World Bank Document
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

OREDA, 1.47MW, Rooftop Solar, Odisha, July 2020
Request for Proposal (RFP) for design, engineering, supply, installation, testing, commissioning and acceptance of Rooftop Solar Power System (RSPS) and solar Street Lighting System (SLS) through off- grid mode along with Comprehensive Maintenance for ten (10) years at various locations in the 115 no. of Panchayat Samiti Office premises across all 30 district(s) in Odisha E-procurement Website: www.tenderwizard.com/OREDA RFP no.: 2701/OREDA/PD-05/2020 dated 30th Jun 2020 Contact details: Odisha Renewable Energy Development Agency (OREDA) Address: S-3/59, Mancheswar Industrial Estate, Bhubaneswar - 751010, Odisha. Phone: (0674) 2588260, 2586398, 2580554, Fax: 2586368 Email: [email protected]. Website: www.oredaorissa.com (This page is international left blank.) RFP No. 2701/OREDA/PD-05/2020 dated 30th Jun 2020 OREDA 1 Notice Inviting Tender (NIT) NIT no.: 2701/OREDA/PD-05/2020 dated 30 Jun 2020 Type of bidding: Domestic Competitive Bidding (DCB) Mode of bidding: Open bidding, Single stage two envelope, E-bidding Odisha Renewable Energy Development Agency (OREDA) invites Request for Proposal (RFP) for design, engineering, supply, installation, testing, commissioning and acceptance of Rooftop Solar Power System (RSPS) and solar Street Lighting System (SLS) through off-grid mode along with Comprehensive Maintenance for ten (10) years at various locations in the 115 no. of Panchayat Samiti Office premises across all 30 district(s) in Odisha. The Schedule of Events is given below: Sl. No. Events Schedule 1. Date of publication of Request for Proposal (RFP) on 30th Jun 2020 E-procurement Website and OREDA Website 2. Due date and time for receipt of pre-bid queries on the 07th Jul 2020, Time: 1:00 PM RFP 3. -

District Irrigation Plan of Kalahandi District, Odisha
District Irrigation Plan of Kalahandi, Odisha DISTRICT IRRIGATION PLAN OF KALAHANDI DISTRICT, ODISHA i District Irrigation Plan of Kalahandi, Odisha Prepared by: District Level Implementation Committee (DLIC), Kalahandi, Odisha Technical Support by: ICAR-Indian Institute of Soil and Water Conservation (IISWC), Research Centre, Sunabeda, Post Box-12, Koraput, Odisha Phone: 06853-220125; Fax: 06853-220124 E-mail: [email protected] For more information please contact: Collector & District Magistrate Bhawanipatna :766001 District : Kalahandi Phone : 06670-230201 Fax : 06670-230303 Email : [email protected] ii District Irrigation Plan of Kalahandi, Odisha FOREWORD Kalahandi district is the seventh largest district in the state and has spread about 7920 sq. kms area. The district is comes under the KBK region which is considered as the underdeveloped region of India. The SC/ST population of the district is around 46.31% of the total district population. More than 90% of the inhabitants are rural based and depends on agriculture for their livelihood. But the literacy rate of the Kalahandi districts is about 59.62% which is quite higher than the neighboring districts. The district receives good amount of rainfall which ranges from 1111 to 2712 mm. The Net Sown Area (NSA) of the districts is 31.72% to the total geographical area(TGA) of the district and area under irrigation is 66.21 % of the NSA. Though the larger area of the district is under irrigation, un-equal development of irrigation facility led to inequality between the blocks interns overall development. The district has good forest cover of about 49.22% of the TGA of the district. -

