HIV-Infected Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

( 12 ) United States Patent
US010385067B2 (12 ) United States Patent ( 10 ) Patent No. : US 10 , 385, 067 B2 Carra et al. (45 ) Date of Patent: Aug. 20 , 2019 (54 ) SODIUM (2R , 55 , 13AR ) - 7 , 9 -DIOX0 - 10 ( 56 ) References Cited ( 2 , 4 ,6 - TRIFLUOROBENZYL )CARBAMOYL ) 2 , 3 , 4 , 5 , 7 , 9 , 13 , 13A -OCTAHYDRO - 2 , 5 U . S . PATENT DOCUMENTS METHANOPYRIDO [ 1 ' , 2 ' : 4 , 5 ]PYRAZINO 5 , 814 ,639 A 9 / 1998 Liotta et al . [ 2 , 1 - B ] [ 1 , 3 ]OXAZEPIN - 8 - OLATE 5 , 914 , 331 A 6 / 1999 Liotta et al . 5 ,922 ,695 A 7 / 1999 Arimilli et al . 5 , 935 , 946 A 8 / 1999 Munger, Jr . et al. (71 ) Applicant: Gilead Sciences , Inc ., Foster Ctiy , CA 5 , 977 , 089 A 11/ 1999 Arimilli et al. (US ) 6 ,043 , 230 A 3 / 2000 Arimilli et al. 6 ,620 , 841 B1 9 / 2003 Fujishita et al . (72 ) Inventors : Ernest A . Carra , Foster City , CA ( US ) ; 6 ,642 , 245 B1 11/ 2003 Liotta et al. 6 , 703 , 396 B1 3 / 2004 Liotta et al . Irene Chen , San Mateo , CA (US ) ; 7 , 176 , 220 B2 2 /2007 Satoh et al. Vahid Zia , Palo Alto , CA (US ) 7 ,419 , 969 B2 9 / 2008 Naidu et al. 7 , 550 , 463 B2 6 / 2009 Yoshida (73 ) Assignee : Gilead Sciences , Inc. , Foster City , CA 7 ,635 , 704 B2 12 /2009 Satoh et al. 7 , 858 , 788 B2 12 / 2010 Yoshida et al . (US ) 8 , 129 , 385 B2 3 / 2012 Johns et al . 8 , 148 , 374 B2 4 / 2012 Desai et al. ( * ) Notice : Subject to any disclaimer , the term of this 8 , 188 , 271 B2 5 / 2012 Yoshida et al . -

Canadian HIV/AIDS Pharmacists Network (CHAP) Newsletter – April 2000
1 Canadian HIV/AIDS Pharmacists Network (CHAP) Newsletter – April 2000 Happy Spring! It is pouring cats and dogs here in “sunny” Alberta today, but the good news is that the grass and trees are green (yes I am an optimist). I even had to shake off the dust from my umbrella! I won’t complain because Spring is finally here……. Hurray! As you know, I have officially taken over the Chair from Kathy Slayter (aka “Mom”). This is my first attempt at a newsletter so please be patient with me! Social News Well I am sure everyone has heard the good news but I would like to officially congratulate Kathy and Mike on the birth of their little boy, Ethan James Tucker, on December 11, 1999. Congratulations Kathy! New Members I would like to officially welcome the following new members: Laura Park-Wyllie who has taken over Michelle Foisy’s position as HIV Primary Care Pharmacist at the St. Michael’s Hospital, Health Centre at 410 (formerly Wellesley Health Centre). Deborah Kelly who is as an Assistant Professor of Clinical Pharmacy at Memorial University in Newfoundland and Clinical Pharmacy Specialist at Health Care Corp of St. John’s. Kimberly Montgomery who is a Pharmacist at the Southern Alberta Clinic (taking over from Nikola Ostrop). Unfortunately, Kim will not be with us long. She is getting married in August and then will be moving to Newfoundland. Her last day at the clinic will be June 30, 2000. Congratulations on your upcoming wedding Kim! For those of you interested, there is an opening at the SAC and you can contact Kimberly for more details… 2 CAHR Update I thought the CAHR conference was excellent and the Network meeting went well (considering all of the problems we had arranging the first Network meeting of the millenium!). -

