCT/B2O12/0567OO Cell(57) binding- agent-drugABSTRACT conjugates comprising hydrophilic- S371 (c)(1), linkers, and methods of using Such linkers and conjugates are (2) Date: Mar. 27, 2015 provided. Patent Application Publication Sep. 10, 2015 Sheet 1 of 23 US 2015/0250896 A1 O HMDS OSiMe 2n O Br H-B-H HPC 3 2 COOEt essiop-\5. E B to NH 120 °C, 2h OsiMe3 J 50 °C, 2h eSiO OEt 120 oC, sh 1 2 3. 42% from 1 Bra-11a1'oet - Brn 11-1 or a 1-1 or ÓH 140 °C ÓEt ÓEt 4 5 6 - --Messio. 8 B1a-Br aus 20 cc, hP-1}^-'ot Br1-Y. -

14-258 Phrma HIV/AIDS2014 0819.Indd
2014 MEDICINES IN DEVELOPMENT REPORT HIV/AIDS PRESENTED BY AMERICA’S BIOPHARMACEUTICAL RESEARCH COMPANIES Biopharmaceutical Company Researchers Are Developing More Than 40 Medicines and Vaccines For HIV Infection Treatment and Prevention Medicines and Vaccines in Globally, approximately 35 million people effective therapies, and preventative Development for HIV Infection are infected with human immunodefi - vaccines. These medicines and vaccines ciency virus (HIV), the virus that causes are either in clinical trials or awaiting Application acquired immune defi ciency syndrome review by the U.S. Food and Drug Submitted (AIDS). However, new infections have Administration (FDA). Phase III dropped by 38 percent since 2001, Phase II The 44 medicines and vaccines in the according to UNAIDS, the Joint United Phase I development pipeline include: Nations Programme on HIV/AIDS. • A fi rst-in-class medicine intended to In the United States, more than 25 prevent HIV from breaking through 1.1 million people are living with HIV the cell membrane. and 15.8 percent of those are unaware they are infected, according to the • A cell therapy that modifi es a U.S. Centers for Disease Control and patient’s own cells in an attempt to Prevention (CDC). Although the U.S. make them resistant to HIV. HIV/AIDS-related death rate has fallen 16 by more than 80 percent since the introduction of antiretroviral therapies in Contents 1995, new HIV infections have stabilized HIV Medicines and Vaccines in at approximately 50,000 each year, Development ......................................2 according to the CDC. Incremental Innovation in HIV/AIDS Treatment .......................... 4 Since AIDS was fi rst reported in 1981, Access to HIV/AIDS Medicines in nearly 40 medicines have been approved Exchange Plans ...................................5 to treat HIV infection in the United Facts About HIV/AIDS ........................7 States. -

This Project Has Been Supported with Unrestriced Grants from Abbvie Gilead Sciences HEXAL Janssen-Cilag MSD Viiv Healthcare By
This project has been supported with unrestriced grants from AbbVie Gilead Sciences HEXAL Janssen-Cilag MSD ViiV Healthcare By Marcus Altfeld, Hamburg/Boston (USA) Achim Barmeyer, Dortmund Georg Behrens, Hannover Dirk Berzow, Hamburg Christoph Boesecke, Bonn Patrick Braun, Aachen Thomas Buhk, Hamburg Rob Camp, Barcelona (Spain/USA) Rika Draenert, Munich Christian Eggers, Linz (Austria) Stefan Esser, Essen Gerd Fätkenheuer, Cologne Gunar Günther, Windhoek (Namibia) Thomas Harrer, Erlangen Christian Herzmann, Borstel Christian Hoffmann, Hamburg Heinz-August Horst, Kiel Martin Hower, Dortmund Christoph Lange, Borstel Thore Lorenzen, Hamburg Tim Niehues, Krefeld Christian Noah, Hamburg Ramona Pauli, Munich Ansgar Rieke, Koblenz Jürgen Kurt Rockstroh, Bonn Thorsten Rosenkranz, Hamburg Bernhard Schaaf, Dortmund Ulrike Sonnenberg-Schwan, Munich Christoph D. Spinner, Munich Thomas Splettstoesser (Figures), Berlin Matthias Stoll, Hannover Hendrik Streeck, Essen/Boston (USA) Jan Thoden, Freiburg Markus Unnewehr, Dortmund Mechthild Vocks-Hauck, Berlin Jan-Christian Wasmuth, Bonn Michael Weigel, Schweinfurt Thomas Weitzel, Santiago (Chile) Eva Wolf, Munich HIV 2015/16 www.hivbook.com Edited by Christian Hoffmann and Jürgen K. Rockstroh Medizin Fokus Verlag IV Christian Hoffmann, M.D., Ph.D. ICH Stadtmitte (Infektionsmedizinisches Centrum Hamburg) Glockengiesserwall 1 20095 Hamburg, Germany Phone: + 49 40 2800 4200 Fax: + 49 40 2800 42020 [email protected] Jürgen K. Rockstroh, M.D., Ph.D. Department of Medicine I University of Bonn Sigmund-Freud-Strasse 25 53105 Bonn, Germany Phone: + 49 228 287 6558 Fax: + 49 228 287 5034 [email protected] HIV Medicine is an ever-changing field. The editors and authors of HIV 2015/16 have made every effort to provide information that is accurate and complete as of the date of publication. -