Self-Employment
SELF-EMPLOYMENT A Framework for Implementation National Rural Livelihood Mission Ministry of Rural Development Government of India SELF-EMPLOYMENT A Framework for Implementation National Rural Livelihood Mission Ministry of Rural Development Government of India June 22, 2016 Executive Summary MoRD has been thinking about a strategy to systematically bring panchayats out of poverty within a clear timeline. Given that 51% of the rural workforce is self-employed, there is a need to create a policy framework for holistically improving self-employment opportunities for the rural poor. In the light of the above, a framework document titled Self-Employment–A Framework for Implementation (No.J-11060/1/2016-RL) dated June 22nd, 2016 has been prepared after a consultation with state representatives in NIRD&PR in Hyderabad on January 9, 2016 and a national consultation in Delhi at Vigyan Bhawan on January 14, 2016. Before the document is taken up for formal consideration at the GoI level, it was thought necessary to seek the opinion of State governments. Accordingly, a copy of the framework document is hereby attached for your comments. The framework proposes a new scheme within the NRLM framework called the Grameen Swarozghar Yojana (GSY) that would be implemented through inter-departmental collaboration. The proposal is to ensure that self-employment, skill up-gradation, and efficient delivery of government schemes and entitlements lead to poverty-free panchayats within a definite timeline. The new scheme is proposed on 7 key principles: 1. Build on the strengths of previous efforts while avoiding it weaknesses 2. Build on the recent success of establishing high quality SHGs through the CRP strategy 3. -

2011-Dshb-Kalahandi.Pdf
GOVERNMENT OF ODISHA DISTRICT STATISTICAL HANDBOOK KALAHANDI 2011 DISTRICT PLANNING AND MONITORING UNIT KALAHANDI ( Price : Rs.25.00 ) CONTENTS Table No. SUBJECT PAGE ( 1 ) ( 2 ) ( 3 ) Socio-Economic Profile : Kalahandi … 1 Administrative set up … 4 I POSITION OF DISTRICT IN THE STATE 1.01 Geographical Area … 5 District wise Population with Rural & Urban and their proportion of 1.02 … 6 Odisha. District-wise SC & ST Population with percentage to total population of 1.03 … 8 Odisha. 1.04 Population by Sex, Density & Growth rate … 10 1.05 District wise sex ratio among all category, SC & ST by residence of Odisha. … 11 1.06 District wise Literacy rate, 2011 Census … 12 Child population in the age Group 0-6 in different district of Odisha. 1.07 … 13 II AREA AND POPULATION Geographical Area, Households and Number of Census Villages in different 2.01 … 14 Blocks and ULBs of the District. 2.02 Classification of workers (Main+ Marginal) … 15 2.03 Total workers and work participation by residence … 17 III CLIMATE 3.01 Month wise Actual Rainfall in different Rain gauge Stations in the District. … 18 3.02 Month wise Temperature and Relative Humidity of the district. … 20 IV AGRICULTURE 4.01 Block wise Land Utilisation pattern of the district. … 21 Season wise Estimated Area, Yield rate and Production of Paddy in 4.02 … 23 different Blocks and ULBs of the district. Estimated Area, Yield rate and Production of different Major crops in the 4.03 … 25 district. 4.04 Source- wise Irrigation Potential Created in different Blocks of the district … 26 Achievement of Pani Panchayat programme of different Blocks of the 4.05 … 27 district 4.06 Consumption of Chemical Fertiliser in different Blocks of the district. -