(12) Patent Application Publication (10) Pub. No.: US 2016/0058872 A1 Crew Et Al
US 2016.0058872A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2016/0058872 A1 Crew et al. (43) Pub. Date: Mar. 3, 2016 (54) IMIDE-BASED MODULATORS OF A613 L/426 (2006.01) PROTEOLYSIS AND ASSOCATED METHODS A 6LX3 L/505 (2006.01) OF USE A613 L/454 (2006.01) A613 L/55 (2006.01) (71) Applicant: Arvinas, Inc., New Haven, CT (US) C07D40 L/4 (2006.01) A6II 45/06 (2006.01) (72) Inventors: Andrew P. Crew, Guilford, CT (US); (52) U.S. Cl. Craig Crews, New Haven, CT (US), CPC ............ A61K 47/481 (2013.01); C07D401/14 Hanging Dong, Madison, CT (US); Jing (2013.01); C07D 495/14 (2013.01); C07D Wang, Milford, CT (US); Yimin Qian, 417/14 (2013.01); A61K 45/06 (2013.01); Plainsboro, NJ (US); Kam Siu Milford, A6 IK3I/505 (2013.01); A61 K3I/454 CT (US); Meizhong Jin, East Northport, (2013.01); A61 K3I/551 (2013.01); A61 K NY (US) 3 1/426 (2013.01) (21) Appl. No.: 14/792,414 (57) ABSTRACT (22) Filed: Jul. 6, 2015 The description relates to imide-based compounds, including Related U.S. Application Data bifunctional compounds comprising the same, which find utility as modulators of targeted ubiquitination, especially (63) Continuation-in-part of application No. 14/686.640, inhibitors of a variety of polypeptides and other proteins filed on Apr. 14, 2015. which are degraded and/or otherwise inhibited by bifunc (60) Provisional application No. 61/979,351, filed on Apr. tional compounds according to the present invention. In par 14, 2014, provisional application No. -

Meeting Report: 26Th International Conference on Antiviral Research Q
Antiviral Research 100 (2013) 276–285 Contents lists available at ScienceDirect Antiviral Research journal homepage: www.elsevier.com/locate/antiviral Review Meeting report: 26th International Conference on Antiviral Research q R. Anthony Vere Hodge Vere Hodge Antivirals Ltd, Old Denshott, Leigh, Reigate, Surrey, UK article info abstract Article history: The 26th International Conference on Antiviral Research (ICAR) was held in San Francisco, California from Received 2 August 2013 May 11 to 15, 2013. This article summarizes the principal invited lectures at the meeting. The opening Accepted 8 August 2013 symposium on the legacy of the late Antonín Holy´ included presentations on his pioneering work with Available online 21 August 2013 nucleotide analogs, which led to the development of several antiviral drugs including tenofovir. This drug has transformed the treatment of HIV infection and has recently become the first-line therapy for chronic Keywords: hepatitis B. The Gertrude Elion Award lecturer described the anti-HIV activities of the CCR5 inhibitor Human immunodeficiency virus cenicriviroc and the reverse transcriptase inhibitor festinavirÒ, and also reviewed the evaluation of bio- Hepatitis B degradable nanoparticles with adjuvant activity. The William Prusoff Award winner reported on the cre- Hepatitis C Herpesviruses ation of NAOMI, a computer model with 21 enzymes to predict the activity of nucleoside analogs against Antiviral therapy hepatitis C virus (HCV). Other invited lecturers discussed the development of countermeasures against severe dengue and the potential of RNA virus capping and repair enzymes as drug targets. Topics in the clinical symposium included the current status of the anti-HCV compounds sovaprevir, ACH-3102, miravirsen and ALS-2200; the evaluation of single-tablet regimens for HIV infection; and the investiga- tion of cytomegalovirus resistance to CMX001. -