TREATMENT B U L L E T I N
ISSN 1472-4863 HIV-treatment bulletin VOLUME 2 NO.2 MARCH 2001 FORMERLYh- Doctor Fax tb H I V i - B a s e TREATMENT bulletin. 2 Volume 2 No.2 - MARCH 2001 TREATMENT ACCESS • Capravirine clinical trials restricted: Additional safety evaluation required • From Talk to Action in Fighting AIDS in the Developing Countries: 8th Retrovirus Conference opening session • Gilead announces start of early access program for investigational anti-HIV agent tenofovir DF in US and France • UNAIDS calls for new deal between pharmaceutical companies and society • Mortality from liver disease increasing in HIV-positive patients • US trade action threatens Brazilian AIDS programme TREATMENT GUIDELINES • Brazil May Flout Trade Laws to Keep AIDS Drugs Free • Roche Open to Discuss Patent Rights of AIDS Drug With Brazil • First European guidelines for HIV-1 drug resistance testing • Crusading Indian firm takes on might of Glaxo SmithKline: • U.S.A HIV treatment guidelines updated for adults and Cipla is offers anti-HIV drugs at a fraction of rivals’ prices adolescents • GSK to review drug pricing policy: Pharmaceuticals giant • U.S.A. Perinatal Treatment Guidelines Updated, Jan. 24, 2001 reacts to criticism over costs to poor countries • Oxfam launches stinging attack on drug industry over cheap CONFERENCE REPORTS medicines ban 8th Conference on Retroviruses and Opportunistic Infections • Companies Weigh Offer of Royalties for AIDS Drugs for Africa February 4 – 8, 2001. Chicago IL. OTHER NEWS • Differentiating within and between drug classes: Sometimes it’s toxicity, -

L:\0901 with Peru\0901PHARMAPPX.Wpd
Harmonized Tariff Schedule of the United States (2009) (Rev. 1) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2009) (Rev. 1) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. ABACAVIR 136470-78-5 ACEXAMIC ACID 57-08-9 ABAFUNGIN 129639-79-8 ACICLOVIR 59277-89-3 ABAMECTIN 65195-55-3 ACIFRAN 72420-38-3 ABANOQUIL 90402-40-7 ACIPIMOX 51037-30-0 ABAPERIDONE 183849-43-6 ACITAZANOLAST 114607-46-4 ABARELIX 183552-38-7 ACITEMATE 101197-99-3 ABATACEPT 332348-12-6 ACITRETIN 55079-83-9 ABCIXIMAB 143653-53-6 ACIVICIN 42228-92-2 ABECARNIL 111841-85-1 ACLANTATE 39633-62-0 ABETIMUS 167362-48-3 ACLARUBICIN 57576-44-0 ABIRATERONE 154229-19-3 ACLATONIUM NAPADISILATE 55077-30-0 ABITESARTAN 137882-98-5 ACODAZOLE 79152-85-5 ABLUKAST 96566-25-5 ACOLBIFENE 182167-02-8 ABRINEURIN 178535-93-8 ACONIAZIDE 13410-86-1 ABUNIDAZOLE 91017-58-2 ACOTIAMIDE 185106-16-5 ACADESINE 2627-69-2 ACOXATRINE 748-44-7 ACAMPROSATE 77337-76-9 ACREOZAST 123548-56-1 ACAPRAZINE 55485-20-6 -

What's in the Pipeline: New HIV Drugs, Vaccines, Microbicides, HCV And
What’s in the Pipeline: New HIV Drugs, Vaccines, Microbicides, HCV and TB Treatments in Clinical Trials by Rob Camp, Richard Jefferys, Tracy Swan & Javid Syed edited by Mark Harrington & Bob Huff Treatment Action Group New York, NY, USA July 2005 e thymidine • BI-201 • Racivir (PSI 5004) • TMC-278 • Diarylpyrimidine (DAPY) • 640385 • Reverset (D-D4FC) • JTK-303 • UK-427 (maraviroc) • Amdoxovir • AMD-070 • Vicriviroc LIPO-5 • GTU-Multi-HIV • pHIS-HIV-B • rFPV-HIV-B • ADMVA • GSK Protein HIV Vaccine TBC-M335 (MVA) • TBC-F357 (FPV) • TBC-F349 (FPV) • LIPO-4T (LPHIV-1) • LFn-p24 • H G • Oligomeric gp140/MF59 • VRC-HIVDNA-009-00-VP • PolyEnv1 • ISS P-001 • EP HIV- • BufferGel • Lactin-V • Protected Lactobacilli in combination with BZK • Tenofovir/PMPA G ulose acetate/CAP) • Lime Juice • TMC120 • UC-781 • VivaGel (SPL7013 gel) • ALVAC Ad5 • Autologous dendritic cells pulsed w/ALVAC • Autologous dendritic cell HIV vaccination x • Tat vaccine • GTU-nef DNA vaccine • Interleukin-2 (IL-2) • HE2000 • Pegasys (peginter L-4/IL-13 trap • Serostim • Tucaresol • MDX-010 anti-CTLA4 antibody • Cyclosporine A • 496 • HGTV43 • M87o • Vertex • VX-950 • Idenix • Valopicitabine (NM283) • JTK-003 mplant • Albuferon • Celgosivir (MBI-3253) • IC41 • INN0101 • Tarvicin • ANA971 (oral) floxacin, Tequin • J, TMC207 (ex R207910) • LL-3858 • M, moxifloxacin, Avelox • PA-824 Acknowledgements. Thanks to our intrepid editors, Bob Huff, copy-editor Andrea Dailey, and proof-reader Jen Curry, to awesome layout expert Lei Chou, to webmaster Joel Beard, to Joe McConnell for handling administrative matters related to the report, and most of all to the board and supporters of TAG for making our work possible.