Kalahandi Family Planning Plan 2011 12
DRAFT 2011 -12 District Family Planning Plan District: KALAHANDI District Family Welfare Bureau Zilla Swasthya Samiti KALAHANDI DISTRICT FAMILY PLANNING PLAN 2011 -12 1 KALAHANDI DISTRICT FAMILY PLANNING PLAN 2011-12 2 KALAHANDI DISTRICT FAMILY PLANNING PLAN 2011-12 3 Table of Contents Chapter Topics Chapter – 1 Background Chapter – 2 Situational Analyses a. Contraceptive Use b. Service Delivery c. Quality Assurance Mechanism d. Logistic and Supply System e. Human Resource Development f. Communication Activities g. Private Sector Partnership h. Monitoring and Evaluation Chapter – 3 District Priorities as per the situations with respect to the State mandate. Chapter – 4 Family Planning Plan for the year 2011-12 a. Service Delivery b. Human Resource Development & Training c. Logistics and supply chain with requirement & distribution plan d. Communication Activities e. Private Sector Partnership f. Monitoring and Evaluation g. Any other (Innovations, Dist/Block/Sector specific) IEC, new plans etc. Chapter – 5 Resource Requirements KALAHANDI DISTRICT FAMILY PLANNING PLAN 2011-12 4 Executive Summary – Kalahandi district is situated in the southwestern portion of Orissa. Geographically this district lies between 19º 8’ N 20º 25’ N latitudes and 82 0 32 ’ E and 83 0 47’ E longitudes with geographical area of 7920 sq Km. The population of the Kalahandi district as per the 2011 census is 157305; the sex ratio is 1003 per one thousand male. It has 13 blocks, 273 Grampanchayats, 2236 Rev villages (including 137 uninhabited villages), 13 Tahsils, and 2 Subdivisions. It has 4 towns Bhawanipatna Municipality, Junagarh & Kesinga NAC and Dharamgarh. Out of 13 blocks two are Tribal blocks1-Biswanathpur 2.Thuamulrampur. -

List of Candidates ( Kalahandi) for Document
LIST OF CANDIDATES ( KALAHANDI) FOR DOCUMENT VERIFICATION & CBST THE POST OF ANM-MHU (ADVT NO 4288/21.08.2018) UNDER NHM, KALAHANDI (VENUE-ANMTC, BHAWANIPATNA) CASTE DATE OF SL. APPL. NAME OF THE FATHER'S/ DOMICILE SEX (UR/SC/ DOB DOCUMENT PRESENT ADDRESS NO. NO. CANDIDATE HUSBAND'S NAME DISTRICT (M/F) ST/SEBC/ (DD-MM-YYYY) VERIFICATION SEBC) & CBST UR-CATEGORY AT- TUJUNG, PO- M.RAMPUR, KALAHANDI, 1 559 PRATIMA NAG BRUNDABAN NAG KALAHANDI F SC 20/10/1993 15-Dec-18 766102 AT-DEWANSAHEB PADA, PO- 2 679 NILEEMA BHATI JAGADISH BHATI BHAWANIPATNA, DIST-KALAHANDI, PIN- KALAHANDI F SEBC 15/05/1995 15-Dec-18 766001 AT-GHUGURBAHALI,PO-SANTPUR,VIA- 3 8 ASHA LATA SAHU TIKARAM SAHU KALAHANDI F SEBC 01/05/1997 15-Dec-18 NARLA, KALAHANDI-766110 AT/PO-BRUNDABAHAL,VIA- 4 269 LILI RAUT RAHASA RAUT KALAHANDI F SEBC 10/18/1992 15-Dec-18 GOLAMUNDA,DIST-KALAHANDI,PIN-766016 AT- KANTAMAL, PO- KUHURA, VIA- BORDA, 5 650 HEMALATA SAHU SANYASI SAHU KEGAON, GOLAMUNDA, KALAHANDI, KALAHANDI F SEBC 24/11/1995 15-Dec-18 766036 AT- LIMSER, PO- BRUNDABAHAL, VIA- 6 82 LILABATI MEHER GUNAKARA MEHER GOLAMUNDA, DIST- KALAHANDI, PIN- KALAHANDI F SEBC 5/16/1996 15-Dec-18 766016 AT- LAKHAGUDA, PO- RUPRARPAD, PS- 7 552 SEEMA BHOI BASANTA BHOI KALAHANDI F SEBC 01/05/1995 15-Dec-18 NARLA, KALAHANDI, 766101 AT/PO- NAKTIKANI, VIA- GOLAMUNDA, DIST- 8 432 KAMINI SENAPATI PREM SENAPATI KALAHANDI F SEBC 11/07/1991 15-Dec-18 KALAHANDI, PIN- 766016 PRAKASH CH. AT/PO-JUNAGARH,TALABANDHAPADA ,DIST- 9 344 MANISHA GHADEI KALAHANDI F SEBC 03/11/1994 15-Dec-18 GHADEI KALAHANDI-766014 AT/PO- -