Modifications to the Harmonized Tariff Schedule of the United States To
U.S. International Trade Commission COMMISSIONERS Shara L. Aranoff, Chairman Daniel R. Pearson, Vice Chairman Deanna Tanner Okun Charlotte R. Lane Irving A. Williamson Dean A. Pinkert Address all communications to Secretary to the Commission United States International Trade Commission Washington, DC 20436 U.S. International Trade Commission Washington, DC 20436 www.usitc.gov Modifications to the Harmonized Tariff Schedule of the United States to Implement the Dominican Republic- Central America-United States Free Trade Agreement With Respect to Costa Rica Publication 4038 December 2008 (This page is intentionally blank) Pursuant to the letter of request from the United States Trade Representative of December 18, 2008, set forth in the Appendix hereto, and pursuant to section 1207(a) of the Omnibus Trade and Competitiveness Act, the Commission is publishing the following modifications to the Harmonized Tariff Schedule of the United States (HTS) to implement the Dominican Republic- Central America-United States Free Trade Agreement, as approved in the Dominican Republic-Central America- United States Free Trade Agreement Implementation Act, with respect to Costa Rica. (This page is intentionally blank) Annex I Effective with respect to goods that are entered, or withdrawn from warehouse for consumption, on or after January 1, 2009, the Harmonized Tariff Schedule of the United States (HTS) is modified as provided herein, with bracketed matter included to assist in the understanding of proclaimed modifications. The following supersedes matter now in the HTS. (1). General note 4 is modified as follows: (a). by deleting from subdivision (a) the following country from the enumeration of independent beneficiary developing countries: Costa Rica (b). -

The Use of Stems in the Selection of International Nonproprietary Names (INN) for Pharmaceutical Substances
WHO/PSM/QSM/2006.3 The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances 2006 Programme on International Nonproprietary Names (INN) Quality Assurance and Safety: Medicines Medicines Policy and Standards The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 © World Health Organization 2006 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. -
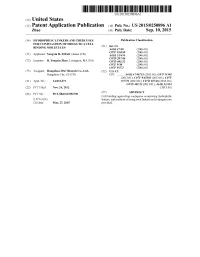
(12) Patent Application Publication (10) Pub. No.: US 2015/0250896 A1 Zhao (43) Pub
US 20150250896A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2015/0250896 A1 Zhao (43) Pub. Date: Sep. 10, 2015 (54) HYDROPHILIC LINKERS AND THEIR USES Publication Classification FOR CONUGATION OF DRUGS TO A CELL (51) Int. Cl BNDING MOLECULES A647/48 (2006.01) (71) Applicant: Yongxin R. ZHAO, Henan (CN) Ek E. 30.8 C07D 207/216 (2006.01) (72) Inventor: R. Yongxin Zhao, Lexington, MA (US) C07D 40/12 (2006.01) C07F 9/30 (2006.01) C07F 9/572 (2006.01) (73) Assignee: Hangzhou DAC Biotech Co., Ltd., (52) U.S. Cl. Hangzhou City, ZJ (CN) CPC ........... A61K47/48715 (2013.01); C07F 9/301 (2013.01); C07F 9/65583 (2013.01); C07F (21) Appl. No.: 14/432,073 9/5721 (2013.01); C07D 207/46 (2013.01); C07D 401/12 (2013.01); A61 K3I/454 (22) PCT Filed: Nov. 24, 2012 (2013.01) (86). PCT No.: PCT/B2O12/0567OO Cell(57) binding- agent-drugABSTRACT conjugates comprising hydrophilic- S371 (c)(1), linkers, and methods of using Such linkers and conjugates are (2) Date: Mar. 27, 2015 provided. Patent Application Publication Sep. 10, 2015 Sheet 1 of 23 US 2015/0250896 A1 O HMDS OSiMe 2n O Br H-B-H HPC 3 2 COOEt essiop-\5. E B to NH 120 °C, 2h OsiMe3 J 50 °C, 2h eSiO OEt 120 oC, sh 1 2 3. 42% from 1 Bra-11a1'oet - Brn 11-1 or a 1-1 or ÓH 140 °C ÓEt ÓEt 4 5 6 - --Messio. 8 B1a-Br aus 20 cc, hP-1}^-'ot Br1-Y. -

This Project Has Been Supported with Unrestriced Grants from Abbvie Gilead Sciences HEXAL Janssen-Cilag MSD Viiv Healthcare By
This project has been supported with unrestriced grants from AbbVie Gilead Sciences HEXAL Janssen-Cilag MSD ViiV Healthcare By Marcus Altfeld, Hamburg/Boston (USA) Achim Barmeyer, Dortmund Georg Behrens, Hannover Dirk Berzow, Hamburg Christoph Boesecke, Bonn Patrick Braun, Aachen Thomas Buhk, Hamburg Rob Camp, Barcelona (Spain/USA) Rika Draenert, Munich Christian Eggers, Linz (Austria) Stefan Esser, Essen Gerd Fätkenheuer, Cologne Gunar Günther, Windhoek (Namibia) Thomas Harrer, Erlangen Christian Herzmann, Borstel Christian Hoffmann, Hamburg Heinz-August Horst, Kiel Martin Hower, Dortmund Christoph Lange, Borstel Thore Lorenzen, Hamburg Tim Niehues, Krefeld Christian Noah, Hamburg Ramona Pauli, Munich Ansgar Rieke, Koblenz Jürgen Kurt Rockstroh, Bonn Thorsten Rosenkranz, Hamburg Bernhard Schaaf, Dortmund Ulrike Sonnenberg-Schwan, Munich Christoph D. Spinner, Munich Thomas Splettstoesser (Figures), Berlin Matthias Stoll, Hannover Hendrik Streeck, Essen/Boston (USA) Jan Thoden, Freiburg Markus Unnewehr, Dortmund Mechthild Vocks-Hauck, Berlin Jan-Christian Wasmuth, Bonn Michael Weigel, Schweinfurt Thomas Weitzel, Santiago (Chile) Eva Wolf, Munich HIV 2015/16 www.hivbook.com Edited by Christian Hoffmann and Jürgen K. Rockstroh Medizin Fokus Verlag IV Christian Hoffmann, M.D., Ph.D. ICH Stadtmitte (Infektionsmedizinisches Centrum Hamburg) Glockengiesserwall 1 20095 Hamburg, Germany Phone: + 49 40 2800 4200 Fax: + 49 40 2800 42020 [email protected] Jürgen K. Rockstroh, M.D., Ph.D. Department of Medicine I University of Bonn Sigmund-Freud-Strasse 25 53105 Bonn, Germany Phone: + 49 228 287 6558 Fax: + 49 228 287 5034 [email protected] HIV Medicine is an ever-changing field. The editors and authors of HIV 2015/16 have made every effort to provide information that is accurate and complete as of the date of publication. -

TREATMENT B U L L E T I N
ISSN 1472-4863 HIV-treatment bulletin VOLUME 2 NO.2 MARCH 2001 FORMERLYh- Doctor Fax tb H I V i - B a s e TREATMENT bulletin. 2 Volume 2 No.2 - MARCH 2001 TREATMENT ACCESS • Capravirine clinical trials restricted: Additional safety evaluation required • From Talk to Action in Fighting AIDS in the Developing Countries: 8th Retrovirus Conference opening session • Gilead announces start of early access program for investigational anti-HIV agent tenofovir DF in US and France • UNAIDS calls for new deal between pharmaceutical companies and society • Mortality from liver disease increasing in HIV-positive patients • US trade action threatens Brazilian AIDS programme TREATMENT GUIDELINES • Brazil May Flout Trade Laws to Keep AIDS Drugs Free • Roche Open to Discuss Patent Rights of AIDS Drug With Brazil • First European guidelines for HIV-1 drug resistance testing • Crusading Indian firm takes on might of Glaxo SmithKline: • U.S.A HIV treatment guidelines updated for adults and Cipla is offers anti-HIV drugs at a fraction of rivals’ prices adolescents • GSK to review drug pricing policy: Pharmaceuticals giant • U.S.A. Perinatal Treatment Guidelines Updated, Jan. 24, 2001 reacts to criticism over costs to poor countries • Oxfam launches stinging attack on drug industry over cheap CONFERENCE REPORTS medicines ban 8th Conference on Retroviruses and Opportunistic Infections • Companies Weigh Offer of Royalties for AIDS Drugs for Africa February 4 – 8, 2001. Chicago IL. OTHER NEWS • Differentiating within and between drug classes: Sometimes it’s toxicity, -