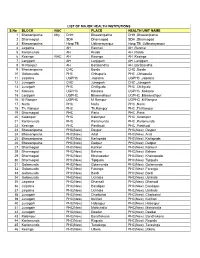
LIST of MAJOR HEALTH INSTITUTIONS S.No BLOCK NAC
LIST OF MAJOR HEALTH INSTITUTIONS S.No BLOCK NAC PLACE HEALTH UNIT NAME 1 Bhawanipatna Mty DHH Bhawanipatna DHH ,Bhawanipatna 2 Dharmagad SDH Dharmagad SDH ,Dharmagad 3 Bhawanipatna Hosp TB Uditnarayanpur Hosp TB ,Uditnarayanpur 4 Jaipatna AH Ranmal AH ,Ranmal 5 Karlamunda AH Risida AH ,Risida 6 Kesinga NAC AH Kesinga AH ,Kesinga 7 Lanjigarh AH Lanjigarh AH ,Lanjigarh 8 M Rampur AH Barabandha AH ,Barabandha 9 Bhawanipatna CHC Borda CHC ,Borda 10 Golamunda PHC Chhapuria PHC ,Chhapuria 11 Jaipatna UGPHC Jaipatna UGPHC ,Jaipatna 12 Junagarh CHC Junagarh CHC ,Junagarh 13 Junagarh PHC Chilliguda PHC ,Chiliguda 14 Koksara UGPHC Koksara UGPHC ,Koksara 15 Lanjigarh UGPHC Biswanathpur UGPHC ,Biswanathpur 16 M Rampur UGPHC M.Rampur UGPHC ,M.Rampur 17 Narla PHC Narla PHC ,Narla 18 Th. Rampur PHC Th.Rampur PHC ,Th.Rampur 19 Dharmagad PHC Parla PHC ,Parla 20 Kalampur PHC Kalampur PHC ,Kalampur 21 Karlamunda PHC Karlamunda PHC ,Karlamunda 22 Kesinga PHC Pastikudi PHC ,Pastikudi 23 Bhawanipatna PHC(New) Deypur PHC(New) ,Deypur 24 Bhawanipatna PHC(New) Artal PHC(New) ,Artal 25 Bhawanipatna PHC(New) Karlapada PHC(New) ,Karlapada 26 Bhawanipatna PHC(New) Dadpur PHC(New) ,Dadpur 27 Dharmagad PHC(New) Kankeri PHC(New) ,Kankeri 28 Dharmagad PHC(New) Behera PHC(New) ,Behera 29 Dharmagad PHC(New) Khairapadar PHC(New) ,Khairapadar 30 Dharmagad PHC(New) Tipiguda PHC(New) ,Tipiguda 31 Golamunda PHC(New) Golamunda PHC(New) ,Golamunda 32 Golamunda PHC(New) Faranga PHC(New) ,Faranga 33 Golamunda PHC(New) Bordi PHC(New) ,Bordi 34 Golamunda PHC(New) Uchhala PHC(New) -

Ground Water Year Book 2016-2017
Government of India CENTRAL GROUND WATER BOARD Ministry of Water Resources & Ganga Rejuvenation GROUND WATER YEAR BOOK 2016-2017 South Eastern Region Bhubaneswar September 2017 F O R E W O R D Groundwater is a major natural replenishable resource to meet the water requirement for irrigation, domestic and industrial needs. It plays a key role in the agrarian economy of the state. Though richly endowed with various natural resources, the state of Orissa has a long way to go before it can call itself developed. Being heavily dependent on rain fed agriculture; the state is very often exposed to vagaries of monsoon like flood and drought. The importance of groundwater in mitigating the intermittent drought condition of a rain-fed economy cannot be overemphasized. To monitor the effect caused by indiscriminate use of this precious resource on groundwater regime, Central Ground Water Board, South Eastern Region, Bhubaneswar has established about 1606 National Hydrograph Network Stations (NHNS) (open / dug wells) and 89 purpose built piezometres under Hydrology Project in the state of Orissa. The water levels are being monitored four times a year. Besides, to study the change in chemical quality of groundwater in time and space, the water samples from these NHNS are being collected once a year (Pre-monsoon) and analysed in the Water Quality Laboratory of the Region. The data of both water level and chemical analysis are being stored in computers using industry standard Relational Database Management System (RDBMS) like Oracle and MS SQL Server. This is very essential for easy retrieval and long-term sustainability of data. -

Information Sheet of District Education Office, Kalahandi