L:\0901 with Peru\0901PHARMAPPX.Wpd
Harmonized Tariff Schedule of the United States (2009) (Rev. 1) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2009) (Rev. 1) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. ABACAVIR 136470-78-5 ACEXAMIC ACID 57-08-9 ABAFUNGIN 129639-79-8 ACICLOVIR 59277-89-3 ABAMECTIN 65195-55-3 ACIFRAN 72420-38-3 ABANOQUIL 90402-40-7 ACIPIMOX 51037-30-0 ABAPERIDONE 183849-43-6 ACITAZANOLAST 114607-46-4 ABARELIX 183552-38-7 ACITEMATE 101197-99-3 ABATACEPT 332348-12-6 ACITRETIN 55079-83-9 ABCIXIMAB 143653-53-6 ACIVICIN 42228-92-2 ABECARNIL 111841-85-1 ACLANTATE 39633-62-0 ABETIMUS 167362-48-3 ACLARUBICIN 57576-44-0 ABIRATERONE 154229-19-3 ACLATONIUM NAPADISILATE 55077-30-0 ABITESARTAN 137882-98-5 ACODAZOLE 79152-85-5 ABLUKAST 96566-25-5 ACOLBIFENE 182167-02-8 ABRINEURIN 178535-93-8 ACONIAZIDE 13410-86-1 ABUNIDAZOLE 91017-58-2 ACOTIAMIDE 185106-16-5 ACADESINE 2627-69-2 ACOXATRINE 748-44-7 ACAMPROSATE 77337-76-9 ACREOZAST 123548-56-1 ACAPRAZINE 55485-20-6 -

Download Article PDF/Slides
Roy M. Gulick, MD, MPH View from the Pipeline: Director, Cornell HIV Clinical Trials Unit Associate Professor of Medicine The 2005 Review of Experimental Weill Cornell Medical College Antiretrovirals New York, New York Summary by Tim Horn Reprinted from The prn Notebook® | june 2005 | Dr. James F. Braun, Editor-in-Chief | Tim Horn, Executive Editor. Published in New York City by the Physicians’ Research Network, Inc.® | John Graham Brown, Executive Director Edited by Sheldon T. Brown, md, For further information and other articles available online, visit http://www.prn.org | All rights reserved. ©june 2005 and Martin Markowitz, md there are 20 unique medications approved for the treatment of maintaining undetectable hiv-rna levels while taking standard regi- hiv infection. Despite this impressive number, there is an indisputable mens, added 200 mg d-d4fc to their therapies for ten days (and two oth- need for new anti-hiv compounds that have potent and durable effica- er others added d-d4fc placebos). cy profiles, unique resistance patterns, patient-friendly dosing schedules, The mean reduction in viral load among the treatment-naive pa- and minimal toxicities. What follows is an overview of some the newest tients in the three treatment groups ranged from 1.67 log10 copies/mL to antiretroviral contenders, discussed by Dr. Roy M. Gulick during a re- 1.77 log10 copies/mL (see Figure 1). Among the treatment-experienced pa- cent meeting of the Physicians’ Research Network. tients, the mean reduction in viral load was 0.8 log10 copies/mL. Seven of eight treatment-naive patients (in the 200 mg d-d4fc group) and four of eight treatment-experienced patients achieved undetectable viral loads (<400 copies/mL) after ten days of therapy. -

Emtricitabine/Tenofovir Alafenamide Fixed-Dose Combination (F/Taf Fdc)
SECTION 2.7.1—SUMMARY OF BIOPHARMACEUTICAL STUDIES AND ASSOCIATED ANALYTICAL METHODS EMTRICITABINE/TENOFOVIR ALAFENAMIDE FIXED-DOSE COMBINATION (F/TAF FDC) Gilead Sciences 20 CONFIDENTIAL AND PROPRIETARY INFORMATION F/TAF 2.7.1 Summary of Biopharmaceutical Studies Final TABLE OF CONTENTS SECTION 2.7.1—SUMMARY OF BIOPHARMACEUTICAL STUDIES AND ASSOCIATED ANALYTICAL METHODS.................................................................................................................................1 TABLE OF CONTENTS ..............................................................................................................................................2 LIST OF IN-TEXT TABLES........................................................................................................................................3 GLOSSARY OF ABBREVIATIONS AND DEFINITION OF TERMS......................................................................5 PHARMACOKINETIC ABBREVIATIONS AND DEFINITIONS ............................................................................7 1. SUMMARY OF BIOPHARMACEUTICAL STUDIES AND ASSOCIATED ANALYTICAL METHODS ...........................................................................................................................................................8 1.1. Background and Overview.......................................................................................................................8 1.1.1. Formulation Development......................................................................................................9