1 INFORMATION SHEET OF DISTRICT EDUCATION OFFICE, KALAHANDI Date of Creation : 14.08.1975 (Inspector of Schools) (From 13.02.2012 as District Education Officer) 1. NO OF HIGH SCHOOLS IN KALAHANDI:- GOVERNMENT HIGH SCHOOL 173 FULLY AIDED HIGH SCHOOL 21 BLOCK GRANT HIGH SCHOOL 94 PROJECT MANAGED HIGH SCHOOL(MUKHIGUDA) 01 RECOGNISED UN-AIDED HIGH SCHOOL 36 INCLUDING SHISHU MANDIR+BLIND SCHOOL GOVT.SSD HIGH SCHOOL 17 TOTAL 342 2. H.S.C EXAMINATION RESULT FOR LAST 5 YEARS:- NO OF NO FO POSITION IN YEAR STUDENT STUDENT % OF PASS THE STATE APPEARED PASSED 2013 18883 14181 76.00 16th 2014 19202 16580 86.77 4th 2015 20493 17968 87.97 5th 2016 22176 19972 90.35 7th 2017 22659 19699 87.20 18th 3. VACANCY POSITION IN GOVT.HIGH SCHOOLS:- AS ON 19.03.2018 Vacancy position in High School Men in Sanctioned Post Position Sl. Category of Post including Vacancy No. Regular & Regular Contractual Total Contractual 1 OES-II HM 3 0 3 3 0 2 Sr.SES HM 79 0 79 49 30 3 TGT Arts 388 0 388 348 40 4 TGT PCM 196 0 196 157 39 5 TGT CBZ 185 0 185 146 39 6 Classical Tr. 163 0 163 146 17 7 Hindi Tr. 156 0 156 89 67 8 PET 157 0 157 140 17 2 4. DISTRIBUTION OF FREE BI-CYCLE SCHEME-2017-18: All the students reading in class-IX of all Govt./Govt.SSD/Aided and Block Grant High School of Kalahandi District were paid Rs.2600/- each through account transfer. -

District Industrial Potentiality Survey Report Kalahandi 2019-20
District Industrial Potentiality Survey Report Kalahandi 2019-20 MSME Development Institute Vikash Sadan, College Square, Cuttack Odisha-753003 Telephone: 0671- 2950011, Fax: 2201006 E. Mail: [email protected] Website: www.msmedicuttack.gov.in i Contents Sl. No. Chapters Subject Page No. 1. Chapter-I Introduction 1-2 2. Chapter-II Executive Summary 3-4 3. Chapter-III District at a Glance 5-7 4. Chapter-IV District Profile 8-11 5. Chapter-V Resource Analysis 12-29 6. Chapter-VI Infrastructure Available for Industrial 30-38 Development 7. Chapter-VII Present Industrial Structure 39-45 8. Chapter-VIII Prospects of Industrial Development 46-49 9. Chapter- IX Plan of Action for promoting Industrial 50-52 Development in the District 10. Chapter- X Steps to set up MSMEs 53-54 11. Chapter- XI Conclusion 55 12. Annexure Policies of the State Government 56-71 ii List of Acronyms AHVS Animal Husbandry & Veterinary Services APEDA Agricultural & Processed Food Products Export Development Authority APICOL Agricultural Promotion & Investment Corporation of Odisha Limited CD Credit Deposit CFC Common Facility Centre CHC Community Health Centre DEPM Directorate of Export Promotion & Marketing DES Directorate of Economics & Statistics DIC District Industries Centre DTET Directorate of Technical Education & Training EDP Entrepreneurship Development Programme ESDP Entrepreneurship Skill Development Programme FIEO Federation of Indian Export Organizations Ha Hectare IDCO Odisha Industrial Infrastructure Development Corporation IMC Industrial Motivation Campaign IPICOL Industrial Promotion & Investment Corporation of Odisha Limited IPR Intellectual Property Rights IT Information Technology KVIB Khadi & Village Industries Board KVIC Khadi & Village Industries Commission MHU Mobile Health Unit MPEDA Marine Products Export Development Authority MT Metric Tonne MARKFED Odisha State Co-Operative Marketing Federation Ltd. -

Seba Jagat Covid -19 Response Program
SEBA JAGAT COVID -19 RESPONSE PROGRAM Context: As the outbreak of the novel corona virus there is growing anxiety about the potential dire consequences of the virus on countries with weaker health systems and within a country like India as well in our project areas in Western Odisha which have poor access to health services , inadequate health personnel, poor logistic and poor nutritional status/livelihood etc . What Seba Jagat has done so far with limited resource: Co-ordination with other NGO and district administration through whatsapp group “Kalahandi NGO-COVID-19 “ and using other media to learn the issues with the active guidance of the Collector,Kld ,NGO Nodal Officer and UNICEF . Awareness for Migrant people through watsapp groups “ Kalahandi Migrants-COVID-19” and Nuapada Migrants-COVID-19 in two Blocks i.e M.Rampur and Sinapali Block with direct monitoring by BDO of respective Block. Supporting the Police dept with awareness Placards with positive message on COVID-19 in four Blocks (i.e, M.Rampur,Lanjigarh, Narla and Karlamunda Block) . Distribution of 4000 Mask to the community people including ,migrant workers/MGNREGA workers ,MGNREGA workers and People with disable etc in five Blocks (i.e, M.Rampur,Lanjigarh,Golamunda,Narla and Karlamunda Block).. Community level awareness and sensitisation on COVID-19 ,Hand washing etc through door to door visit ,small group training /counseling with keeping distance , Flash Banner in different points including Rly Station ,G.P points ,PHC(N) etc Social distance maintaining at community -
Xo Ba4 R CSO-Cum-District Manager, OSCSC Ltd
t. \ Annexure-ll ) CSO.CUM.DISTRICT MANAG ER, ODISHA STATE CIVIL SUPPLIES CORPORATION LIMITED, KALAHANDI. COLLECTORATE, FS & CW SECTION, KALAHAND! www.kalahandi.nic.in (Website of Kalahpndj) xo bA4 r CSO-cum-District Manager, OSCSC Ltd. Kalahandi invites sealed tenders from reputed firms / companies / persons for appointment as Level-ll Transport Contractor for transportation of foodgrains from Rice Receiving Centre-Cum- Departmental Storage Centre (RRC-cum-DSC) to Retail Centres of Unit tagged. The Level-ll Transport Contractor shall perform all operations for transportation of foodgrains from RRC-cum-DSC to retail centres & delivering the foodgrains at Retail Centres of Unit tagged. lnterested firms/ companies/ persons may obtain tender document from the office of the CSO-cum-District Manager from 23.02J9to 15.03.19 up to 3.00 PM. The interested firms/ companies/ persons may also download the tender document from the district website www.kalahandi.nic'in. lnterested firms/ companies/ persons wiil have to submit the tender documents through reqistered post/ speed post/ courier service only as per the procedure prescribed in the tender document to the following address. Tender document sent other than the above mode shall not be entertained in any circumstances. The Corporation shall not be responsible for any postal/ courier delay. Tender paper received after the schedule date &time shall not be considered Address for submission of Tender document: District Manager, OSCSC Ltd, Kalahandi, AUPo-Bhawanipatna, District- Kalahandi, PrN- 766001 Period of sale of tender document 23.02.19 to 15.03.19 up to 3 PM Last date for receipt of tender document 15.03.2019 up to 5 PM Date of opening of Technical Bid 16.03.19 at 11 AM Date of opening of Price Bid 19.03.19 at 11 AM GSO-cum ager,-6$N OSCSC l-- \ ) Annexure-lII TENDER PAPER (Ievel-TI Transoort Contractor) OFF'ICE OF THE DISTRICT MANAGER ODISHA STATE CIVIL SUPPLIES CORPORATION LIMITED KALAHANDI.